 Introduction
Introduction
Immune inhibitory receptors (IRs) play a significant role in regulating the innate and adaptive immunity during chronic viral infections and cancer. Under chronic antigen stimulation, T cell dysfunction or exhaustion occurs, leading to the upregulation of many IRs, including programmed cell death receptor 1 (PD-1) and T cell immunoreceptor with immunoglobulin and ITIM domains (TIGIT). Simultaneously, tumor cells and antigen-presenting cells (APCs) express IR ligands within the tumor microenvironment (TME), allowing tumor cells to evade immune surveillance. Targeting IRs with monoclonal antibodies (MAB) has shown anti-tumor effects in mouse tumor models and humans, with anti-cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), anti-PD-1, or both becoming standard treatments for many solid tumors. There is substantial evidence supporting the critical role of TIGIT in limiting tumor adaptive immunity and innate immunity. Below, we will review the role of TIGIT in tumor immunology and the clinical outcomes of TIGIT-based tumor immunotherapy.
The TIGIT Functional Axis and Ligands
TIGIT (also known as WUCAM, Vstm3, VSIG9) is a receptor of the Ig superfamily that plays a critical role in limiting adaptive and innate immunity. TIGIT is involved in a complex regulatory network that includes multiple IRs (e.g., CD96/TACTILE, CD112R/PVRIG), a competitive co-stimulatory receptor (DNAM-1/CD226), and several ligands (e.g., CD155 (PVR/NECL-5), CD112 (Nectin-2/PVRL2)). Thus, there are some similarities with the CD28/CTLA-4/CD80/CD86 pathway, where inhibitory and co-stimulatory receptors compete for binding to the same ligands. In contrast to CTLA-4-/- mice, TIGIT-/- mice do not develop autoimmunity. However, compared to wild-type mice, TIGIT-/- mice exhibit more severe experimental autoimmune encephalomyelitis when immunized with myelin oligodendrocyte glycoprotein. Such observations support the functional role of TIGIT as a negative regulator of T cells.
