
Cover photo: Teacher Deng Minxing
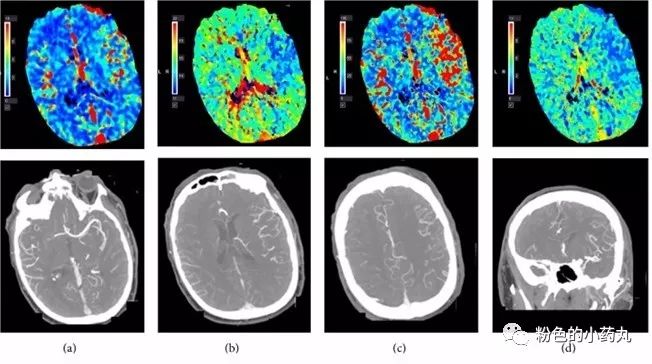
Figure 1. CTP perfusion imaging and dilation of the left middle cerebral artery and its branches after intravenous rtPA treatment: (a) increase in cerebral blood volume (CBV); (b) shortened time to peak (TTP); (c) increase in cerebral blood flow (CBF); (d) shortened mean transit time (MTT).
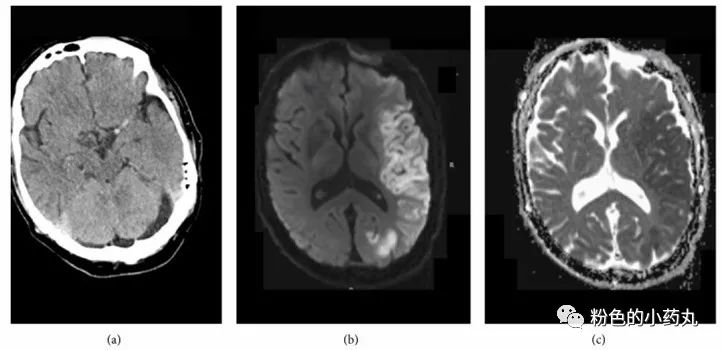
Figure 2. (a) Initial CT before intravenous rtPA indicated high-density signs in the middle cerebral artery; (b) the next day’s MRI diffusion-weighted imaging and (c) ADC both confirmed acute infarction in the LMCA region.
After rtPA treatment, CTA and CTP examinations showed recanalization and dilation of the affected intracranial arteries as well as increased perfusion in the infarcted area. Therefore, this case reminds us not to forget about cerebral hyperperfusion syndrome in patients with clinical deterioration after tPA treatment for acute ischemic stroke.
Cerebral hyperperfusion syndrome (CHS) is a clinical syndrome of reperfusion injury and is a rare complication after rapid revascularization procedures. The incidence of CHS after carotid endarterectomy and carotid artery stenting is 1-3%, and it can also occur in acute ischemic stroke (AIS) patients after intravenous tPA treatment. Although the incidence of intracranial hemorrhage caused by CHS is low, the mortality and disability rates are extremely high and should be taken seriously. The pathogenesis of CHS is currently believed to be related to several factors, including impaired cerebral blood flow autoregulation, activated endothelial cells, microvascular lesions caused by hypertension, the effects of nitric oxide and free radicals, and dysfunction of carotid sinus baroreceptors.
1. Risk factors: These include advanced age, hypertension, diabetes, recent history of stroke, severe carotid stenosis, bilateral stenosis, infection, and chronic inflammatory diseases.
2. Clinical manifestations: The clinical manifestations are mainly due to vascular re-canalization leading to excessive perfusion, resulting in vasogenic cerebral edema or intracranial hemorrhage, occurring in most patients within hours to days after the procedure. The most common symptoms are headache on the affected side and altered consciousness. There may be fluctuating pain in the ipsilateral frontal and temporal regions or diffuse headache, vomiting, vision loss, altered consciousness, hypertension, etc. After cerebral edema occurs, there may be corresponding symptoms of increased intracranial pressure and seizures.
3. Auxiliary examinations: TCD, CT, MRI, PET, and SPECT can all assist in the diagnosis of cerebral hyperperfusion syndrome, with different methods emphasizing different aspects.
1、CT can quickly clarify whether there is an intracranial hematoma and can distinguish it from acute ischemic stroke. In the hours following onset, acute ischemic stroke usually shows no abnormal changes on CT, while CHS can show swelling of the affected brain tissue, disappearance of sulci and gyri on CT after onset, which are indirect signs of CHS. SPECT can early reveal signs of cerebral hyperperfusion syndrome not detected by CT.
2、MRI diffusion-weighted imaging (DWI) can be used to exclude acute ischemic stroke, T2WI and FLAIR imaging can better show cerebral edema.
