ABSTRACT Abstract
A patient with a Class II division 2 malocclusion is presented, illustrating the application of a modified double J retractor (DJR) and palatal miniscrews along with clear aligners to correct the malocclusion and normalize the incisor torque. In terms of incisor torque recovery, a nonextraction approach might be a good choice if the Class II correction could be successfully achieved with total arch distalization. When maxillary molar distalization was limited by anatomical boundaries, the treatment plan was changed to bilateral maxillary first premolar extractions, which led to even more retroclination of the maxillary incisors after space closure. Anterior interdental miniscrews were used to intrude the maxillary incisors. A modified DJR and palatal miniscrews were used to regain torque and achieve palatal root movement of the maxillary incisors. The treatment effects and biomechanical designs were evaluated for torque recovery of the retroclined maxillary incisors.
INTRODUCTION Introduction
The incisors tend to retrocline during space closure in extraction treatment. This is especially difficult to manage in Class II division 2 patients, who often present with significantly retroclined maxillary incisors. In conventional edgewise mechanotherapy, rectangular archwires are required to control the torque with third-order bends through the interaction of the archwire and the bracket slots. Because incisor torque control is even more challenging with aligners, nonextraction treatment approaches such as maxillary molar distalization are often considered instead of extractions. Programmed overcorrection in anterior torque or adding power ridges are common strategies for incisor torque control in extraction aligner treatment. However, it is not always predictable. The double J retractor (DJR) is a lingual retractor that aims to retract incisors bodily via lever arm mechanics and helps incisor torque control during space closure. This case reports on the application of the modified DJR when used in conjunction with aligners for incisor torque recovery after space closure.
Diagnosis and Etiology Diagnosis and Etiology
A 41-year-old female patient visited the clinic with a chief complaint of protrusion and deep overbite. She wished to correct her bite before having final restoration of her maxillary anterior teeth. No contributory past medical history was reported. Past dental history included regular dental prophylaxis and restorations, including crowns. In consideration of her work and social activities, she preferred to use clear aligners for her orthodontic treatment.
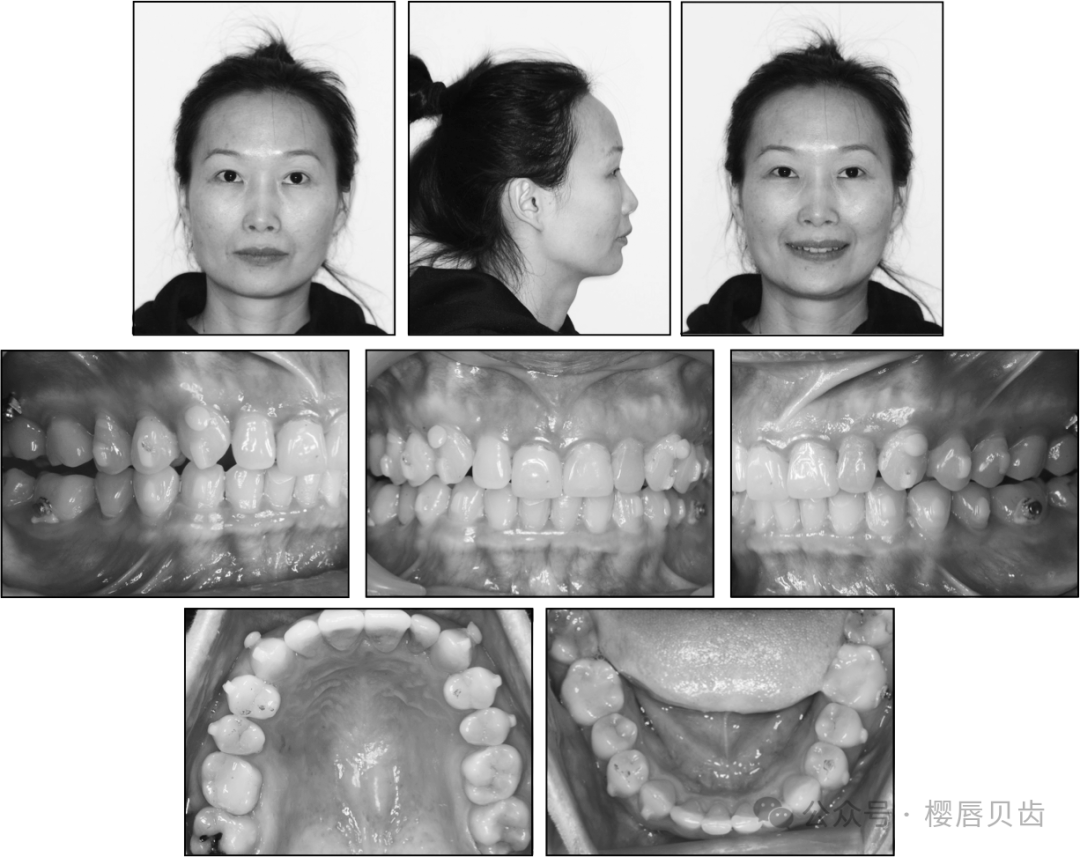
On clinical examination, she showed a mildly convex lateral profile with a slightly protrusive upper lip and a retruded mandible with strong chin projection (Figures 1 and 2). The nasolabial angle was within the normal range. The labiomental fold was slightly deep. The frontal facial view showed no obvious asymmetry. The vertical facial proportions were within the normal range. Intraoral photographs showed a 100% deep overbite, which measured 4.8 mm. The overjet was 3.7 mm. The maxillary dental midline was coincident with the facial midline, whereas the mandibular dental midline was shifted to the right by 2.5 mm. Bilateral molar and canine relationships were Class II. The curve of Spee was 2.2 mm in depth. The arch form was more square in the maxillary arch and more tapering ovoid in the mandibular arch, without obvious asymmetry. The space discrepancies were 4.5 mm in the maxillary arch and 4.0 mm in the mandibular arch. Two splinted porcelain-fused-to-metal crowns were noted on the upper central incisors.