TIGIT is expressed by activated CD8+ T and CD4+ T cells, natural killer (NK) cells, regulatory T cells (Tregs), and follicular helper T cells. In contrast to DNAM-1/CD226, TIGIT is weakly expressed in naïve T cells. In cancer, TIGIT co-expresses with PD-1 on mouse and human tumor antigen-specific CD8+ T cells and CD8+ tumor-infiltrating lymphocytes (TIL). It also co-expresses with other IRs, such as TIM-3 and LAG-3 on exhausted CD8+ T cells in tumors. Moreover, TIGIT is highly expressed in peripheral blood mononuclear cells of healthy individuals and cancer patients and is further upregulated in the TME.
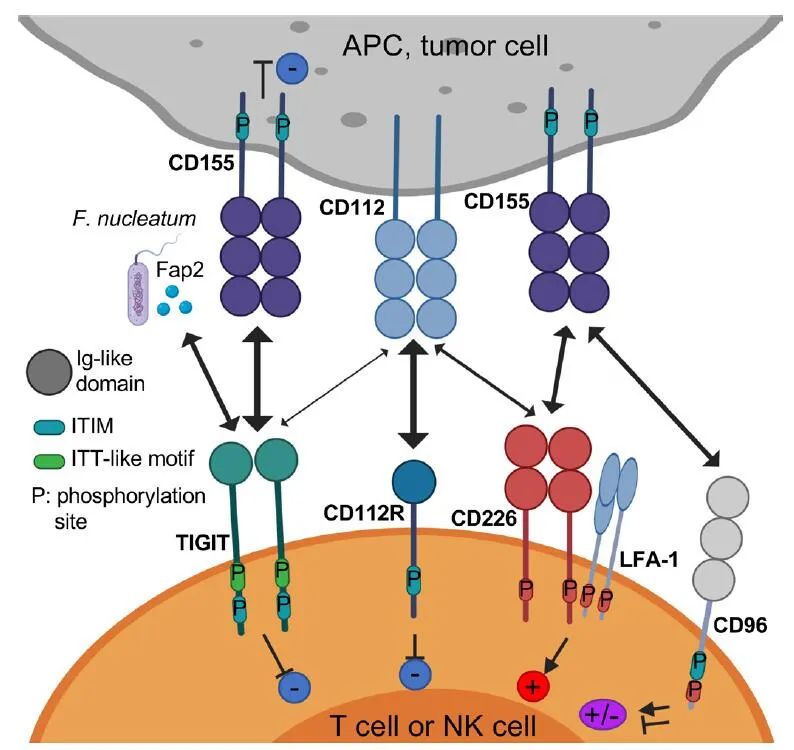
The increased expression of TIGIT is associated with low methylation of the TIGIT locus in Tregs and binding of FOXP3, distinguishing Tregs from activated effector CD4+ T cells. Compared to mouse splenic NK cells, NK cells in human circulation exhibit high TIGIT expression, regulating their tumor-killing activity. In contrast to CD8+ T cells, NK cells that are infrequently found in metastatic tumors are dysfunctional and downregulate the expression of TIGIT and CD226. Membrane-bound CD155 triggers the internalization and degradation of CD226, leading to reduced NK cell-mediated tumor reactivity. TIGIT binds to two ligands, CD155 and CD112, expressed on monocytes, dendritic cells (DC), and many non-hematopoietic cells (including tumor cells of different histological types). TIGIT has a higher affinity for CD155 than the competitive receptor CD226 and CD96.

TIGIT weakly binds to CD112, while CD112R has a higher affinity for CD112 than CD226. Interestingly, the expression of CD155 increases during reactive oxygen species-dependent DNA damage response activation, which modulates the interaction between NK cells and T cells and myeloid-derived suppressor cells (MDSCs). Moreover, the Fap2 protein from Fusobacterium nucleatum, an anaerobic Gram-negative commensal associated with colorectal cancer, can directly bind to TIGIT but not to CD226, thereby inhibiting NK cell and T cell-mediated tumor responses. These findings suggest that the gut microbiome modulates innate immune responses in a TIGIT-mediated manner.
