Abstract
Objective:
To explore the correlation between monocyte chemoattractant protein-1 (MCP-1) and its gene polymorphisms with diabetic peripheral neuropathy (DPN) in Han Chinese population in the coastal area of Zhejiang province.
Methods:
General data and blood samples were collected from 187 hospitalized type 2 diabetes patients in the endocrinology department of the First People’s Hospital of Wenling City from 2014 to 2017.
According to the diagnostic criteria for peripheral neuropathy in type 2 diabetes patients, the selected patients were divided into those with DPN (DPN group, n=95) and those without DPN (T2D group, n=92), alongside a healthy control group of 94 individuals (HC group, n=92).
Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to detect the gene polymorphism of MCP-1 (-2518A/G), and enzyme-linked immunosorbent assay (ELISA) was used to determine serum MCP-1 levels.
Results:
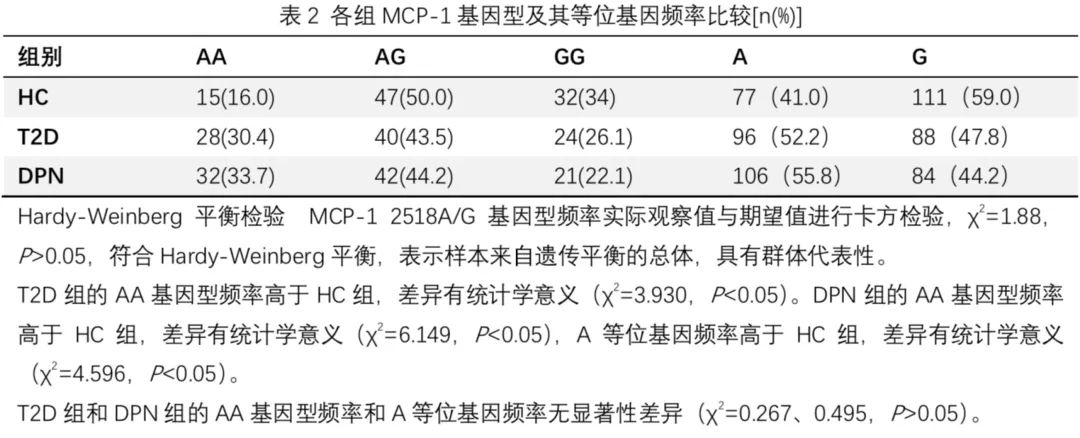
The frequency of the AA genotype in the T2D group was significantly higher than that in the HC group (p<0.05). The frequencies of the AA genotype and the A allele in the DPN group were also significantly higher than those in the HC group (p<0.05). No significant differences were found in the AA genotype frequency and A allele frequency between the T2D and DPN groups (p>0.05).
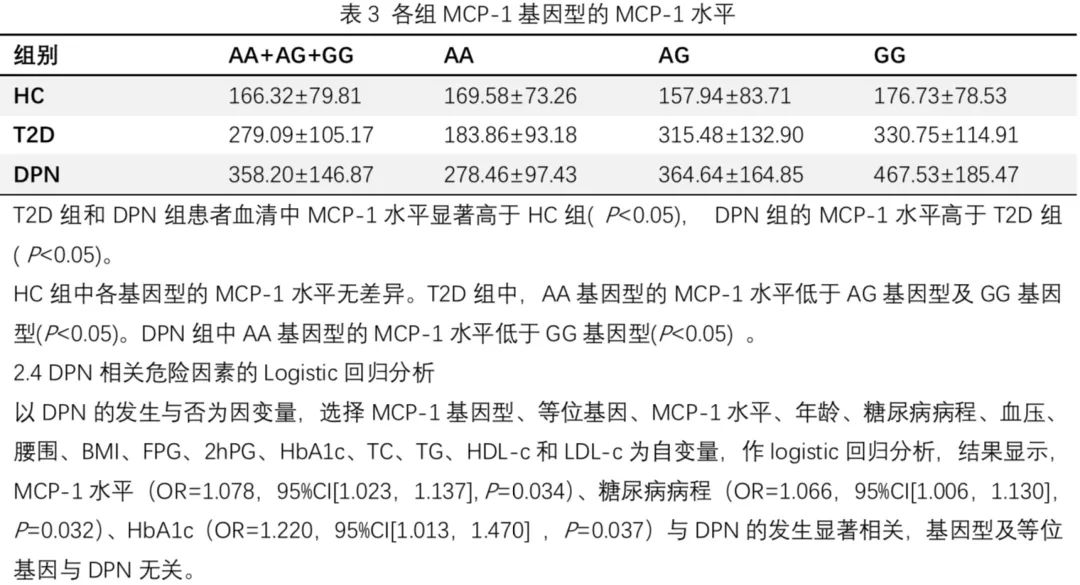
Serum MCP-1 levels in the T2D and DPN groups were significantly higher than those in the HC group (P<0.05), with the DPN group having higher MCP-1 levels than the T2D group (P<0.05). There was no difference in MCP-1 levels among the genotypes in the HC group. In the T2D group, the MCP-1 level in the AA genotype was lower than that in the AG and GG genotypes (P<0.05).
