Forum Introduction: Common types of vascular malformations include cerebral cavernous malformations (CCM), capillary telangiectasia, developmental venous anomalies (DVA), and arteriovenous malformations (AVM). CCM is a common congenital vascular malformation of the brain and is the second most common vascular malformation in the central nervous system. Its incidence ranges from 0.16% to 0.5%, accounting for 5% to 10% of vascular malformations in the brain, commonly found in adults aged 40 to 50, with a higher prevalence in females than males. It often leads to 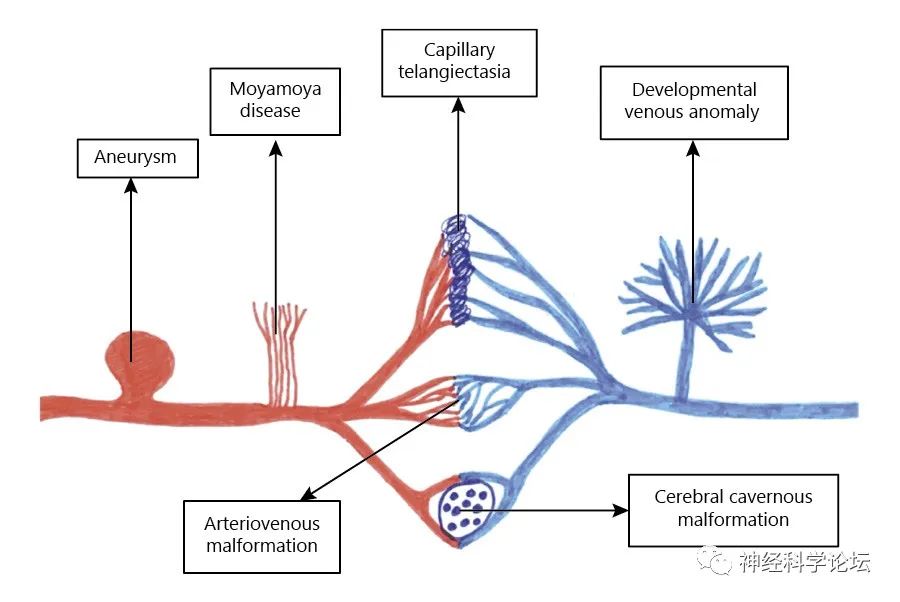
Etiology and Pathogenesis
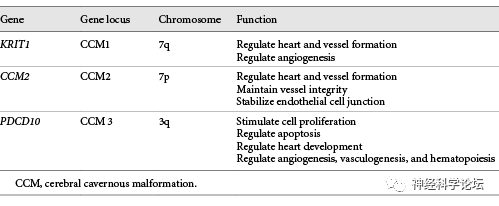
Hereditary or familial CCM—accounts for about 20% of all patients with cavernous malformations, often with a positive family history and usually presents as multiple lesions. It is caused by autosomal dominant mutations in three genes: CCM1, CCM2, and CCM3. In most cases, these mutations may be nonsense, frameshift, or splice site mutations that result in non-functional protein products. In some cases, there may be deletions or duplications of multiple exons or entire genes. Sporadic CCM – sporadic cavernous malformations are less common and present as single lesions. They are usually asymptomatic and may be associated with DVA.
CCM consists of small vascular clusters formed by the dilation of endothelial cells, with the vessel walls composed of structurally abnormal collagen forming a stroma, irregularly shaped. These small vessels lack muscle layers and elastic fibers, embedded in collagen stroma, devoid of neurons, and contain no brain tissue. Iron-laden hemosiderin often deposits on the walls of capillaries surrounding the lesion. CCM is a vascular space lined by a monolayer of endothelial cells, with no intervention into the brain parenchyma. The blood flow pressure within the lesions is low, with slow blood flow, leading to thrombosis, which occurs repetitively. These features are roughly visualized as a characteristic “mulberry appearance.” Insufficient tight and adherens junctions between endothelial cells lead to leakage and dysfunction of the blood-brain barrier.
Clinical Manifestations
CCM can present differently depending on the location of the lesions. They can be supratentorial, affecting the cerebral cortex, or infratentorial, affecting the brainstem or cerebellum. 70% to 80% of CCMs are located supratentorially, with epilepsy being the most common clinical manifestation of supratentorial CCM, occurring at a rate of 48.1% to 79%, higher than that of gliomas and arteriovenous malformations. When these lesions become symptomatic, they may present with various clinical manifestations, including seizures, hemorrhage, headaches, and focal neurological deficits. Supratentorial lesions are more commonly associated with seizures, while infratentorial lesions present as focal neurological deficits. Some studies have attempted to explain the natural process of hemorrhage in CCM patients. Gross et al. summarized the risk factors for hemorrhage in these patients, including previous hemorrhage from cerebral cavernous malformations, female sex, and the location of lesions in the brainstem. Cavernous malformations are a rare cause of isolated non-aneurysmal subarachnoid hemorrhage, with very few reported cases.