TIGIT Structure and Signaling Pathways
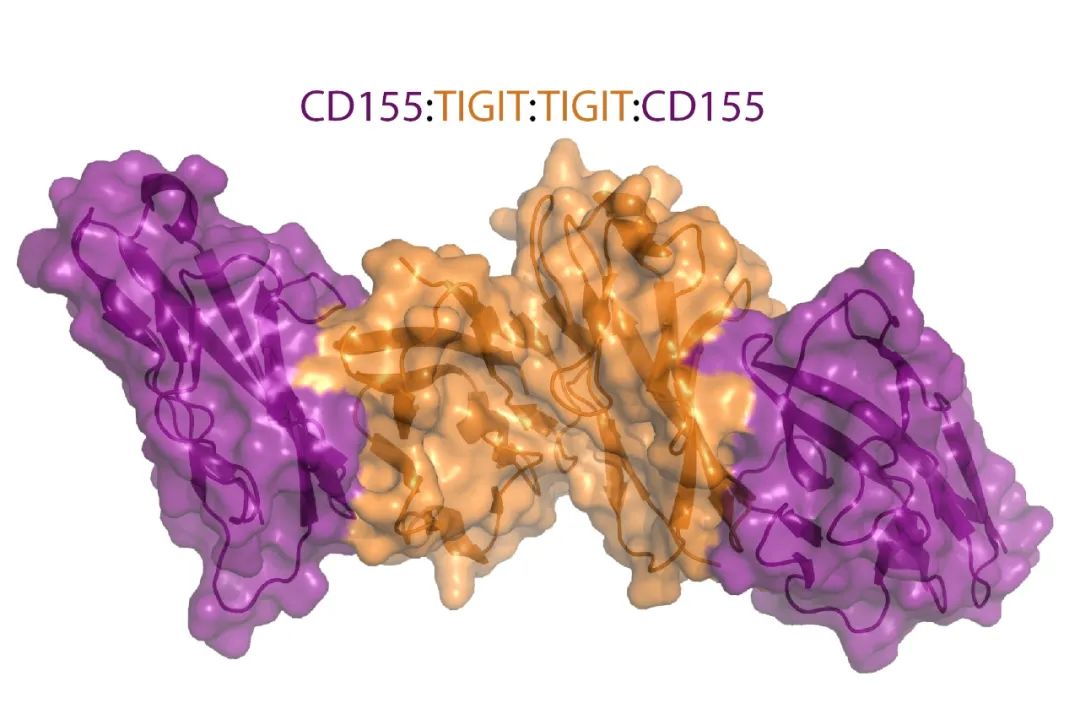
TIGIT consists of an extracellular immunoglobulin (Ig) variable domain, a type I transmembrane domain, and an intracellular domain that contains two conserved inhibitory motifs in mice and humans: an immune receptor tyrosine-based inhibitory motif (ITIM) and an Ig tail tyrosine-like (ITT) motif. The crystal structure of TIGIT bound to CD155 shows that two TIGIT/CD155 dimers form a heterotetramer with a TIGIT/TIGIT cis-homodimer at the core, where each TIGIT molecule binds to one CD155 molecule. This cis-trans receptor aggregation mediates cell adhesion and signaling.
In mice, phosphorylation of the ITIM (Y227) or ITT-like motif residue (Y233) can trigger TIGIT inhibitory signaling. However, in the human NK cell line YTS, TIGIT/CD155 binding initiates the main inhibitory signal through an ITT-like motif, while the ITIM motif mediates a smaller inhibitory signal. Following TIGIT/CD155 binding activation, the ITT-like motif is phosphorylated at Tyr225 and associates with intracellular signaling molecules Grb2 and β-arrestin 2 to recruit SH2-containing inositol phosphatase-1 (SHIP-1). SHIP-1 blocks phosphoinositide 3-kinase and mitogen-activated protein kinase signaling. SHIP-1 also inhibits the activation of TRAF6 and NF-κB, resulting in decreased NK cell production of IFN-γ.
TIGIT’s Inhibitory Mechanisms
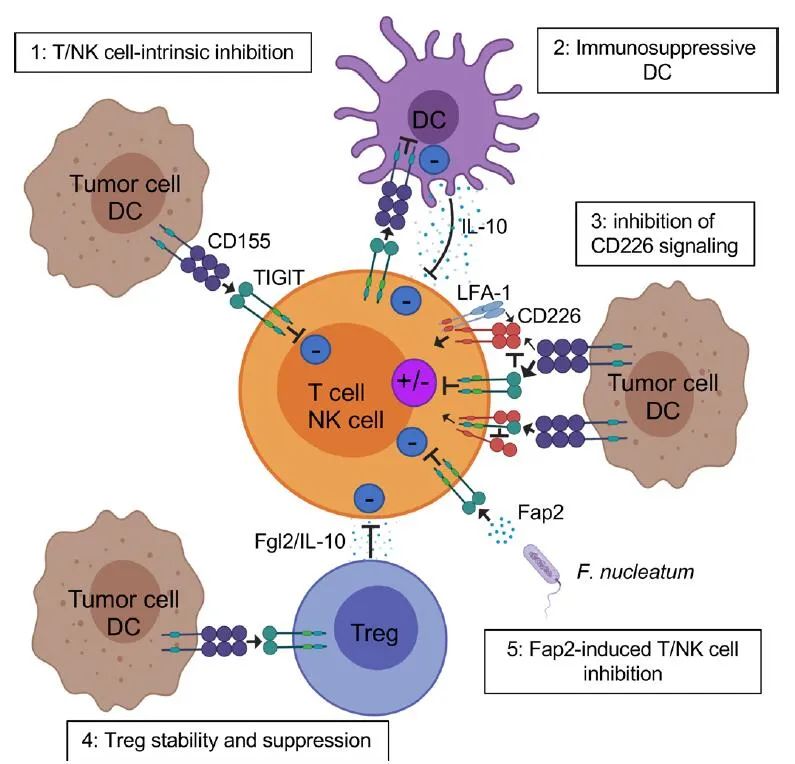
TIGIT potentially inhibits both innate and adaptive immunity through various mechanisms. First, in mouse models, TIGIT indirectly obstructs T cell function by binding to CD155 on DCs. The binding of TIGIT to DCs induces phosphorylation of CD155 and triggers a signaling cascade that promotes the formation of tolerogenic DCs, decreasing the production of interleukin (IL)-12 and increasing IL-10.