In the DPN group, the MCP-1 level in the AA genotype was lower than that in the GG genotype (P<0.05). Logistic regression analysis indicated that MCP-1 levels, diabetes duration, and HbA1c were significantly associated with the occurrence of DPN.
Conclusion:
Serum MCP-1 levels correlate with the occurrence of T2DM and DPN; the gene polymorphism of MCP-1 (-2518A/G) is associated with T2DM but not with the occurrence of DPN.
Keywords: Monocyte Chemoattractant Protein-1, Gene Polymorphism, Diabetic Peripheral Neuropathy
With the increasing number of type 2 diabetes cases, diabetes and its chronic complications have become a significant social burden.
Diabetic peripheral neuropathy is the most common and early-occurring chronic complication of diabetes, being a major cause of hospitalization and non-traumatic amputations [1,2].
The pathogenesis is related to various factors, including inflammatory factors, and there is evidence that genetic factors are also associated with the occurrence of diabetic peripheral neuropathy [3,4]. Monocyte Chemoattractant Protein-1 (MCP-1) belongs to the chemokine family and is an inflammatory factor that has a chemotactic effect on monocytes [5].
Current studies indicate that MCP-1 and its gene polymorphism at the -2518 site (A-2518G, rs1024611) affect serum MCP-1 levels and are associated with diabetes and its chronic complications like diabetic nephropathy, diabetic retinopathy, and diabetic foot disease, but there are fewer reports on its correlation with diabetic peripheral neuropathy [6-8].
This study aims to explore the correlation between MCP-1 and its A-2518G gene polymorphism with diabetic peripheral neuropathy.
1. Subjects and Methods
1.1 Subjects
A total of 187 type 2 diabetes patients hospitalized at the First People’s Hospital of Wenling City from 2014 to 2017 were evaluated, including 90 males and 97 females, aged 50-81 years, diagnosed according to the 1999 WHO standards for diabetes diagnosis and classification.
All subjects were Han Chinese from the Zhejiang region, with no blood relation among them, and excluded were type 1 diabetes patients, those with acute or chronic infectious diseases, severe cardiovascular and cerebrovascular diseases, pregnancy, autoimmune diseases, malignant tumors, and mental illnesses.
Data collected included age, sex, diabetes history and treatment history, other significant disease history, family history, height, weight, blood pressure, physical examination, and blood samples for glucose, glycosylated hemoglobin (HbA1c), C-peptide, total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL-c), and low-density lipoprotein (LDL-c) biochemical indicators.
All subjects underwent physical examinations and neurophysiological tests, including ankle reflex, vibration sense, 10g nylon monofilament, pinprick pain sensation, and temperature sensation, using an electromyography device (keypoint-p from Vidi Company).
According to the DPN diagnostic criteria from the 2013 Chinese guidelines for diabetes prevention and treatment:
(1) Clear history of diabetes;
(2) Neuropathy occurring at or after the diagnosis of diabetes;
(3) Clinical symptoms and signs consistent with DPN;
(4) For those with clinical symptoms (pain, numbness, sensory abnormalities, etc.), at least one abnormal finding in five tests (ankle reflex, pinprick pain, vibration sense, pressure sense, temperature sense); for those without clinical symptoms, at least two abnormalities among the five tests, clinically diagnosed as DPN.
Exclusion Criteria:
Other causes of neuropathy such as cervical and lumbar spondylosis, cerebral infarction, Guillain-Barré syndrome, severe vascular disease, and neuropathy caused by chemotherapy drugs or metabolic toxins due to renal insufficiency were excluded [9].