3、TCD has many advantages in the diagnosis and treatment of cerebral hyperperfusion syndrome. It is simple and non-invasive, allowing for direct and real-time monitoring of cerebral blood flow (CBF) and cerebral blood flow velocity, and can use preoperative blood flow status as a reference baseline for comparison with postoperative measurements to prevent the occurrence of cerebral hyperperfusion syndrome. Currently, it is believed that an increase in postoperative cerebral blood flow velocity exceeding100% indicates cerebral hyperperfusion syndrome.
4、CTP also assists in the diagnosis of CHS, with mean transit time (MTT) significantly correlated with the occurrence of CHS. An MTT greater than 3 seconds is a risk factor for the occurrence of CHS. The degree of MTT prolongation is positively correlated with the degree of intracranial vascular stenosis and reduction in cerebral blood flow. Reduced cerebral blood flow, prolonged mean transit time, and slight increase in cerebral blood volume (CBV) suggest intracranial vascular dilation and impaired cerebral blood flow autoregulation, increasing the risk of postoperative CHS. Arterial spin labeling (ASL) is similar to CTP but does not require additional contrast injection, making it suitable for patients with renal failure.
5、PET can also provide valuable information for the diagnosis of cerebral hyperperfusion syndrome. Matsubara and others compared PET imaging before and after carotid artery stenting and found that postoperative cerebral blood flow, cerebral perfusion pressure (CPP), and cerebral oxygen metabolism rapidly increased and peaked, while the cerebral blood flow reserve capacity only slightly increased, which may be one of the mechanisms for the occurrence of cerebral hyperperfusion syndrome.
4. Diagnostic criteria: The diagnosis of CHS is mainly based on the occurrence of headache, seizures, and focal neurological deficits unrelated to ischemia after vascular recanalization, especially seizures are more indicative of a CHS diagnosis and should be distinguished from AIS. If the above clinical symptoms occur and auxiliary examinations such as CTP and TCD confirm the existence of excessive perfusion in the brain tissue, it can be considered as cerebral hyperperfusion syndrome.
5. Prevention: 1. Improve auxiliary examinations. CTP and TCD help understand baseline levels of cerebral blood flow, mean flow velocity, etc., and comparisons before and after can assist in predicting the occurrence of CHS. For patients with indications for cerebral angiography, DSA can accurately determine the development of the circle of Willis and collateral compensation. The integrity of the circle of Willis is a protective factor against CHS. 2. Control blood pressure. Strict blood pressure control is currently the most focused preventive method for CCHS. Patients with normal blood pressure may still have a high risk of cerebral hyperperfusion syndrome. Blood pressure control should continue until cerebral vascular reactivity returns to normal; TCD helps to understand cerebral vascular reactivity. Sodium nitroprusside and calcium antagonists can increase cerebral blood flow and should be avoided in clinical use. Studies have shown that β–adrenergic receptor blocker labetalol can prevent CHS by lowering mean arterial pressure and cerebral perfusion pressure. 3. Oxygen free radical scavengers. The large generation of oxygen free radicals is one of the mechanisms for the occurrence of CHS, thus scavenging oxygen free radical drugs such as edaravone can prevent the occurrence of CHS, providing a new clinical treatment approach for its prevention. 4. Surgical measures and timing. (1) Stepwise release of the stent: Stepwise release of the stent to phase-wise resolve vascular stenosis is a simple and effective preventive measure. Research by Yoshimura in Japan showed that patients who underwent balloon pre-dilation of stenotic areas 1-2 months before stenting had a significantly lower incidence of CHS compared to those who directly underwent stenting. (2) Surgical timing: Studies show that patients with carotid stenosis undergoing carotid artery stenting within one week after stroke have a higher risk of developing CHS. Xu and others found that undergoing intracranial artery stenting within three weeks after stroke is a risk factor for CCHS.
6. Treatment: Currently, there are no guidelines for the treatment of cerebral hyperperfusion syndrome, and treatment should focus on managing cerebral edema. Mannitol or hypertonic saline can be used to reduce intracranial pressure, and corticosteroids and barbiturates may also be effective for some patients with cerebral edema. If seizures are present, antiepileptic drugs should be added, but preventive use of antiepileptic drugs is not recommended. In cases of concomitant intracranial hemorrhage, surgical intervention should be determined based on the size and location of the hematoma.
References: 1. Imaging Evidence for Cerebral Hyperperfusion Syndrome after Intravenous Tissue Plasminogen Activator for Acute Ischemic Stroke. Yi Zhang, et al. Case Rep Neurol Med. 2016;2016:8725494.
2. Progress in the Study of Cerebral Hyperperfusion Syndrome. Zhang Guang et al., Chinese Journal of Modern Neurology, December 2017, Vol. 17, No. 12, 869-873.
