※※Building a Medical Imaging Platform for Imaging Professionals※※
◎Make Learning a Habit◎Make Knowledge an Essence
◎Make Expertise a Communication◎Let Us Become Lifelong Friends
※※※※※※※※※※※※※※※※※※※※※
A few days ago, I stumbled upon a piece of literature that piqued my interest while searching through references, so I decided to read it. Why was I interested? Initially, I didn’t think there was anything specific about lesions in the middle cerebellar peduncle, but after reading, I found it quite enlightening, and today I would like to share it with you.
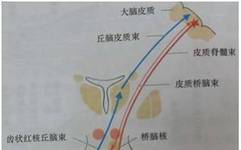
First, I flipped through the anatomy of the middle cerebellar peduncle (middle cerebellar peduncle, MCP), which originates from the base of the pons and is located on the outer side of the three cerebellar peduncles. The inner side is the inferior cerebellar peduncle, and the superior cerebellar peduncle is slightly more anterior (refer to an anatomy book if unclear).MCP contains only afferent fibers.MCP is mainly composed of white matter fibers originating from the contralateral pontine nuclei. The pontine nuclei are an intermediate gray matter, scattered throughout the base of the pons, and are part of the cortical–pons–cerebellum pathway. The superior cerebellar peduncle is the only efferent fiber, and the signal transmission from the dentate nucleus to the cortex is through the dentate nucleus–red nucleus–thalamic bundle connection. The cerebellar pathway crosses twice, once at the level of the pons (transverse pontine fibers) and once at the inferior colliculus of the midbrain (crossing of the superior cerebellar peduncle). Therefore,MCP damage manifests as ipsilateral limb ataxia. See the image below.
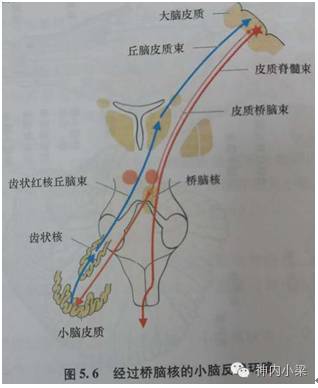
Next, here is an anatomical diagram of the transverse pontine fibers. The cortical fibers from the midbrain and cerebral peduncles terminate at the pontine nuclei, and the axons of these cells give rise to the transverse pontine fibers, which cross the midline and intersect with the corticospinal tract and the corticobulbar tract, dividing into many small bundles. The transverse pontine fibers enter the middle cerebellar peduncle and distribute in the cerebellar hemispheres. (The cause of the “trident sign” is due to central myelinolysis.)

Now, let’s start discussing the lesions affecting theMCP.
1、Demyelination
MS、ADEM、Progressive Multifocal Leukoencephalopathy (PML)、Immune Reconstitution Syndrome.
A 40-year-old female patient diagnosed withMS.
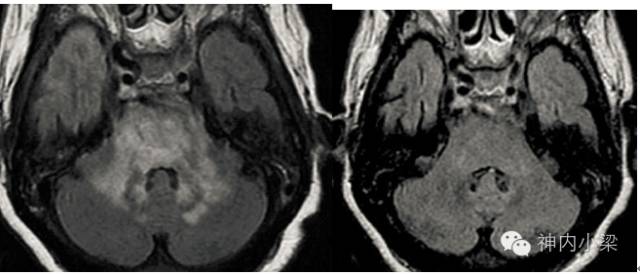
HIVpatients withJCvirus infection. The left image shows bilateralMCP involvement, and the right image shows involvement of the subcorticalUfibers. PML generally does not present as a mass effect or enhancement.
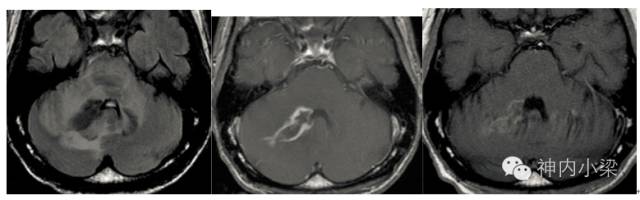
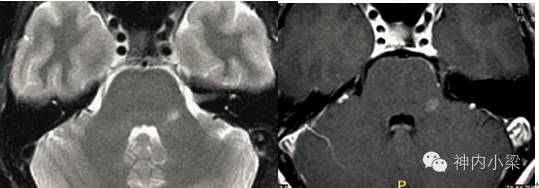
HIV+JCvirus infection patients intermittently treated with antiretroviral drugs. The left image shows diffuse high signal in bilateralMCP, the middle image shows enhancement on the right side, and the right image shows the status two months after treatment with steroids and antiretroviral therapy. Generally,HIVpatients do not show enhancement in PML, but when enhancement occurs, consider immune reconstitution syndrome, tumors, or viral and bacterial infections.
2、Vascular/Toxicity
Reversible posterior leukoencephalopathy due to vascular regulation disorders.18% of reversible posterior leukoencephalopathy involves the brainstem. The causes are varied, such as medications like cyclosporine.