Type 2 diabetes patients were divided into a diabetic peripheral neuropathy group (DPN group, 95 cases) and a non-peripheral neuropathy group (T2D group, 92 cases). A healthy control group (HC group) of 94 individuals was selected, including 44 males and 50 females, aged 45-76 years, from the same hospital’s health examination population, all Han Chinese, confirmed by laboratory tests to have no diabetes, no history of cardiovascular, liver, and kidney diseases, and no family history of diabetes, with no significant differences in sex distribution and age among the three groups.
This study was approved by the ethics committee of the First People’s Hospital of Wenling City, and all participants provided informed consent.
1.2 Methods
Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to detect polymorphism.
DNA was extracted from peripheral blood leukocytes using QIAGEN’s DNA extraction kit as the template, with upstream primer sequence 5-CCGAGATGTTCCCAGCACAG -3’ and downstream primer sequence 5-CTGCTTTGCTTGTGCCTCTT -3’, yielding an amplification product size of 930bp.
Reaction Conditions: Pre-denaturation at 94℃ for 10 min, denaturation at 94℃ for 30s, annealing at 64℃ for 30s, extension at 72℃ for 30s, repeated for 40 cycles, and a final extension at 72℃ for 10 min. The PCR amplification products were subjected to enzyme digestion reactions with PvuII endonuclease (New England Biolabs), and the digested products were observed using 1.5% agarose gel electrophoresis and ethidium bromide staining under UV imaging.
Since the -2518G allele has a PvuII restriction site, the AA genotype has a 930bp digestion fragment, the AG genotype has fragments of 930, 708, and 222bp, and the GG genotype has fragments of 708 and 222bp.
Samples carrying different genotypes were sent to Yingweijie (Shanghai) Trading Co., Ltd. for sequencing, and results were compared with the digestion results. All subjects had 4 mL of fasting venous blood collected, treated with EDTA anticoagulant, and serum was obtained after centrifugation. Serum MCP-1 levels were measured using the enzyme-linked immunosorbent assay (ELISA) (R&D Company).
1.3 Statistical Analysis
SPSS 23.0 statistical software was used, and all measurement data conforming to a normal distribution were expressed as `x±s. The genotype distribution and gene frequency of each group were calculated, and Hardy-Weinberg equilibrium was tested to determine whether the genotype reached genetic equilibrium.
Comparisons among multiple groups were conducted using one-way ANOVA, and comparisons between two continuous variables used t-tests; categorical data were expressed as frequencies, and inter-group comparisons used the χ2 test. Risk factor analysis related to DPN was performed using logistic regression analysis.
