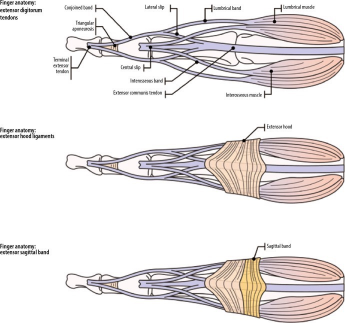
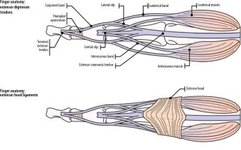
This article is prohibited from being reproduced without authorization.Following the previous article: Latest review: Various traumatic anatomy and MRI reading techniques of the wrist, packed with useful information!AbstractThe anatomy of the wrist and hand is complex, containing many small structures. Magnetic Resonance Imaging (MRI) is the ideal imaging modality for assessing various traumatic and pathological conditions in this area and is often performed after X-ray imaging. In this article, we describe the normal anatomy, imaging techniques, and MRI findings of various traumatic and pathological conditions of the wrist and hand, including occult fractures, osteonecrosis, ligament and tendon injuries, and compressive neuropathies.MRI of the Little Finger01 AnatomyEach finger consists of metacarpals, proximal phalanges, middle phalanges, and distal phalanges. The metacarpals connect to the proximal row of carpal bones to form the CMC joint. Distally, the metacarpals connect to the proximal phalanges to form the MCP joint. The proximal phalanges and middle phalanges of each finger hinge to form the proximal interphalangeal joint (PIP). The middle phalanges and distal phalanges of each finger form the distal interphalangeal joint (DIP).The primary stabilizing ligaments around the little finger MCP and interphalangeal (IP) joints are the radial and ulnar collateral ligaments, as well as the palmar plate, which is a fibrocartilaginous thickening of the joint capsule. Each palmar plate attaches to the collateral ligaments, and the sagittal bands and deep transverse metacarpal ligaments at the MCP joint.The extensor tendons of the little finger are formed by a combination of extrinsic and intrinsic tendons (Figure 26). The extrinsic tendons originate from the forearm, innervated by the posterior interosseous nerve, consisting of the Extensor Digitorum Communis (EDC), Extensor Indicis Proprius (EIP), and Extensor Digiti Minimi (EDM). The EDC and EIP tendons pass through the fourth extensor compartment, while the EDM tendon traverses the fifth extensor compartment. Only about half of people have a distinct fifth finger EDC tendon. The EIP tendon typically inserts into the EDC tendon of the second finger, while the EDM tendon moves to the fifth finger. Extensor tendons can be either extrinsic or intrinsic. There are anatomical variations of the extrinsic tendons that extend the little finger at the MCP, PIP, and DIP. The intrinsic extensor tendons are primarily formed by the interossei. The abductor digiti minimi is an exception, forming the ulnar lateral band of the fifth finger. The intrinsic tendons enter the fingers as the medial and lateral bands.
Figure 26. Schematic diagram of finger extensors, including tendons, extensor hood ligaments, and extensor sagittal bands.Between the MCP and PIP joints of each finger, the extensor tendons split into three bundles of ligaments, namely the central band, radial side band, and ulnar side band. The central band inserts at the base of the middle phalanx. The lateral bands combine with their respective lumbricals to insert at the PIP joint and form the terminal tendons. These terminal tendons merge in the distal interphalangeal joint area and insert as the terminal tendons at the base of the distal phalanx (Figure 26). The distal terminal tendons are connected by the triangular ligament.The extensor hood is primarily located on the dorsal side of each little finger’s proximal interphalangeal joint, stabilizing the extensor tendons and preventing abnormal lateral movement. Additionally, the radial and ulnar sagittal bands are located at the level of each little finger’s MCP joint (Figures 26 and 27). They extend around the joint from the extensor hood to the palmar plate, stabilizing the extensor tendons at the level of the MCP joint.