Figure 1.

Pretreatment facial and intraoral photographs.
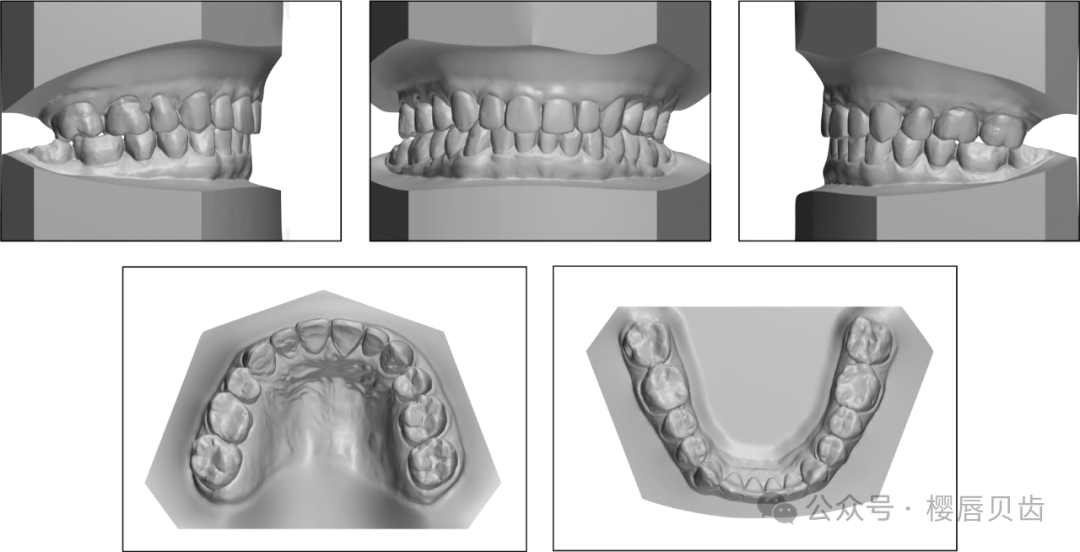
Figure 2.
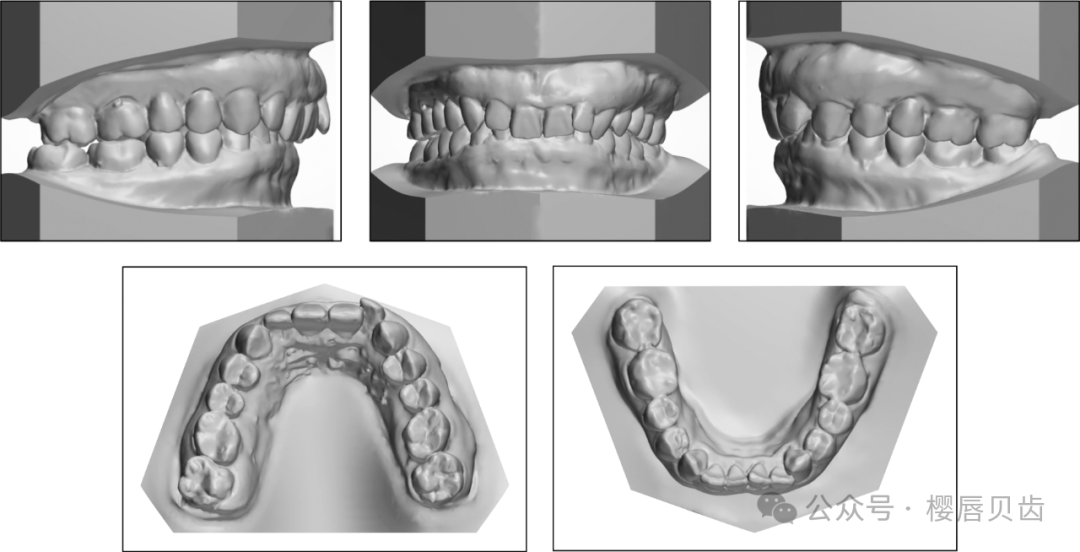
Pretreatment study models.