Results
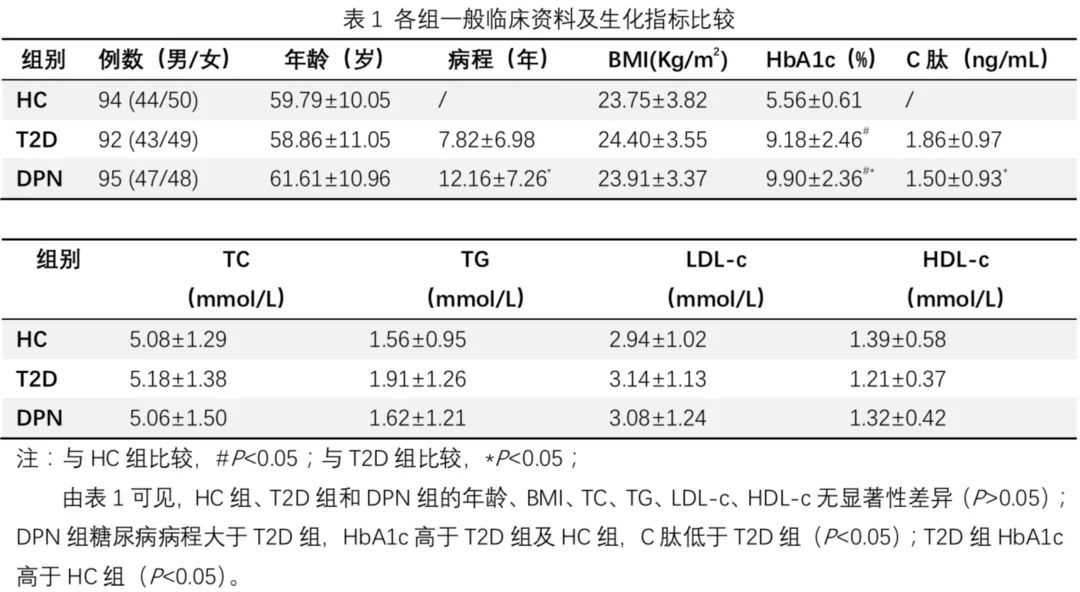
2.1 Comparison of General Clinical Data and Biochemical Indicators Among Groups is shown in Table 1.
2.2 Comparison of MCP-1 Genotype and Allele Frequency Among Groups is shown in Table 2.
2.3 Serum MCP-1 Levels are shown in Table 3
Discussion
DPN is one of the most common chronic complications in type 2 diabetes patients, with an incidence of 8% in newly diagnosed type 2 diabetes and more than 50% in long-term diabetes patients, and is also a significant risk factor for the occurrence and development of diabetic foot, causing a severe social burden [2]. The pathogenesis of DPN is still unclear, but it is currently believed that inflammatory responses, oxidative stress, and abnormal polyol pathways are all related to the onset of DPN [10].
MCP-1 is an inflammatory chemokine involved in various responses occurring in monocytes and macrophages, including the induction of superoxide anion, cytokine production, and expression of adhesion molecules [11].
In recent years, studies have found that MCP-1 and its gene polymorphisms are closely related to type 2 diabetes and its chronic complications, but there are fewer studies on its correlation with DPN. Some studies indicate that MCP-1 plays an important role in promoting chronic neuropathic pain through its receptor (CC chemokine receptor 2, CCR2) [12,13].
Moreover, CCR2 knockout mice do not develop neuropathic pain in nerve injury models, suggesting that the MCP-1/CCR2 signaling pathway is a necessary pathway for the occurrence of neuropathic pain [14].
This study focused on Han Chinese individuals from the coastal area of Zhejiang province, comparing the differences in MCP-1 levels and the distribution of the -2518A/G gene polymorphism among patients with type 2 diabetes with and without peripheral neuropathy, as well as a healthy control group.
The results indicate that compared with the healthy control group, serum MCP-1 levels are elevated in type 2 diabetes patients, and MCP-1 is closely related to the occurrence of DPN. MCP-1 levels, diabetes duration, and HbA1c are risk factors for DPN, which is consistent with the findings of Ma Furong [15] et al.
Analysis of the -2518A/G gene polymorphism among the three groups revealed that the frequency of the AA genotype in the DPN and T2D groups was higher than that in the HC group, while there were no significant differences in genotype and allele frequencies between the DPN and T2D groups, suggesting that the -2518A/G gene polymorphism is associated with the susceptibility to type 2 diabetes but not with the occurrence of DPN. This result aligns with the findings of Ma Jiangbo [16] et al. regarding the correlation between MCP-1 gene polymorphism and type 2 diabetes in a local population in Zhejiang.
The mechanisms of MCP-1’s effect on DPN remain unclear, but this study proposes possible pathways:
(1) Hyperglycemia activates the polyol pathway, leading to the glycosylation of nerve myelin proteins, resulting in excessive reactive oxygen species that not only cause demyelination of nerves but also directly damage nerves, triggering inflammatory responses. Damaged nerve axons can upregulate MCP-1 expression, attracting macrophages and stimulating the secretion of other inflammatory factors, leading to neuropathic pain and further exacerbating nerve damage [10,17];
(2) MCP-1 sensitizes transient receptor potential vanilloid type 1 (TRPV1) and transient receptor potential ankyrin 1 (TRPA1) via CCR2 on the spinal dorsal horn and dorsal root ganglia, causing Na+ and Ca2+ influx, thereby promoting neuronal excitation and the release of related neurotransmitters or neuropeptides, leading to pain hypersensitivity;
(3) MCP-1 co-stores and secretes with other neuropeptides such as calcitonin gene-related peptide (CGRP) and substance P, which may have a synergistic effect on pain transmission [18].
Although the results of this study suggest that MCP-1 levels are associated with DPN, its gene polymorphism, while affecting MCP-1 levels in diabetic patients, is not related to the occurrence of DPN. This may be related to other polymorphic sites that regulate MCP-1 transcription, as well as ethnic differences and regional factors, which require further study.
In conclusion, the results of this study confirm that compared to patients without peripheral neuropathy and healthy controls, serum MCP-1 levels are elevated in type 2 diabetes patients with peripheral neuropathy, suggesting that MCP-1 levels may aid in the diagnosis of DPN; however, the MCP-1 (-2518A/G) gene polymorphism is only related to T2DM and not to DPN occurrence.
Since the occurrence and development of diabetes and peripheral neuropathy are determined by a combination of various genetic and environmental factors, further research on other MCP-1 gene polymorphic sites and their interactions with environmental factors will help reveal the pathophysiological mechanisms of diabetic peripheral neuropathy.

