
When mentioning Merkel cell carcinoma, some colleagues may assume that this tumor originates from the Merkel cells of the epidermis. In fact, the reason it is named Merkel cell carcinoma is that the tumor cells are morphologically, immunophenotypically, and ultrastructurally similar to normal Merkel cells, and do not originate from them!
Merkel cell carcinoma (MCC) is a rare, highly aggressive, primary cutaneous neuroendocrine malignant tumor, prone to local recurrence, with a high tendency for regional lymph node and distant metastases, and a mortality rate as high as 33%-46%[1]. The prognosis is often poor, and clinical manifestations can be non-specific, leading to delayed diagnosis. Therefore, dermatologists and oncologists need to understand and recognize this disease.
History
● In 1875, Friedrich Sigmund Merkel first described Merkel cells and believed that these cells might be tactile receptors closely related to nerve endings[2];
● In 1972, Toker first described this disease and named it “trabecular carcinoma of the skin” based on histopathological patterns, believing it to be a subtype of sweat gland carcinoma[3];
● In 1978, Tang and Toker confirmed the presence of neuroendocrine granules in trabecular carcinoma cells, and because the ultrastructure of these tumor cells was similar to that of normal Merkel cells, they named it “Merkel cell carcinoma”[4];
● In 2008, Feng et al.[5] discovered a new polyomavirus closely related to MCC, naming it Merkel cell polyomavirus (MCPyV);
● In 2008, Heath et al.[6] found that most MCCs exhibit clinical features of “AEIOU” (see Table 2), which can be used for the preliminary diagnosis of MCC;
● In 2010, the American Joint Committee on Cancer (AJCC) first proposed a staging/prognostic system for MCC based on an analysis of 5823 cases from the National Cancer Database (NCDB);
● In 2017, AJCC revised the staging system again based on an analysis of 9387 MCC patients diagnosed from 1998 to 2012, leading to the 8th edition AJCC staging system[8].
Etiology and Pathogenesis
Cell Origin
Merkel cells are dendritic cells located in the basal layer of the epidermis. In terms of cell morphology, immunophenotype, and ultrastructure, MCC cells are similar to normal Merkel cells, leading to the initial belief that MCC originates from Merkel cells. Despite significant progress in research on MCC, the cell origin of MCC remains unclear and controversial. Most scholars do not believe that MCC cells are derived from Merkel cells, as Merkel cells are post-mitotic in vivo, and the anatomical location with the highest density of Merkel cells is not the most common site for MCC tumor cells. Currently, it is believed that MCC may originate from progenitor B cells or pre-B cells, fibroblasts, dermal mesenchymal stem cells, or epidermal precursor cells[9].
The etiology and pathogenesis of MCC are not fully elucidated. It is currently believed that Merkel cell polyomavirus and ultraviolet-induced mutations are the two main pathogenic factors of MCC.
1. Merkel Cell Polyomavirus (MCPyV)
MCPyV is a double-stranded DNA virus in the polyomavirus family, with a full length of 5387 bp. The MCPyV genome encodes large T antigen (LT), small T antigen (ST), 57KT antigen, and a protein called alternative large T open reading frame (ALTO) (Figure 1[10]). Humans typically become infected with MCPyV during childhood, and it can be detected in the skin of most healthy individuals, but only a very small number of people will develop MCC. MCPyV DNA can be detected in 75-89% of MCC cases.
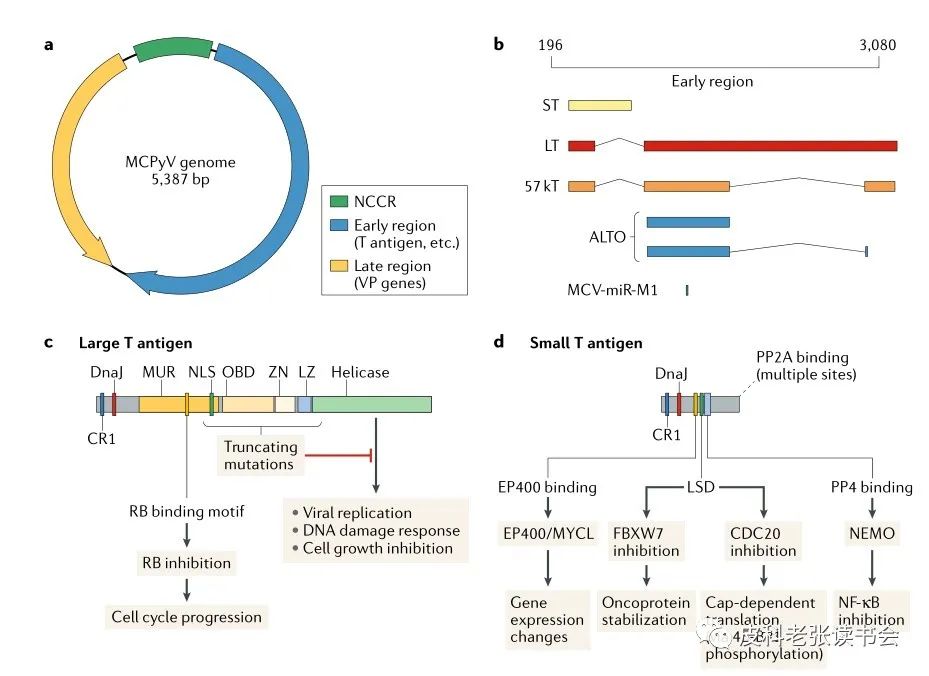
Figure 1 Structure and functional diagram of Merkel cell polyomavirus
2. Ultraviolet Exposure
Ultraviolet exposure can lead to DNA damage, inducing mutations in the viral genome that drive tumorigenesis, thereby evading host immune responses and promoting tumor cell proliferation. Furthermore, ultraviolet exposure can also cause local immunosuppression, playing a role in viral carcinogenesis. Ultraviolet irradiation can also induce the expression of inflammatory mediators and alter the function of antigen-presenting dendritic cells, leading to immune system dysregulation[9].