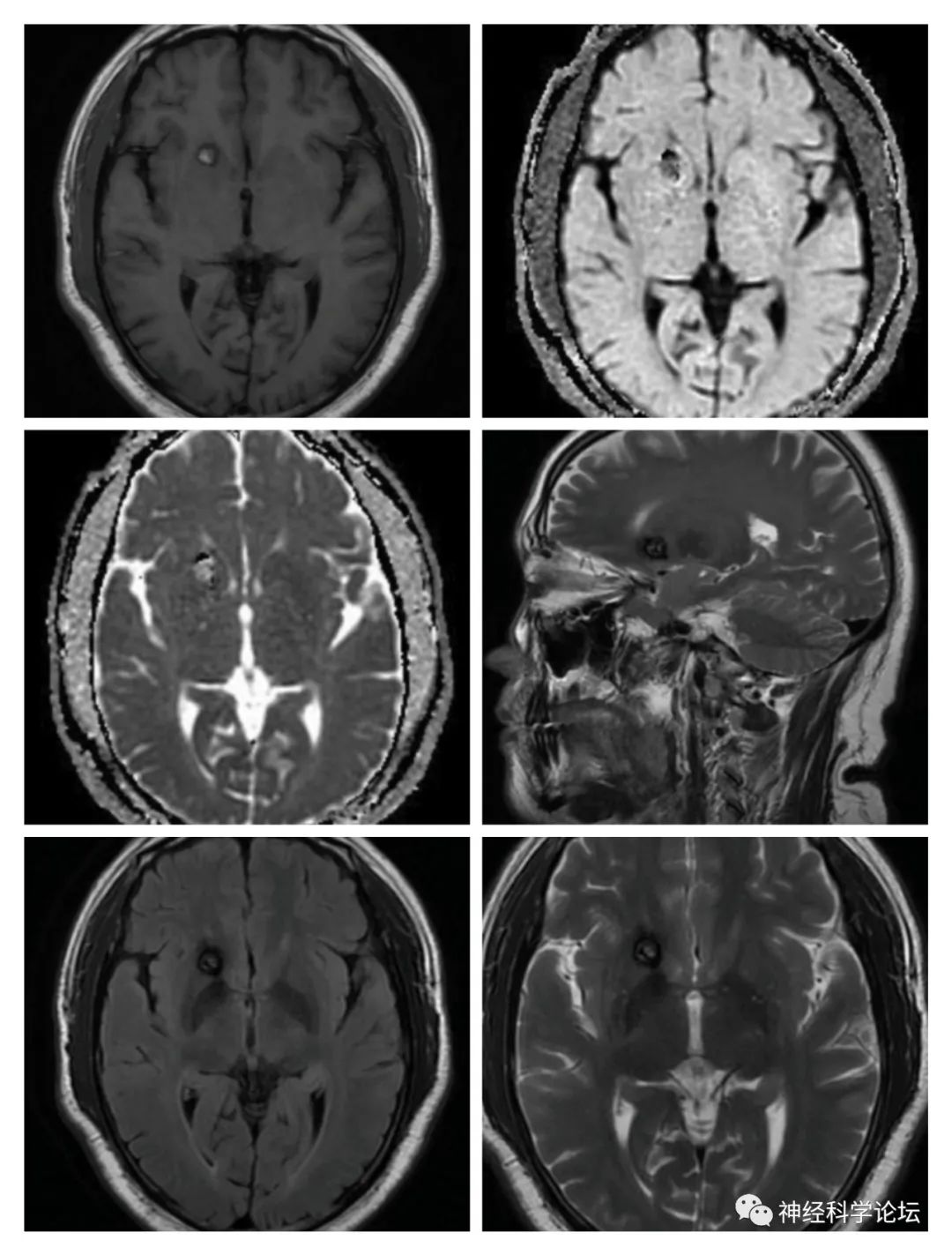
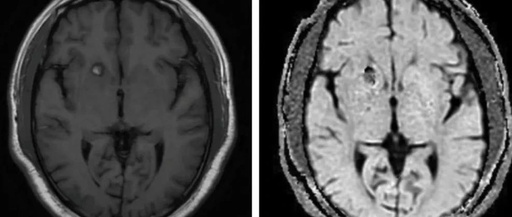
A 50-year-old male presented with sudden loss of smell. Cavernous malformations
A prospective imaging study conducted at the Mayo Clinic involving 4,721 individuals aged 50 to 89 found an overall prevalence of 0.46%, with a slightly higher prevalence in males compared to females. The overall prevalence of familial CCM is approximately 1 in 3,300 to 1 in 3,800, with the incidence of symptomatic genetic mutations around 1 in 5,400 to 1 in 6,200.