Second, TIGIT exhibits intrinsic inhibitory effects on immune cells directly. Anti-TIGIT agonistic antibodies suppress T cell proliferation and function by diminishing T cell receptor (TCR) driven activation signals. In both mice and humans, TIGIT inhibits NK cell degranulation, cytokine production, and NK cell-mediated cytotoxicity against CD155+ tumor cells. TIGIT+ NK cells interacting with CD155-expressing MDSCs reduce the phosphorylation of ZAP70/Syk and ERK1/2, lowering the cytolytic capacity of NK cells.
Third, multiple lines of evidence suggest that TIGIT obstructs CD155-mediated CD226 activation. CD226 is a co-stimulatory receptor widely expressed on immune cells, including T cells, NK cells, monocytes, and platelets. CD226 binds to LFA-1 to promote cell contact and trigger TCR signaling. This receptor also facilitates the production of pro-inflammatory cytokines by CD4+ T cells through binding to CD155. CD226 is directly involved in the recognition of tumors by T cells and NK cells in both mice and humans, with CD8+ T cells and NK cells in CD226-deficient mice showing defects in immune synapses, leading to a loss of anti-tumor immunity. TIGIT binds CD155 with higher affinity than CD226, thereby limiting CD226-mediated activation. Additionally, TIGIT can also directly cis-bind CD226, disrupting its ability to form homodimers with CD155.
Fourth, the balance of TIGIT/CD226 expression regulates the effector functions of T cells and NK cells. In TCR-activated CD4+ T cells, knocking down the expression of TIGIT with shRNA increases T-bet expression and IFN-γ production; conversely, CD226 knockout reduces T-bet expression and IFN-γ production. Moreover, blocking CD226 abolishes the effects of dual PD-1 and TIGIT blockade on tumor antigen-specific CD8+ T cell proliferation and cytokine production in melanoma. Similarly, in CT26 tumor-bearing mice, the anti-tumor effects of dual PD-L1/TIGIT blockers occur in a CD226-dependent manner and are eliminated after CD226 blockade. Interestingly, anti-PD-1 blockers and anti-GITR monoclonal antibody agonists can improve overall survival in MC38 tumor-bearing mice. In this model, inhibiting PD-1 rescues dysfunctional CD8+ T cells by blocking SHP2-mediated CD226 dephosphorylation, while anti-GITR monoclonal antibodies reduce TIGIT expression. These important findings support the notion that other immune checkpoint blockers (ICBs) can enhance T cell-mediated tumor rejection by balancing CD226 and TIGIT in CD8+ T cells beyond blocking PD-1 and TIGIT.
Fifth, TIGIT acts on Tregs, enhancing their immunosuppressive function and stability. TIGIT is highly expressed in a subset of natural Tregs in mice and in most human Tregs, with upregulation of TIGIT in Tregs associated with low methylation of the TIGIT locus and binding of Foxp3. Compared to TIGIT−Tregs, TIGIT+Tregs upregulate many Treg gene markers, including Foxp3, Helios, neuronilin-1, CTLA-4, PD-1, and LAG-3, at peripheral and tumor sites. TIGIT+Tregs also suppress pro-inflammatory responses from Th1 and Th17 but do not inhibit Th2. Following TIGIT activation, TIGIT++Tregs produce IL-10 and fibrinogen-like protein 2, mediating T cell suppression.