The left image shows bilateralMCPinvolvement, and the right image shows abnormal signals disappearing on a three-month follow-up.
3、Metabolic and Toxicity
Osmotic demyelination, heroin use, toluene and methotrexate toxicity, and less commonWilsondisease.
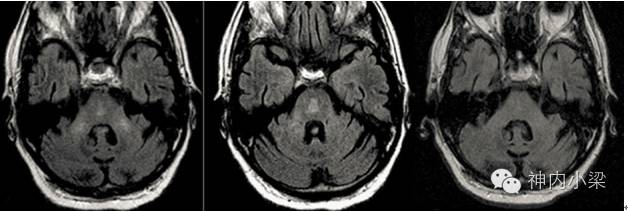
Osmotic demyelination patients present with the “trident sign” in the pons (the reason for this was previously mentioned regarding the transverse pontine fibers, damaging the transverse pontine fibers without affecting the corticospinal tract and corticobulbar tract, combined with the anatomical diagram, it resembles a trident, which is not typical). The final image shows what was seen during follow-up.
4、Vascular/Infarction
Infarction in the blood supply area of the anterior inferior cerebellar artery leads to pontine arm infarction. Additionally, pontine infarction causes Wallerian degeneration of the pontine arms. Cavernous hemangioma.
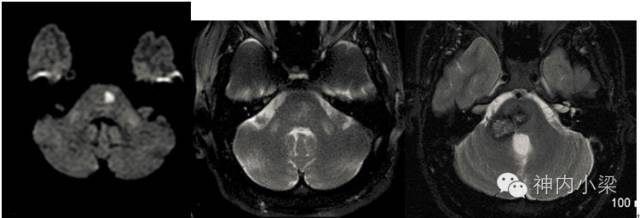
The left image shows a restricted diffusion lesion in the left pons; the middle image shows symmetrical bilateral Wallerian degeneration of the pontine arms. The right image is of a cavernous hemangioma.
5、Degenerative Diseases
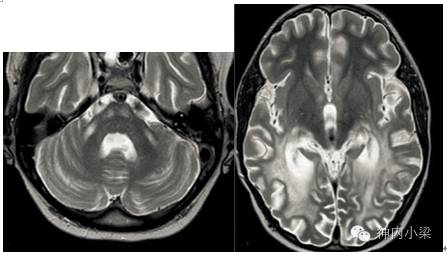
MSA-Cpatients show43% with high T2 signal in the middle cerebellar peduncle, often accompanied by atrophy.
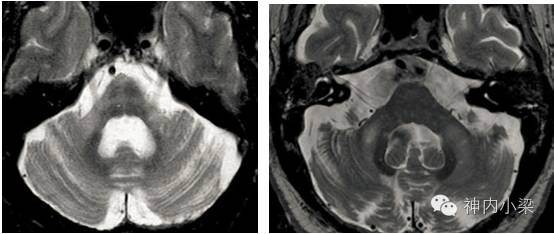
The left image shows an MSA-C patient with a typical “cross-bun sign” accompanied by abnormal signals in the bilateral pontine arms and pontine atrophy; the right image shows a patient with fragileXchromosome-related tremor-ataxia syndrome,where up to82% of patients exhibit T2 high signal in the pontine arms (known as the middle cerebellar peduncle sign, though not specific).
6、Leukodystrophy
Leukodystrophy is a hereditary metabolic disorder caused by a lack of substances necessary for myelination, leading to leukodystrophy. Leukodystrophy is often associated with peroxisomal or lysosomal deficiencies such as (adrenoleukodystrophy, metachromatic leukodystrophy).LD can affectMCP, however, it is often accompanied by symmetrical damage to the supratentorial white matter and generally does not accumulateUfibers.
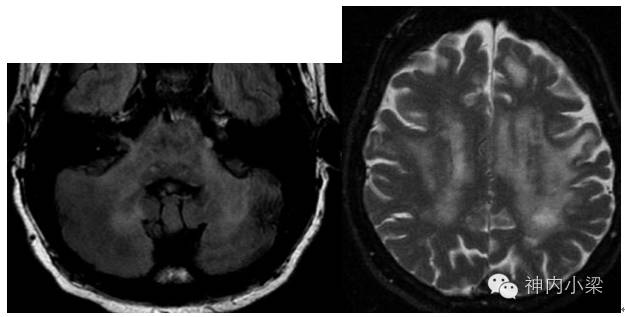
A patient with adrenoleukodystrophy. The left image shows abnormal signals in bilateralMCP and corticospinal tract; the right image shows typical symmetrical abnormal signals in the parieto-occipital region.
7、Infection
The most common infections are viral, including varicella, mumps, measles, rubella, rotavirus, etc. Rarely, there are bacterial infections such as Lyme disease, Listeria,Whippledisease.
This WeChat platform is a personal public welfare medical imaging learning platform. All articles reprinted on this WeChat are for the purpose of conveying more information and are clearly marked with sources and authors. All reprinted videos are for grassroots teaching purposes, and the name of the teaching expert is clearly indicated. If the original author or teacher does not wish to be reprinted, please contact us, and we will immediately take action to delete it.