Cheng Yi
Attending Physician
Endocrinology Department, First People’s Hospital of Wenling City
Graduated from Zhejiang University Clinical Medicine
Trained for six months at Ruijin Hospital in Shanghai
References
[1] Volmer-Thole M, Lobmann R. Neuropathy and Diabetic Foot Syndrome[J]. Int J Mol Sci. 2016,17(6).
[2] Edwards JL, Vincent AM, Cheng HT, et al. Diabetic neuropathy: mechanisms to management[J]. Pharmacol Ther. 2008,120(1):1-34.
[3] Vincent AM, Russell JW, Low P, et al. Oxidative stress in the pathogenesis of diabetic neuropathy[J]. Endocr Rev. 2004,25(4):612-628.
[4] Yagihashi S, Mizukami H, Sugimoto K. Mechanism of diabetic neuropathy: Where are we now and where to go? [J]. J Diabetes Investig. 2011,2(1):18-32.
[5] Melgarejo E, Medina MA, Sanchez-Jimenez F, et al. Monocyte chemoattractant protein-1: a key mediator in inflammatory processes[J]. Int J Biochem Cell Biol. 2009,41(5):998-1001.
[6] Jing Y, Zhu D, Bi Y, et al. Monocyte chemoattractant protein 1-2518 A/G polymorphism and susceptibility to type 2 diabetes in a Chinese population[J]. Clin Chim Acta. 2011,412(5-6):466-469.
[7] Madeshiya AK, Singh S, Dwivedi S, et al. Monocyte chemoattractant protein-1 gene polymorphism and its serum level have an impact on anthropometric and biochemical risk factors of metabolic syndrome in Indian population[J]. Int J Immunogenet. 2015,42(2):78-86.
[8] Moon JY, Jeong L, Lee S, et al. Association of polymorphisms in monocyte chemoattractant protein-1 promoter with diabetic kidney failure in Korean patients with type 2 diabetes mellitus[J]. J Korean Med Sci. 2007,22(5):810-814.
[9] Chinese Medical Association Diabetes Branch. Guidelines for the Prevention and Treatment of Type 2 Diabetes in China (2013 Edition)[S]. Chinese Journal of Endocrinology and Metabolism 2014,30:893-942.
[10] Pasnoor M, Dimachkie MM, Kluding P, et al. Diabetic neuropathy part 1: overview and symmetric phenotypes[J]. Neurol Clin. 2013,31(2):425-445.
[11] Kolattukudy PE, Niu J. Inflammation, endoplasmic reticulum stress, autophagy, and the monocyte chemoattractant protein-1/CCR2 pathway[J]. Circ Res. 2012,110(1):174-189.
[12] White FA, Sun J, Waters SM, et al. Excitatory monocyte chemoattractant protein-1 signaling is up-regulated in sensory neurons after chronic compression of the dorsal root ganglion[J]. Proc Natl Acad Sci U S A. 2005,102(39):14092-14097.
[13] Bhangoo SK, Ren D, Miller RJ, et al. CXCR4 chemokine receptor signaling mediates pain hypersensitivity in association with antiretroviral toxic neuropathy[J]. Brain Behav Immun. 2007,21(5):581-591.
[14] Abbadie C, Lindia JA, Cumiskey AM, et al. Impaired neuropathic pain responses in mice lacking the chemokine receptor CCR2[J]. Proc Natl Acad Sci U S A. 2003,100(13):7947-7952.
[15] Ma Furong, Ji Shangrong, Chen Hui et al. Serum MCP-1 levels and their gene polymorphism related to diabetic peripheral neuropathy[J]. Journal of Lanzhou University 2017,43(5):13-17.
[16] Ma Jiangbo, Xu Xin, Ma Gai et al. Study on the correlation between monocyte chemoattractant protein-1 gene polymorphism and type 2 diabetes in Han Chinese population in Zhejiang Province[J]. Zhejiang Medical Journal 2016,38(20):1646-1649.
[17] Tan X, Gao J, Shi Z, et al. MG132 Induces Expression of Monocyte Chemotactic Protein-Induced Protein 1 in Vascular Smooth Muscle Cells[J]. J Cell Physiol. 2017,232(1):122-128.
[18] Gao YJ, Zhang L, Samad OA, et al. JNK-induced MCP-1 production in spinal cord astrocytes contributes to central sensitization and neuropathic pain[J]. J Neurosci. 2009,29(13):4096-4108.