Interestingly, human Foxp3+Tregs exhibit lower CD226 expression compared to Foxp3−CD4+ T cells. In metastatic melanoma, CD226 is also downregulated in Tregs compared to peripheral Tregs, leading to an increased TIGIT/CD226 ratio. The TIGIT and CD226 interplay appears to enhance or diminish Treg suppression and stability, respectively. The TIGIT/CD226 ratio in Tregs seems to correlate with increased Treg frequency in tumors and unfavorable clinical outcomes in ICB therapy. Further studies are needed to determine whether the TIGIT/CD226 ratio in Tregs can serve as a biomarker for clinical response to ICB in patients with solid tumors.
Clinical Prospects of TIGIT Blockers
Dual PD-1 and TIGIT blockers represent a promising strategy for tumor combination immunotherapy. Although each individual blocker does not significantly impede the growth of CT26 tumors in mice, the synergistic effect of TIGIT and PD-1/PD-L1 dual blockers enhances the proliferation and function of anti-tumor CD8+ T cells, resulting in the generation of protective memory T cells and complete tumor rejection, extending overall survival.
Compared to single blockers, dual PD-1/TIGIT blockers also enhance the proliferation and function of tumor antigen-specific CD8+ T cells and TILs isolated from melanoma patients. Interestingly, the PD-L1/TIGIT dual blocker (atezolizumab/tiragolumab) appears to provide higher clinical benefits as first-line therapy for PD-L1 positive non-small cell lung cancer patients compared to PD-L1 blockers alone, despite similar toxicity. However, these observations need to be confirmed in large randomized clinical trials.
The effects of PD-1/TIGIT dual blockers in vitro and in mouse tumor models can be antagonized by blocking CD226, indicating that TIGIT blockade primarily exerts its effects by directing CD155-mediated signaling towards CD226 activation. Following this logic, the downregulation of CD226 expression in CD8+ TILs across multiple solid tumors (including melanoma) may represent a significant barrier limiting the impact of dual PD-1/TIGIT blockers on cancer patients. Membrane-bound CD155 mediates the downregulation of CD226 in immune cells within the TME, supporting the role of CD155 in mediating immune dysfunction.
In animal models, TIGIT blockade or TIGIT deficiency significantly enhances NK cell-mediated anti-tumor responses both in vitro and in vivo. A recent study on B16 melanoma and CT26 lung metastatic mouse models indicated that TIGIT blockers, alone or in combination with PD-1 blockers, primarily act on NK cells to enhance CD8+ T cell-mediated anti-tumor responses to inhibit tumor growth. In these experimental models, NK cell-specific TIGIT deficiency and NK cell exhaustion diminish the effectiveness of TIGIT blockade. However, many other studies support that single TIGIT blockade does not significantly enhance CD8+ T cell immunity and promotes tumor rejection in wild-type mice bearing solid tumors. These conflicting observations indicate that the mechanisms of potential helper roles of NK cells on CD8+ TILs and the relevance of these findings to cancer patients remain unclear. Whether and how NK cells participate in guiding CD8+ T cell initiation, maturation, and memory differentiation in response to environmental cues requires further investigation. Interestingly, IL-15 and TIGIT blockade can increase NK cell-mediated melanoma cell toxicity in vitro and reduce metastasis in mouse melanoma models. This finding supports the development of new combination immunotherapies using IL-15 and TIGIT blockers to promote the killing of MHC class I deficient melanoma, which is unresponsive to CD8+ T cell-mediated immune responses.
In addition to PD-1 blockers, other ICBs combined with TIGIT blockers can also enhance anti-tumor immune responses. For example, TIGIT and TIM-3 synergistically inhibit anti-tumor immune responses in mice. In another trial, mixed T cell subsets including CD8+ T cells, CD4+ T cells, and Tregs were subcutaneously transferred into wild-type, TIGIT-/- mice and Rag-/- mice carrying B16F10, indicating that TIGIT primarily acts in Tregs to hinder CD8+ T cell anti-tumor responses, promoting tumor growth. TIGIT+ Tregs infiltrating tumors upregulate TIM-3, and blocking TIM-3 in TIGIT-/- mice can further slow tumor growth and improve overall survival.