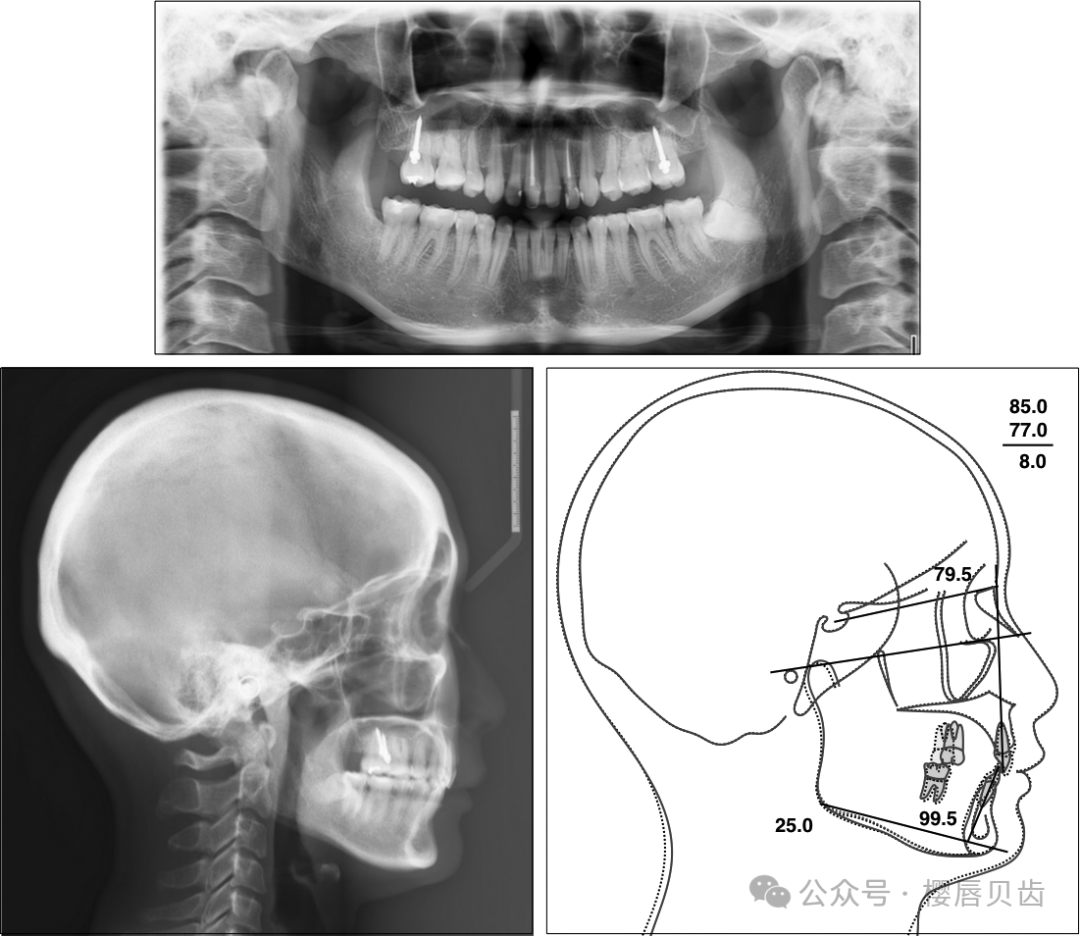
The panoramic radiograph revealed a mesially angulated impaction of the mandibular left third molar (Figure 3). None of the other third molars were present. Endodontic fillings were noted at the maxillary right central incisor and the maxillary left lateral incisor. The periodontal condition was fair despite the uneven gingival line in the maxillary anterior region.
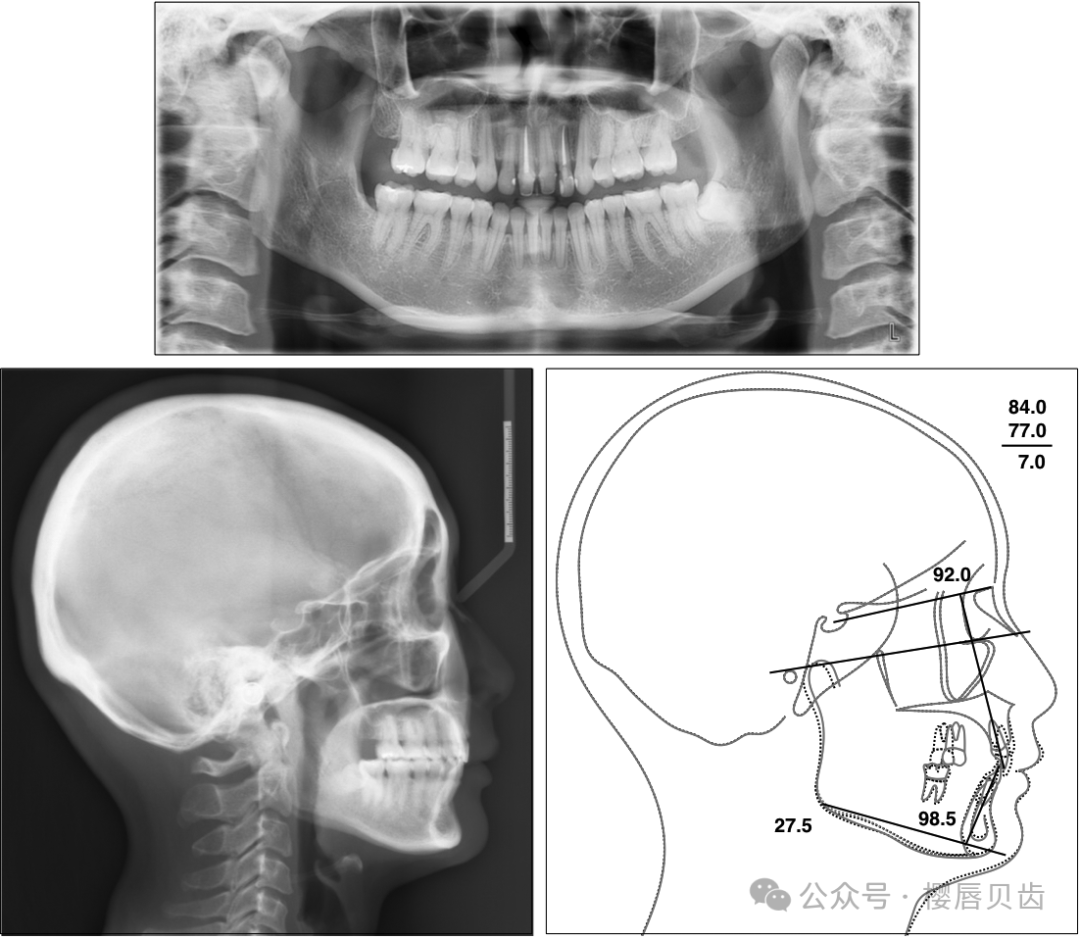
Figure 3.