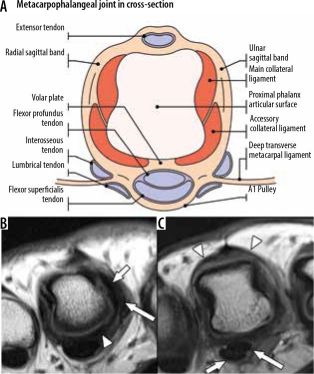
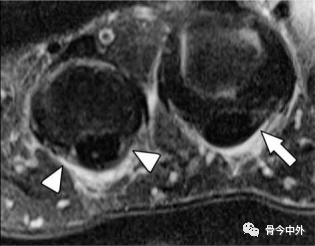
Figure 27. Normal anatomy of the metacarpophalangeal joint. A) A transverse section of one little finger at the level of the metacarpal head and MCP joint shows the position of the palmar plate, collateral ligaments, and flexor and extensor tendons. B) Axial proton density (PD) non-fat-suppressed (NFS) magnetic resonance (MR) image of a 42-year-old female shows thickening of the palmar plate (arrow) fibrocartilage. The radial main ligament (short arrow) and collateral ligaments (long arrow) are clearly displayed. C) On the same finger, a slightly proximal axial PD-NFS MR image shows the centrally located EDC tendon alongside the adjacent radial and ulnar sagittal bands (arrow). The palmar side also shows the flexor digitorum superficialis and flexor digitorum profundus tendons (short arrow and long arrow, respectively).The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons constitute the flexor mechanism of the little finger. The FDS muscle originates from the forearm, innervated by the median nerve, and flexes the MCP and PIP joints of the wrist. The FDP muscle also originates from the forearm, innervated by the median and ulnar nerves, and flexes the MCP and IP joints of the wrist. The FDS is located on the surface of each little finger’s FDP, inserting at the level of the proximal phalanx. The FDS splits into two distinct sliding tendons at the base of each little finger’s proximal phalanx, which then pass through and ultimately delve into the FDP tendon at the level of the PIP joint (Figure 28). Just proximal to the insertion point of the FDS, fibers from each sliding tendon extend to the other end, known as the Camper’s cross. The separation of the FDS tendon provides a channel for the FDP tendon to continue distally in the finger and insert into the palmar plate and the base of the distal phalanx at the DIP joint.The flexor tendons are surrounded by a digital sheath from the palm to the distal joints. Small arteries nourish the flexor tendons, which are usually not visible on conventional MRI. Local regions of thickening of the digital sheath form a pulley system to secure the flexor tendons to the adjacent bones during finger movements. Although the three cruciate (C) pulleys are poorly visualized on MRI, the five annular (A) pulleys are commonly seen, especially in axial views, and are numbered according to their positions. The A1, A3, and A5 pulleys are located at the levels of the MCP, PIP, and distal joints, respectively, and connect to the palmar plate. The A2 pulley attaches to the bone membrane of the proximal phalanx, and the A4 pulley attaches to the bone membrane of the middle phalanx (Figure 28).
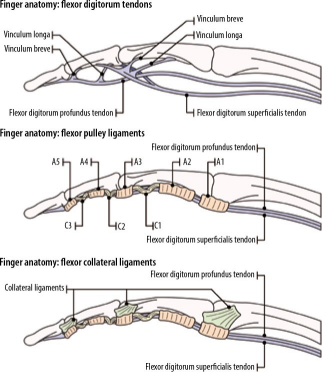
Figure 28. Schematic diagram of finger flexor anatomy, including tendons, annular pulleys, and cruciate pulleys.02 Disruptions within the Little Finger Joints>> Bones and JointsBones and joints are typically assessed for contusions, fractures, malalignment, dislocations, or joint effusions. For fractures involving joint surfaces, the extent of involvement should be quantified, as it can serve as an indicator of joint stability. Any fracture displacement, including the size of any bone fragments, should also be described. The integrity of the cartilage and degenerative or inflammatory joint disease also needs to be assessed. X-rays are often helpful in this evaluation. Additionally, in cases of injury, the soft tissues of the little finger should be evaluated for the presence of hematoma, effusion, or edema.>> Ligaments and Palmar PlateOn MRI, edema around the ligaments and palmar plate typically indicates acute injury to that structure. Additionally, the presence of partial or full-thickness tears should be assessed. The location of any tears, as well as any bone/periosteum involvement, should be described. Ligament injuries most commonly affect the PIP joint, and dorsal dislocations can lead to tears of the palmar plate. Any radiological evidence of ligament/palmar plate displacement or collapse should be described in the report to aid clinical management.