Imaging Diagnosis
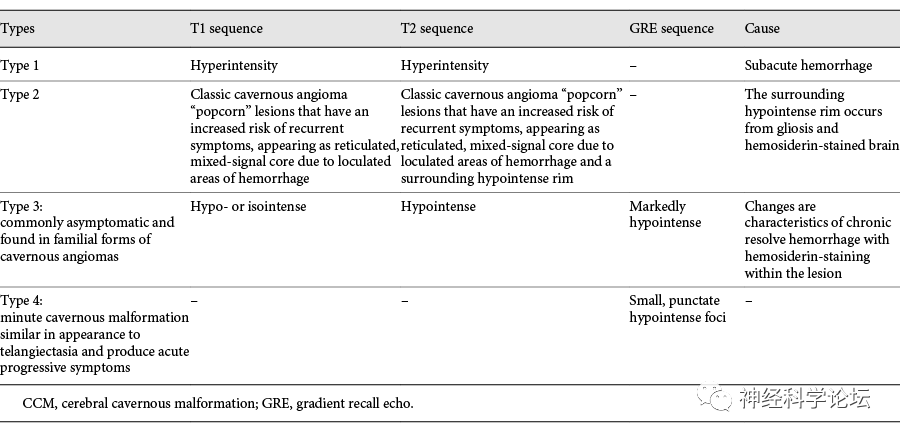
Diagnosing CCM can be challenging as they often appear hidden on angiography due to slow blood flow. Early detection and timely management are necessary as they increase the likelihood of recurrent hemorrhage. CT scans can reveal lesions with associated hemorrhage or calcification, but they lack sensitivity and specificity for detecting smaller lesions; thus, they are not the primary method for diagnosing these lesions. MRI shows higher specificity in detecting symptomatic and asymptomatic lesions, particularly those located in the posterior fossa or brainstem. The MRI characteristics of cavernous malformations can also be seen in other conditions, such as hemorrhagic tumors or metastases, tumor calcifications, occult vascular malformations, oligodendrogliomas, and pleomorphic xanthoastrocytomas. Based on MRI images, cavernous malformations can be classified into four types.
Treatment and Prognosis
Currently, if the lesions are incidentally diagnosed and asymptomatic, conservative treatment is recommended, regardless of their location, with annual MRI to assess growth. If the lesions present with severe clinical symptoms, microsurgical resection or stereotactic radiosurgery is recommended. The main treatment options for intracranial CCM currently include microsurgical resection, stereotactic
A 2016 study published in The Lancet Neurology included 1,620 patients with a follow-up duration of approximately 5,200 patient-years, utilizing a meta-analysis of patient data to assess the natural course of cavernous malformations and intracranial hemorrhage (ICH). Kaplan-Meier survival analysis was conducted to observe outcomes for patients at five years post-follow-up. The study found that patients with a single hemispheric cavernous malformation but without prior ICH or focal neurological deficits had an ICH incidence of about 4% over five years of follow-up. For patients with brainstem cavernous malformations and without ICH or focal neurological deficits, this rate was as high as 8%. If patients had a hemispheric lesion and a history of ICH or focal neurological deficits, their ICH occurrence rate sharply increased to about 18%. Finally, patients with concurrent brainstem cavernous malformations and ICH and/or focal neurological deficits had the highest symptomatic ICH occurrence rate, approximately 31%. CCM has an incidence of <1%, with an annual bleeding risk of up to 3%, and a rebleeding risk of 4.5-23%, making it the second most common form of vascular malformation after DVA. Although it is found to be more common in the third decade of life, malformations can exist in any age group.
References
-
Idiculla PS, et al. Cerebral Cavernous Malformations, Developmental Venous Anomaly, and Its Coexistence: A Review. Eur Neurol. 2020;83(4):360-368.
-
Zafar A, et al. Familial Cerebral Cavernous Malformations. Stroke. 2019 May;50(5):1294-1301.
-
addock M,et al.Pediatric Cerebral Cavernous Malformations. Pediatr Neurol. 2021 Mar;116:74-83.
Neuroscience Forum
Latest Neuroscience Information Sharing Platform
Rare Disease Consultation Platform for Difficult Neurological Conditions


This public account aims to disseminate cutting-edge information in neuroscience and explore clinical challenges in rare neurological diseases for educational purposes! We welcome original works for submission. The content and images are shared to convey more scientific information. If you wish for any content to be removed, please contact us. Submission and contact email: [email protected].