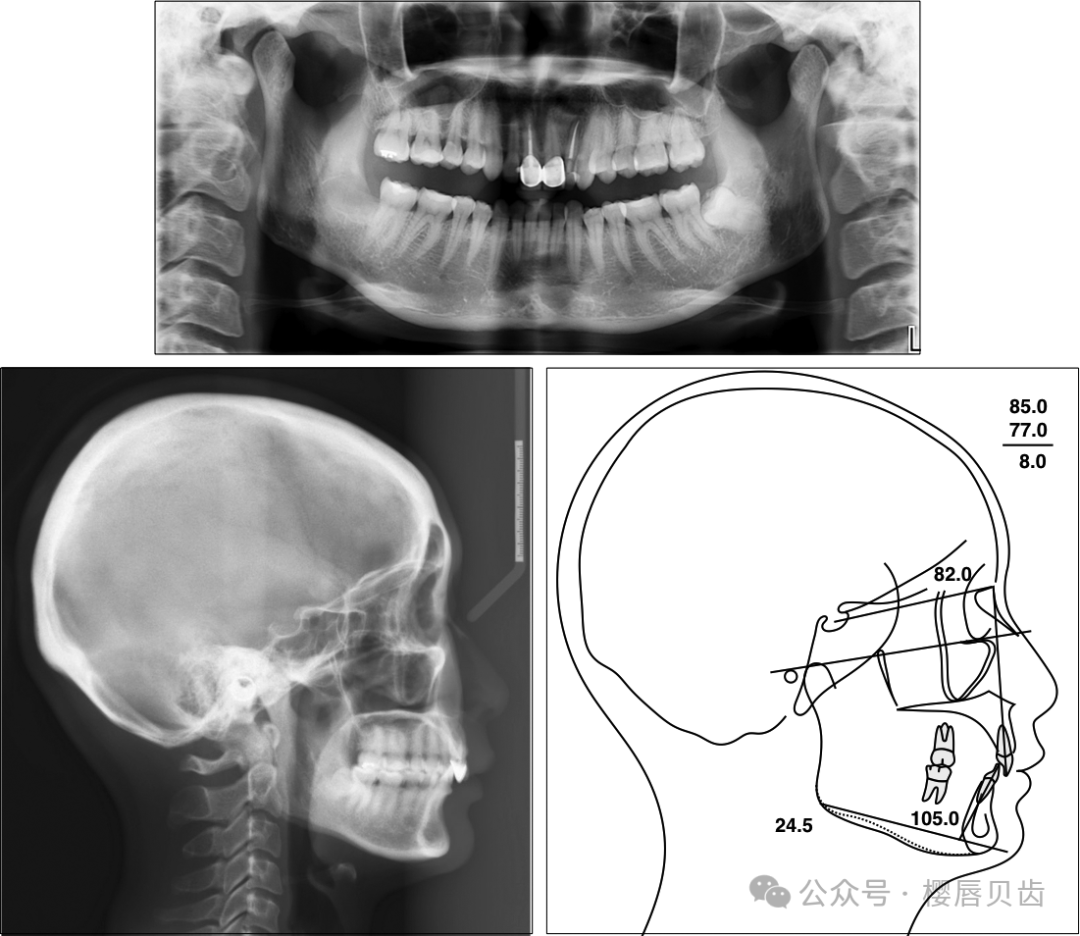
Pretreatment panoramic radiograph and lateral cephalogram.
Treatment Alternatives Treatment Alternatives
The treatment alternatives for Class II division 2 malocclusion may include growth modification, dental compensation, and combined surgical–orthodontic therapy. The deep bite can be corrected by incisor intrusion, molar extrusion, or a combination of both. The treatment modality of choice depends on age, growth potential, facial profile, the severity of malocclusion, skeletal pattern, and preferences of the patient. Because the patient was an adult, growth modification was not a consideration.
The following three treatment options were proposed to this patient:
-
Option 1: Combined surgical–orthodontic therapy with a nonextraction approach.