>> Extensor MechanismExtensor injuries are typically classified according to their anatomical locations. The Verdan system is the most commonly used, consisting of eight regions (Figure 20). Odd-numbered regions are located at the high position of the joints. The report should detail the site of the injury, the percentage of tendon involvement, and any adjacent bone or soft tissue involvement.Injury to region 1 is the most common and is usually closed. They occur at the level of the distal tendons and often occur when the fingers are extended, while forcefully bending the joints can result in avulsion injuries, referred to as mallet fingers. Avulsion fractures at the dorsal base of the distal phalanx may occur. Treatment for region 1 injuries typically involves splinting the finger to keep the distal joints extended.Region 2 injuries are typically caused by lacerations and occur at the level of the middle phalanx. These injuries usually involve the terminal tendons or triangular ligaments. An injury to a terminal tendon typically undergoes conservative treatment. If the injury involves the triangular ligament or two tendons, surgical repair is typically required.Region 3 injuries can be open or closed and occur at the level of the PIP joint. Closed injuries typically refer to those caused by a blow to the back of the finger, forceful flexion at the joint, or palmar joint dislocation. These injuries may involve distal central tendon dislocations and may be accompanied by avulsion injuries at the dorsal base of the middle phalanx, but can also involve the lateral bands. Many injuries can be treated conservatively, such as splinting or skin traction. However, open injuries, displaced avulsion fragments, and instability may require surgical treatment. Region 4 injuries at the level of the proximal phalanx are often caused by lacerations and can involve the central band, lateral bands, medial and lateral lumbricals, and extensor hood. Due to the wider extensor tendons in this region, most injuries are partial tears without significant retraction. Injuries in this region are typically treated conservatively, such as splinting with skin traction. More severe injuries typically require surgical treatment.MCP joint surface region 5 injuries commonly occur at the flexion of the index finger MCP joint. These injuries are usually due to a clenching mechanism, involving complete or partial tears of the extensor tendons. The sagittal bands and joint capsule may also be involved (Figure 29). Oblique injuries involving the sagittal bands can be open but are more commonly closed. They may lead to subluxation or dislocation of the extensor tendons, often resulting in a sensation of snapping in the patient. If the joint capsule is involved, open injuries can lead to infections, including suppurative arthritis. Region 5 injuries typically require surgical repair.
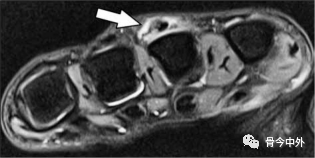
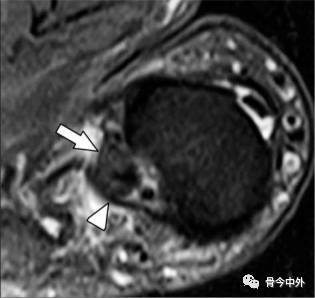
Figure 29. Rupture of the Extensor Digitorum Communis (EDC) tendon in extensor tendon region 5 with rupture of the ulnar sagittal band. A 37-year-old female, with dorsal pain and swelling of the left third MCP joint, axial T2W fat-suppressed MR image shows partial rupture of the EDC tendon, with tendon thickening. This is associated with a localized tear when the ulnar sagittal band attaches to the tendon (arrow).Back of the hand region 6 injuries are typically caused by lacerations. The extensor tendons in this area are very superficial. A single injury can involve multiple extensor tendons. Clinical examination may not reveal significant limitations in extension due to inter-tendon connections leading to single tendon or partial tendon ruptures. Surgical repair is required.>> Flexor MechanismMagnetic Resonance Imaging is useful for assessing flexor tendon injuries. T2W sequences typically show fluid signal in the recently torn area. Important imaging findings include whether the tear is partial thickness (estimated cross-sectional percentage of tendon involvement) or full thickness. The location of the tear and any tendon retraction should be clearly described, including the presence of any bone avulsions and any fragment displacements.Kleinert, Verdan, and others classify flexor tendon injuries into five anatomical regions (Figure 20). Flexor tendon injuries are mostly open injuries and are often lacerations. Less common are closed injuries associated with avulsions. The most common type of closed avulsion injury is the distal FDP tendon tear. This is usually caused by forced extension of the distal joint during activities such as football or rugby, most commonly involving the ring finger. Leddy and Packer initially classified these injuries into three main types, later describing other types. Type I injuries occur when the tendon contracts the palm. Type