As TIGIT competes with IRs CD96 and CD112R for binding to its ligands, several studies have investigated combination therapies of TIGIT and other IRs in the TIGIT family with PD-1, including CD96 and CD112R. TIGIT and CD96 have a synergistic effect in inhibiting anti-tumor responses in tumor-bearing mouse models with lung metastasis, with the anti-tumor effects of CD96 blockers being higher in TIGIT-/- mice. CD96 blockers are more effective when used in combination with anti-CTLA-4 or anti-PD-1, and their effects depend on NKs, CD226 signaling, and IFN-γ production. Additionally, TIGIT blockers, either alone or in combination with PD-1 blockers plus CD96 blockers, significantly reduce the growth of B16 melanoma in wild-type and Cd155-/- mouse models. Notably, the role of CD96 as an IR remains controversial, as there is also evidence suggesting it can serve as a co-stimulatory receptor for CD8+ T cells. Multiple experimental studies in vitro and in mouse models indicate that CD112R blockade combined with TIGIT blockade can enhance anti-tumor immune responses. CD112R blockers synergistically enhance antibody-dependent cell-mediated cytotoxicity (ADCC) triggered by NK cells against breast cancer cells in vitro. In the MC38 tumor mouse model, dual CD112R/PD-L1 blockade shows significant improvement compared to single blockade. Furthermore, CD112R blockers, either alone or in combination with TIGIT blockers and/or PD-1 blockers, can increase the capacity of TILs from ovarian, endometrial, and lung tumors to produce cytokines.
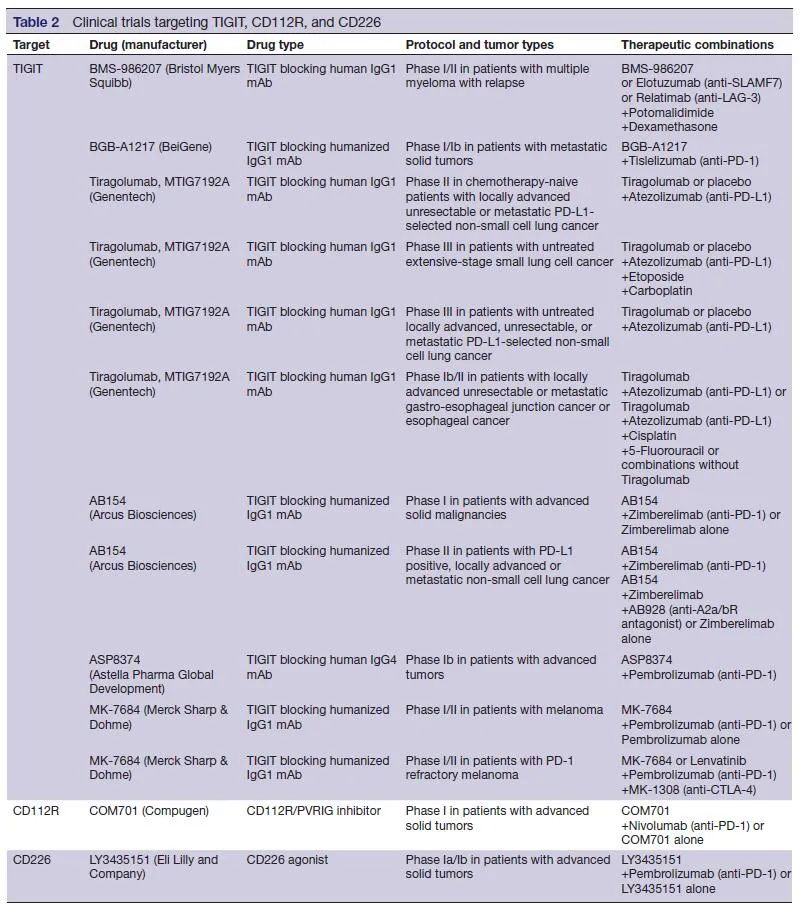
Several studies suggest that anti-CTLA-4 monoclonal antibodies exert their effects through ADCC-mediated Treg depletion. Given that Tregs highly express TIGIT in the TME, there are concerns about whether anti-TIGIT monoclonal antibodies with Fc receptor binding capabilities would lead to Treg depletion. Interestingly, in mouse tumor models, anti-TIGIT monoclonal antibodies with Fc mutations showed enhanced antigen-specific T cell responses and tumor reactivity through selective binding to FcγR on APCs, without evidence of Treg depletion. Whether the anti-TIGIT antibody’s anti-tumor effects in cancer patients are Fc-dependent remains to be further studied. The answer to this critical question may come from several phase I and II clinical trials testing engineered Fc anti-TIGIT monoclonal antibodies: IgG1 (MTIG7192/Genentech, MK-7684/Merck, and OP-313M32/Oncomed), inert Fc-IgG1 (BMS-986207/Bristol-Myers-Squibb; AB-154/Arcus), and IgG4 (ASP8374/Potenza/Astellas).