-
Option 2: Total arch distalization with skeletal anchorage in the maxillary arch for Class II correction. (Bilateral infrazygomatic crest [IZC] temporary skeletal anchorage devices [TSADs] were required to distalize the whole maxillary arch.)
-
Option 3: Maxillary first premolar extractions to reduce the maxillary protrusion and finish at a full-cusp Class II molar relationship.
If space gained by the arch form expansion were insufficient for uprighting the proclined mandibular incisors, Class III elastics supported with IZC TSADs or interproximal reduction might be considered.
Combined surgical–orthodontic therapy might be the treatment of choice to correct the skeletal discrepancy and malocclusion at the same time, optimizing esthetics and function. However, it was declined by the patient. In consideration of the deep bite, retroclination of the maxillary incisors, and heavy occlusal force in low-angle cases, the nonextraction approach was preferred. After a thorough discussion, it was decided to attempt option 2 with aligners first, with the understanding that option 3 might be necessary if Class II correction was not achieved successfully with total arch distalization. The impacted mandibular left third molar was planned for extraction before orthodontic treatment, but the patient did not follow through with this recommendation.
Treatment Progress Treatment Progress
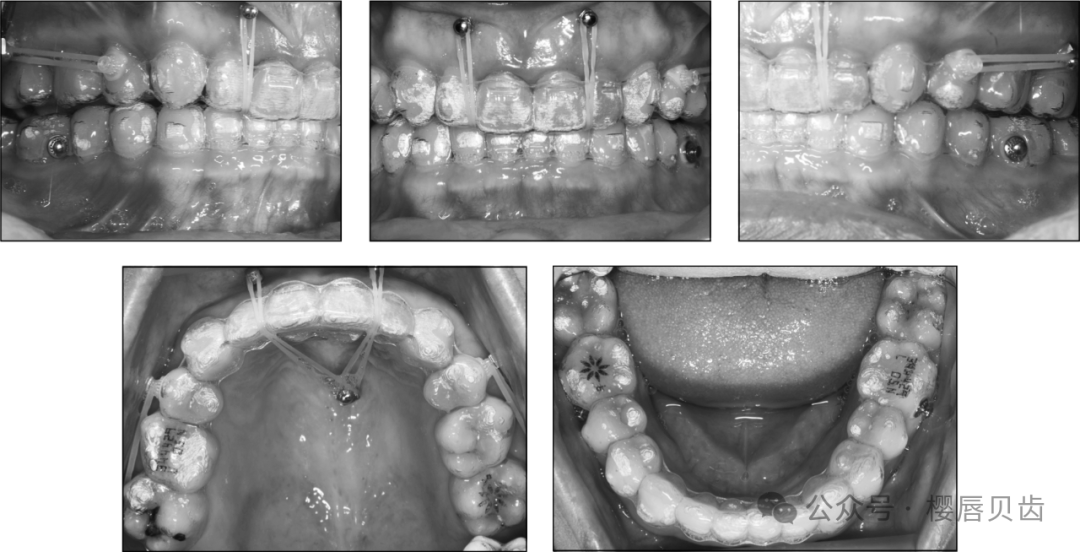
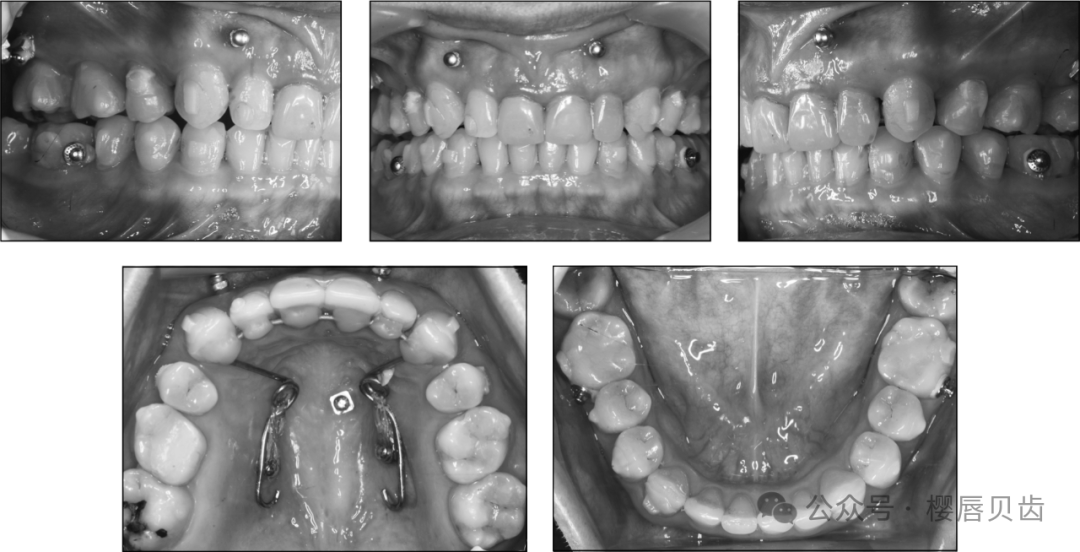
After the old prostheses were replaced with provisional crowns, an intraoral scan was taken for the virtual design of clear aligners. Sequential maxillary molar distalization and interproximal reduction were planned in 92 sets of clear aligners with a 7-day protocol. A minimum of 22 hours of wear per day was suggested. The IZC miniscrews were inserted in the fifth month to support sequential molar distalization with elastics (3/16 inches, 6 oz; Ormco, Orange, Calif) from the miniscrews to the buttons on the labial cervical area of the maxillary canines. Class II elastics were also prescribed from the mandibular first molars to the maxillary canines to enhance Class II correction (Figure 4). Reevaluation in the 15th month after the first round of aligners showed incomplete Class II correction, especially on the right side. It was decided to change the treatment plan to maxillary first premolar extractions (Figure 5).