II injuries occur when the tendon retracts to the level of the skin joints. Type III injuries occur with avulsed bone fragments, with the fragments fixed by the A4 pulley. Type IV injuries occur with bone fragments, but the tendon has been avulsed from the fragments. These injuries often require surgical repair, with Type I injuries often becoming urgent due to compromised blood supply. Isolated FDS avulsion injuries are rare, and FDS injuries usually occur concurrently with FDP injuries.Flexor tendon ruptures typically occur in the mid-portion rather than at the origin and insertion points and are classified according to their location in the regions described by Kleinert, Verdan, and others (Figure 30). Injuries in regions 2 to 5 may involve neurovascular bundles and require urgent surgical intervention. Region 2 injuries are the most common and have the highest complication rates. Although traditional Region 2 injuries have not been surgically repaired due to high complication rates, advances in understanding these injuries and surgical techniques have allowed for surgical repair of these injuries. In current practice, the best surgical repair time for these injuries is within 24 hours.
Figure 30. Type I distal flexor digitorum profundus (FDP) tendon rupture. A 23-year-old male, axial T2W MR fat-suppressed image shows a complete rupture of the distal FDP tendon at the insertion point of the flexor digitorum superficialis (arrow), with a tendon gap of 1.1 cm.Injuries to the annular pulleys are most clearly shown on axial imaging (Figure 31). Rock climbing is a common cause of pulley injuries, most commonly the A2 pulley of the ring finger. Tears can be partial or complete, and may involve single or multiple pulley tears. The result of pulley tears is a bowstring phenomenon of the flexor tendons, depending on the number of pulley tears and the position of the finger. Comparing the flexor mechanisms of adjacent fingers can help assess subtle bowstring MRI findings. In cases of acute injury, fluid signals are often seen around the annular pulleys. Klauser et al. examined the degree of displacement of flexor tendons from the palmar surface of the proximal phalanx at rest in excellent climbers using MRI and ultrasound [the distance from the tendon to the phalanx (TP)] and the situation when the finger is forcibly bent. They observed that a TP distance greater than 1.0 mm is a sign of pulley dysfunction and at least partial tears, while an increase in the displacement of the palmar tendons of at least 1.0 mm when the finger is forcibly bent is also a sign of at least partial tears. In cases of forced flexion of the fingers, a TP distance greater than 2.5 mm may assist in diagnosing complete tears of the A2 or A4 pulleys.
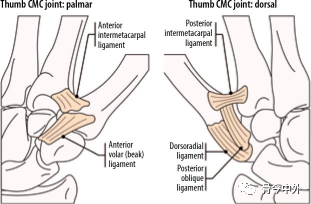
Figure 31. A1 flexor tendon pulley injury. A 59-year-old female, with low-energy trauma to the middle and ring fingers, axial T2W fat-suppressed MR image shows mild thickening, intermediate signal, and surrounding edema of the A1 pulley (arrow). Mild edema is present around the middle finger. However, the pulley fibers appear intact, with uniform thickness and low signal (short arrow).MRI of the Thumb01 Thumb AnatomyThe thumb consists of the proximal and distal phalanges, the first metacarpal, and the CMC joint, with multiple carpal joints including its articulation with the scaphoid, trapezium, and the bases of the first and second metacarpals.The first CMC joint is a double-concave saddle joint located between the trapezium and the base of the first metacarpal, allowing for a significant range of motion, including internal rotation, flexion, external rotation, abduction/adduction, and external rotation (rotational movements). It is statically stabilized by many ligaments (Figure 32). Historically, the most important is the anterior oblique ligament (AOL or beak ligament), which is a palmar structure located between the tubercle of the trapezium and the ulnar side of the first metacarpal base. It consists of deep and superficial bands and is the primary restraint against dorsal dislocation of the first metacarpal. Other dorsal ligaments include the posterior oblique ligament, dorsal ligament (DRL), intercarpal ligaments, and ulnar collateral ligament (UCL) (Figure 33). Recent evidence suggests that these ligaments, particularly the DRL, which is the thickest and strongest of the dorsal ligaments, also play a key role in preventing dorsal dislocation of the first metacarpal.