Challenges and Prospects
TIGIT is a promising target for tumor immunotherapy, particularly in combination with PD-1 blockers. However, as clinical trials based on TIGIT progress in cancer patients, we need to address several key issues and challenges. First, what are the mechanisms of action of TIGIT blockers in cancer patients? Are these effects primarily mediated by their direct activity in CD8+ T cells, Tregs, or both? Can TIGIT block the reprogramming of APCs in the TME to enhance T cell initiation or activation? Do these effects vary depending on the disease stage? Can TIGIT blockers mediate NK cell responses to MHC class I deficient tumors in vivo, offering clinical benefits for PD-1 refractory cancer patients? Furthermore, beyond PD-1/TIGIT dual blockade, do CD112R or CD96 blockers have any potential synergistic effects, as shown in mouse tumor models and in vitro studies? In this regard, we must remember that the role of CD96 as an IR remains controversial. Moreover, the potential evidence of CD112R blockade enhancing the specificity of human tumor antigen-specific CD8+ T cells is still lacking. The answers to these important questions may come from phase I clinical trials evaluating the efficacy of a CD112R inhibitor alone or in combination with anti-PD-1 monoclonal antibodies in patients with advanced solid tumors (NCT03667716).
Additionally, CD226 plays a crucial regulatory role in PD-1/TIGIT dual blockade. The downregulation of CD8+ T cells and NK cells in the TME may be a major barrier to the success of PD-1/TIGIT dual blockade. Therefore, it is necessary to design new strategies to increase CD226 expression and signaling to prevent its downregulation in the TME. Notably, an ongoing clinical trial is testing anti-CD226 agonists in multiple cancers (NCT04099277).
However, due to the role of CD226 in mediating platelet adhesion and activation, potential hematologic adverse events need to be carefully monitored. Finally, clinical trials using various engineered Fc anti-TIGIT monoclonal antibodies may help determine the role of FcγR synergy in TIGIT blockade.
In summary, within just ten years of its discovery, TIGIT has entered clinical trials as a target for immunotherapy. As research into TIGIT-mediated immune response regulation deepens, it will aid in the design of optimized combination strategies for TIGIT blockers in cancer patients and will also help develop therapies targeting TIGIT for other chronic diseases expressing this protein.
References:
TIGIT in cancer immunotherapy. J Immunother Cancer 2020;8:e000957.
Benefits:The JPM 2021 Three-Day Collection40 PPT Electronic Versions The editor has collected 40 PPTs from various companies at the JP Morgan conference to capture the hot news and future trends from the conference.

Scan the code to register for information, and you can receive the download link!
Scan to Receive
Recognize the WeChat QR code, add the antibody circle editor, and qualified individuals can join the antibody circle WeChat group!Please specify: Name + Research Direction!

All articles reproduced by this public account are for the purpose of conveying more information, and the source and author are clearly indicated. Media or individuals who do not wish to be reproduced can contact us ([email protected]), and we will delete it immediately. All articles represent the author’s opinions and do not represent the position of this site.