Figure 4.
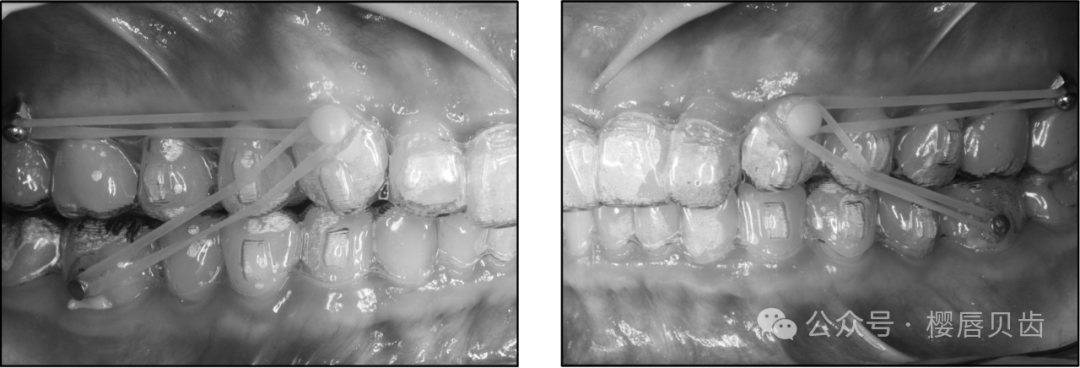
Bilateral IZC miniscrews and Class II elastics were used for a nonextraction approach.
Figure 5.

Treatment Results Treatment Results
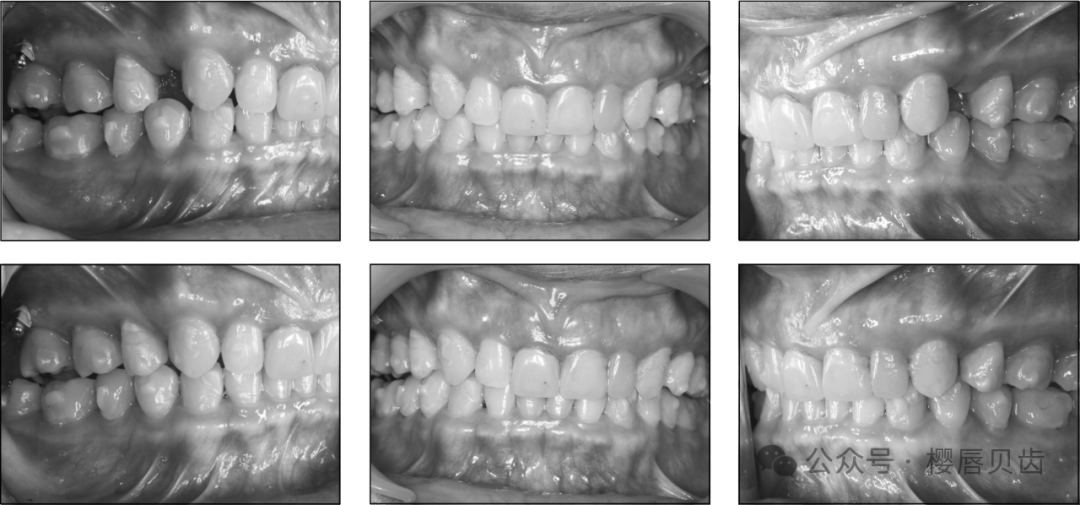
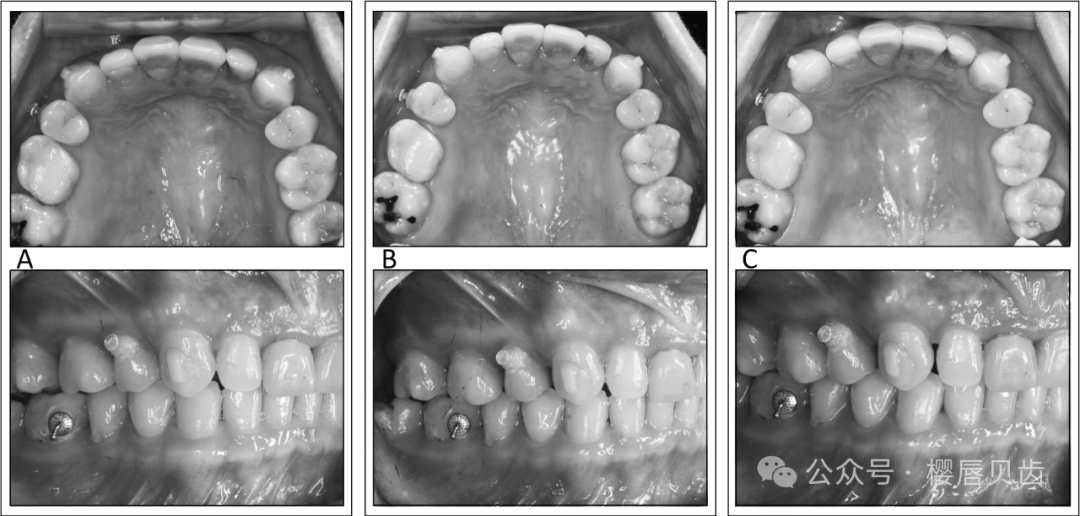
The total treatment time was 52 months, with 130 sets of clear aligners in five rounds. The posttreatment records showed well-aligned teeth in both arches with solid interdigitation (Figures 12–14). Optimal overjet and overbite were achieved. Bilateral molar relationships were complete Class II, and canine relationships were end-on Class II. The protrusion was reduced, and the patient was satisfied with the treatment outcome, although the mandibular dental midline was still deviated to the right by about 0.5 mm.