Figure 32. Schematic diagram of the palmar and dorsal ligaments of the first carpometacarpal joint.
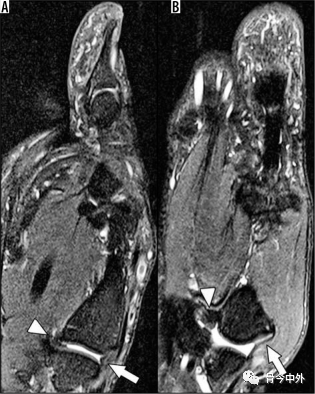
Figure 33. Normal anatomy of the first carpometacarpal ligament in a 36-year-old male. A) Sagittal T2W fat-suppressed (FS) MR image of the thumb shows normal anterior oblique ligament and dorsal ligament (long arrow and short arrow, respectively), which help stabilize the thumb and prevent dorsal/palmar dislocation. B) Coronal T2W FS MR image shows normal intercarpal ligaments (long arrow) and ulnar collateral ligament (short arrow).The first MCP joint is a double-joint joint characterized by features of a condylar (ellipsoidal) joint and a hinge (ginglymus) joint, allowing for a greater range of motion than typical hinge joints. The MCP joint capsule is partially composed of fibrocartilage, which thickens on the dorsal and palmar sides, forming the dorsal and palmar plates, respectively. On MRI, normal dorsal and palmar plates appear as triangular low-signal structures on sagittal imaging. Typically, there are two palmar sesamoid bones surrounded by the palmar plates, which attach to the metacarpal head and the base of the proximal phalanx, helping to stabilize the flexor pollicis longus tendon. Additionally, there is typically a small joint recess between the base of the proximal phalanx and the palmar plate. The radial and ulnar collateral ligaments resist varus and valgus forces, respectively. They consist of an intrinsic ligament from the dorsal head of the metacarpal to the base of the proximal phalanx and an extrinsic ligament from the metacarpal head to the palmar plate and sesamoid bones (Figure 34). The ligaments tighten during flexion and loosen during extension. Importantly, the adductor tendon membrane originates from the adductor pollicis, extending superficially to the UCL, attaching to the proximal axis of the proximal phalanx.
Figure 34. Normal metacarpophalangeal ligaments of the thumb. A) Coronal T2W fat-suppressed (FS) MR image of the thumb MCP joint of a 38-year-old male shows normal ulnar collateral ligament (UCL, long arrow) and radial collateral ligament (short arrow) morphology. The ligaments are smooth, attaching to the metacarpal and proximal phalanx, with low signal and no surrounding soft tissue or bone marrow edema. Normal collateral ligaments of the thumb interphalangeal joint can also be observed. B) Axial T2W FS MR image of the same patient shows the position of the main UCL and collateral ligaments (long arrow and short arrow, respectively).Finally, the IP joint is a true hinge joint, allowing for flexion and extension. Similar to the thumb MCP joint, the IP joint has dorsal and palmar plates composed of fibrocartilage. Because it allows for minimal mobility, it is the most stable of these joints and the least prone to injury.The flexor and extensor tendons dynamically stabilize the thumb and facilitate its movement. The flexor pollicis longus tendon originates from the forearm, traverses the radial side through the carpal tunnel to the palmar side of the thumb, located between the sesamoid bones on the palmar plate of the MCP joint. It inserts at the base of the distal phalanx and flexes the IP and MCP joints (Figure 35). The thumb pulleys help stabilize the tendons and connect them to the palmar surfaces of the MCP joint, proximal phalanx, and IP joint. Unlike the little finger, the thumb has only one pulley. The A1 pulley is located at the MCP joint, and the A2 pulley is located at the IP joint. An oblique ring pulley (Ao) is located at the level of the proximal phalanx. In about 93% of cadaver specimens, there is also a variable pulley (Av) between the A1 and Ao pulleys. The radial side of the pulley is slightly longer, and the tendons are usually located on the ulnar side of the joint midline. Two extensor compartments in the wrist are used for abduction and extension of the thumb. The first extensor compartment originates from the radial edge of the first metacarpal, mainly inserting into the flexor pollicis longus tendon and inserting at the base of the proximal phalanx or the dorsal first MCP joint capsule of the flexor pollicis brevis tendon. On the other hand, the third extensor compartment consists solely of the flexor pollicis longus, which inserts at the dorsal base of the distal phalanx and allows for IP joint extension. This tendon is stabilized by the extensor hood at the MCP joint, which has radial and ulnar sagittal bands, along with a slightly distal triangular expansion that extends distally to insert at the base of the distal phalanx.