Figure 12.

DISCUSSION Discussion
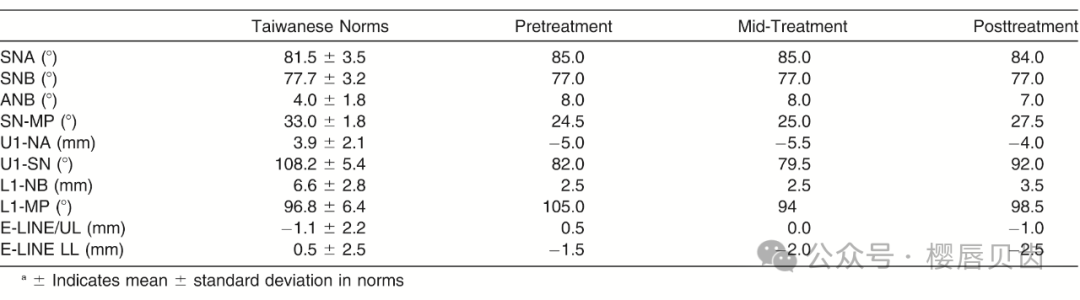
A Class II division 2 malocclusion is characterized by a deep overbite and retroclination of the maxillary central incisors. Although Class II skeletal and molar relationships exist, these patients usually show a balanced soft tissue facial profile with a prominent chin. In addition to reduced U1-SN, indicating retroclined maxillary incisors, the cephalometric measurements usually also indicate reduced lower anterior facial height, small gonial angle, and a large interincisal angle. To correct the deep bite and retroclined maxillary incisors, aligning without extraction is preferable, as space closure is often associated with further retroclination of the incisors and bite deepening. Therefore, a nonextraction approach was attempted in the present patient with sequential molar distalization using aligners. IZC miniscrews were installed for anchorage reinforcement by attaching latex elastics (3/16 inches, 6 oz) from the miniscrews to the bonded clear buttons on the maxillary canines. Class II elastics were also used at the same time from the buttons on the mandibular first molars to those on the maxillary canines.
Progress records at the 15th month showed incomplete Class II correction. The molar relationships were end-on bilaterally. Looking at the coronal view of cone beam computed tomography (CBCT) images, the distal end of the alveolar trough distal to the distobuccal roots of the maxillary second molars diminished in width, which led to insufficient bone for further molar distalization at the root level. Although the constriction of the alveolar trough was not as obvious as the lingual concavity of the mandibular alveolar trough, respecting the anatomical bony boundaries is always a treatment consideration. Therefore, it was decided that option 3 should be pursued, and maxillary first premolars were extracted. The main reason for the failure of total arch distalization of the maxillary arch was the anatomical limitation of alveolar bone, which could have been identified earlier by checking the CBCT. The total treatment time could have been significantly reduced to improve treatment efficiency.
The transverse dimension of the alveolar trough might be one of the limiting factors for further molar distalization to achieve complete Class II correction. A indicates anterior; L, left; p, posterior; and r, right.
In any extraction case, there is a tendency for loss of torque, deepening of the overbite, and retroclination of incisors, leading to what is commonly called a “drawbridge” effect. If the loss of torque and loss of vertical control is excessive, severe deepening of the overbite and premature incisor contact can result, leading to a posterior open bite. In fixed edgewise mechanotherapy, the treatment effects are primarily extrusive in nature with elastic wear, resulting in concurrent extrusion of the lower posterior and upper anterior segments. This may or may not be desirable depending on the initial smile esthetics of the patient. In clear aligner biomechanics, the same tendencies for the loss of upper incisor torque and resultant deepening of the overbite are also potential complications of extraction cases.
Align Technology (San Jose, Calif) launched an innovation called G6 to overcome these issues specifically. Force systems, called “SmartForce” features, are built into the aligners to simulate Tweed tip back bends, which prepare molar anchorage before anterior retraction to maximize anchorage. In the anterior part of the aligner, additional incisor palatal root torque with intrusive forces is built into the aligner to counteract the loss of torque and deepening of the overbite. These force systems are applied to both the upper and lower arches in extraction cases treated with clear aligners.
Even with the advent of SmartForce features, extraction aligner treatment is still quite challenging. A comparison of achieved and predicted tooth movement of maxillary first molars and central incisors in 30 first premolar extraction treatments with Invisalign (Align Technology) was reported by Dai et al. in 2019. Most cases in that study were maximum anchorage cases with an average predicted mesial translation of 0.9 mm for the upper first molars. However, analyses revealed that the first molars actually moved mesially by 3.2 mm. Also, the amount of achieved retraction of the incisors was lower than predicted, and the amount of lingual inclination and extrusion of the upper incisors was greater than what was predicted.
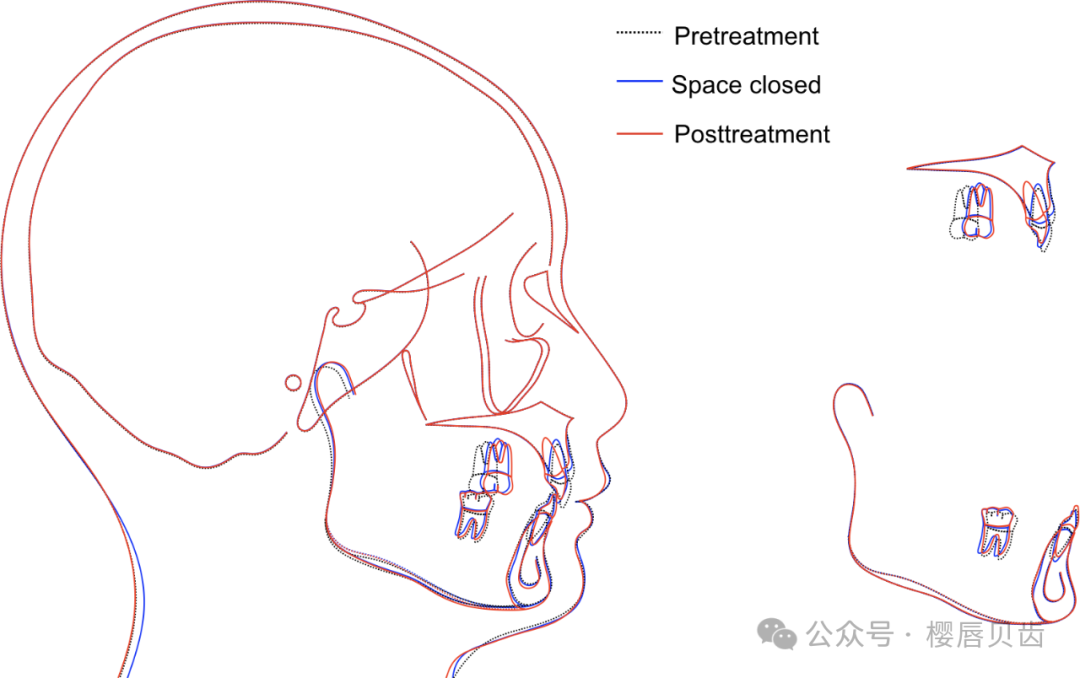
To correct the deep bite in Class II division 2 malocclusion, it might be more stable to focus on incisor intrusion, as heavy occlusal forces may impede molar extrusion or cause relapse of any molar extrusion that occurs. Therefore, two anterior TSADs were used interdentally between the maxillary central and lateral incisors. The cephalometric superimpositions revealed 1.2 mm of intrusion of the maxillary incisors during the 8 months of using anterior TSADs. In addition to the vertical effect of incisor intrusion, the use of anterior TSADs might be beneficial for regaining torque. Liu et al. reported a finite element study in 2021 and suggested that anterior miniscrews and elastics can achieve incisor intrusion and palatal root torquing. However, a coronal view of the CBCT image showed the proximity of anterior TSADs with the incisor roots, which was unfavorable for any root movement.
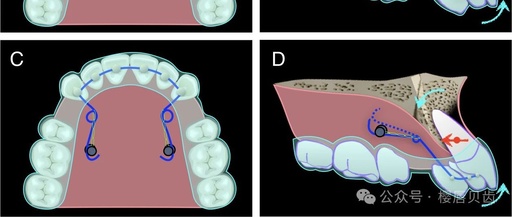
The DJR is a lingual retractor designed for retracting incisors bodily via lever arm mechanics, even without the labial braces. It was first described in 2010 by Jang et al. in a finite element study to locate the center of resistance of the six maxillary anterior teeth. It was suggested that the center of resistance of the six maxillary anterior teeth was 12.2-mm apical to the incisal edge and that the implant position should be 8 mm from the cervical line of the first molar. Torquing springs with helices are designed to slide along the palatal miniscrews to enhance incisor torque control during en-masse space closure. In 2011, Joo reported anterior retraction with a DJR system. He modified the torquing springs, supporting them with up-and-down elastics. In 2012, Park et al. used Class II elastics to support the torquing springs. Liaw et al. reported two cases in 2022, following Jang’s design of the DJR, and achieved very good torque control of the maxillary incisors.
CONCLUSIONS Conclusions
-
In a Class II division 2 case with retroclined maxillary incisors, a modified DJR was used for recovering the torque loss after space closure. The modifications included omitting the two extended lever arms to facilitate wear and removal of the clear aligners and using the helices of the torquing springs to attach elastomeric chains from the palatal miniscrews. This made the line of action higher than the center of resistance and further enhanced the palatal root movement.
-
The modified DJR can be a viable option for aligner patients who undergo extraction treatment and need excellent torque control.