Figure 35. Normal tendon and pulley anatomy of the thumb. A) Schematic diagram of the dorsal flexor tendon of the thumb, showing the attachment points of the tendons and extensors. B) Schematic diagram of the palmar side of the thumb showing the flexor pollicis longus tendon pulley and the adductor. C) An axial T1W fat-suppressed MR image of a 38-year-old male shows a thin fibrous band at the level of the proximal phalanx, covering the flexor pollicis longus tendon. Due to the radial side of the pulley being longer, the tendon is slightly positioned towards the ulnar side (long arrow).02 MRI of Joint Disruptions in the Thumb>> First CMC JointAcute ligament injuries of the thumb can occur, but are less common than acute ligament injuries of the MCP joint. The most common intra-articular disruption in this area is osteoarthritis. This is typically related to repetitive movements associated with ligament laxity, such as pinching or a single traumatic event. The incidence of first-time CMC osteoarthritis is higher in females, related to hormonal influences. X-rays are the primary means of evaluating osteoarthritis, but MRI is helpful for detecting ligament injuries, such as AOL injuries, which may lead to joint instability. Additionally, MRI often detects signs of osteoarthritis earlier than X-rays. Finally, MRI can be used to look for other causes of radial-sided pain, such as DeQuervain’s tenosynovitis or radiologically occult fractures. Typical MRI findings include synovial proliferation and effusion, cartilage loss, bone marrow edema with subchondral cyst-like changes, and marginal osteophytes. Thickening of the stabilizing ligaments, with intermediate signal, suggests chronic scarring and degenerative changes. As with acute ligament injuries in other locations, MRI findings include thickening of the ligaments and intermediate/enhanced signals, accompanied by surrounding ligament edema, and fluid signal intensity gaps within the ligaments or at their bony attachments, indicating partial or complete tears.>> First MCP JointUCL injuries are typically associated with excessive stretching of the thumb, especially when falling and grabbing something (like ski poles). Therefore, this condition is often referred to as skier’s thumb. The term “gamekeeper’s thumb” has been used synonymously, although it typically refers to chronic injuries, while skier’s thumb is reserved for more severe injuries. UCL tears most commonly occur at the distal attachment of the proximal phalanx and may be associated with avulsion injuries; however, they can also occur proximally, near the metacarpal head, or in the middle substance. When the distal UCL tears, a narrow lesion occurs between the UCL remnant and the base of the proximal phalanx. This impairs the healing of the UCL, leading to joint instability and osteoarthritis.MRI is very helpful for the diagnosis and characterization of UCL injuries. The sensitivity for diagnosing UCL tears is reported to be 96%, with a specificity of 95%. UCL injuries can be classified into acute and chronic injuries, with differing MRI findings. In acute UCL injuries, significant edema typically appears on fluid-sensitive sequences. The ligament may thicken, have indistinct margins, and contain internal intermediate signals. When there are fluid signal gaps within the ligament or at its bony attachment, it is diagnosed as a complete tear, and may be associated with avulsion fractures of varying degrees of bone marrow edema (Figure 36). If the displaced bone fragments exceed 5 mm, or if it involves more than 25% of the joint surface, surgical treatment is required.
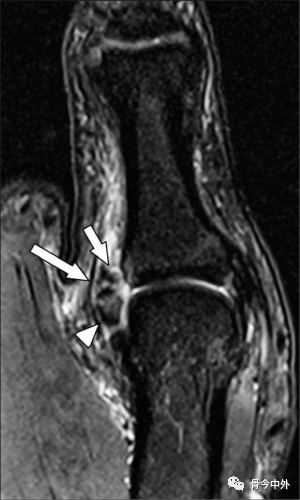
Figure 36. A 26-year-old male professional baseball player injured his thumb while sliding into a base, resulting in a bony avulsion injury of the ulnar collateral ligament (UCL) of the first metacarpophalangeal (MCP) joint. The coronal T2W fat-suppressed MR image at the thumb MCP joint shows avulsion of the UCL from the base of the proximal phalanx (arrow), with mild bone marrow edema at the base of the proximal phalanx, and a fluid gap between the torn ligament and the proximal phalanx (short arrow). However, no narrow lesion is seen, and the adductor tendon membrane covers the torn UCL (long arrow).In chronic injuries, soft tissue and bone marrow edema typically resolve, and the ligaments may show thickening and irregularity, reflecting chronic scarring. There may be gaps between the bone and the ligament remnants, and the ligament remnants may retract into a rounded shape. In these cases, the adductor tendon membrane may extend into the UCL remnants, forming the typical “yo-yo” appearance described in Stener lesions (Figure 37). In this finding, the string represents the tendon membrane, while the yo-yo is the thickened ligament remnant. Some authors have noted that intact collateral ligaments or sesamoid ligaments may prevent the development of narrow lesions. MRI may help assess the integrity of these structures to determine whether the patient is prone to narrow lesions.
Figure 37. A 39-year-old female with a left thumb abduction injury, resulting in a bony avulsion of the ulnar collateral ligament (UCL) of the first metacarpophalangeal (MCP) joint with a narrow lesion. A) Coronal T1W fat-suppressed (FS) gradient echo MR image of the MCP joint shows a displaced bone fragment on the ulnar side at the base of the proximal phalanx (arrow), with a displacement of 6 mm. This is an indication for surgical repair. B) The same area on the coronal T2W FS MR image shows a narrow lesion, resembling a “yo-yo on a string.” The short arrow indicates the adductor tendon membrane (string), and the long arrow indicates the retracted ligament and bone fragment (yo-yo).RCL injuries are much less common than UCL injuries. Although most injuries are low-grade sprains that can be treated with immobilization, high-grade partial and complete tears have been shown to contribute to joint instability, chronic ulnar deviation, and MCP osteoarthritis. Therefore, these injuries are typically treated with surgical intervention. Rare reports have indicated the presence of narrow lesions between the abductor tendon membrane and the RCL, which also require surgical intervention.>> Trigger Finger/ThumbTrigger finger/thumb can lead to painful clicking and restricted range of motion. This creates a digit that must be manually unlocked. It typically occurs in the fifth and sixth decades of life, more commonly in patients with diabetes. It is caused by the flexor tendon and pulley fibrocartilaginous metaplasia, usually occurring at the proximal edge of the A1 pulley. MRI can show tendon thickening and intermediate signals within the substance, indicating tendonopathy, and may have pulley thickening (Figure 38). When this occurs in the thumb, it may spontaneously resolve. Therefore, surgical indications are when the thumb is in a continuous triggering state.
Figure 38. Trigger thumb. A 65-year-old male with a clicking thumb and limited range of motion. Axial T2W fat-suppressed MR image at the level of the first metacarpophalangeal joint shows mild thickening of the flexor pollicis longus tendon, with intermediate signal (long arrow). Additionally, the A1 pulley is slightly thickened, with intermediate signal (short arrow).ConclusionMagnetic Resonance Imaging provides fine contrast and spatial resolution, allowing for accurate, non-invasive assessment of all musculoskeletal tissues of the wrist and hand. To generate diagnostic images in a reasonable time, patient positioning, selection of scanners and coils, and MRI parameters must be optimized, and imaging should be tailored to best resolve clinical issues. Newer MRI techniques, such as three-dimensional volumetric acquisition, improve image quality while speeding up imaging.The content of this article only represents the author’s personal views and does not represent the official position of Bone Today. We hope everyone will make rational judgments and apply them purposefully.