Therefore, the pathogenesis of MCC is currently classified into two types: virus-negative (MCPyV-Negative MCC, VN-MCC) and virus-positive (MCPyV-Positive MCC, VP-MCC), which have different mechanisms promoting cell growth and proliferation (Figure 2[10]). In VN-MCC, due to ultraviolet-mediated DNA damage to the progenitor cells, there is a high tumor mutation burden and inactivation of tumor suppressor genes (such as RB1 and TP53); in VP-MCC, MCPyV integrates into the human genome, with viral T antigens constitutively expressed as LT and ST, altering the behavior of tumor suppressor proteins and cell cycle regulatory proteins, promoting the occurrence of MCPyV-induced MCC, as detailed in Figure 3[11].
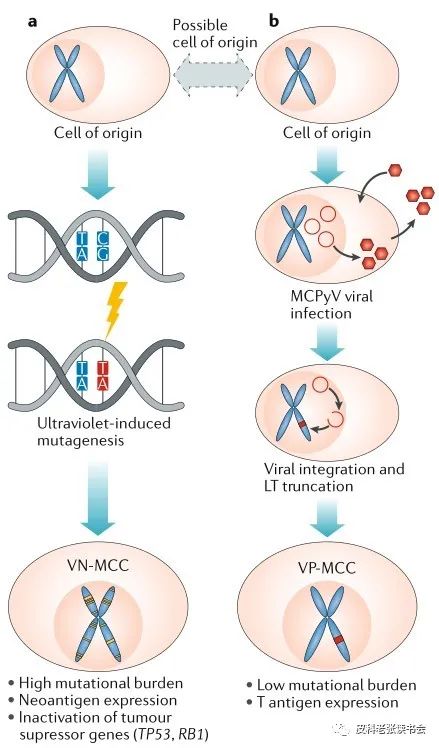
Figure 2 Pathways of virus-negative and virus-positive MCC
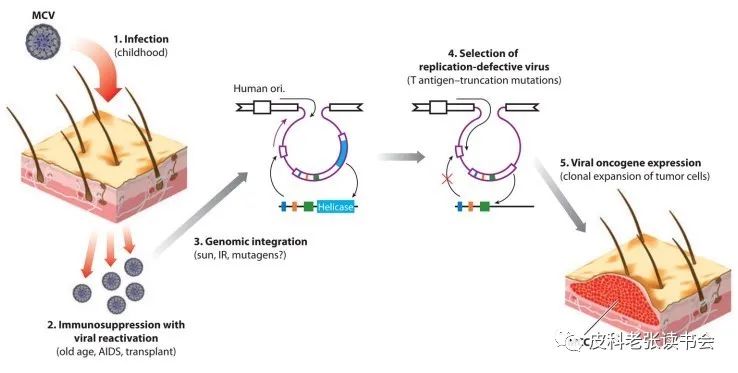
Figure 3 Viral infection process in MCC patients
(1) MCV infection is widespread in the population and is acquired early in childhood, being a component easily detected in the normal skin microbiota; (2) when the body’s immunity declines (due to aging or disease), MCV may reactivate; (3) viral infection outbreaks promote viral integration in susceptible cells; (4) due to cell lysis, cells infected with replicating viruses are selected; (5) MCV tumor antigens (T antigens) are expressed in cells with integrated viral truncated mutations, providing proliferation signals for the occurrence of MCC.
3. Chromosomal Abnormalities
In addition to the factors mentioned above, various chromosomal abnormalities have been found in MCC, with the most common being the deletion of 1p36, a structural abnormality found in up to 40% of MCC cases. Other chromosomal abnormalities, such as loss of heterozygosity at 3p21, and abnormalities at 10q23 and chromosome 13, have also been reported[12].
Risk Factors
In addition to ultraviolet exposure, the risk of developing MCC is also significantly increased in other malignancies such as chronic lymphocytic leukemia (Figure 4[13]) and in immunocompromised individuals (such as HIV patients and those on immunosuppressants). Compared to the general population, HIV-infected individuals have a relative risk of 13.4 for developing MCC, and organ transplant recipients have a 4.59-fold increased risk[14].
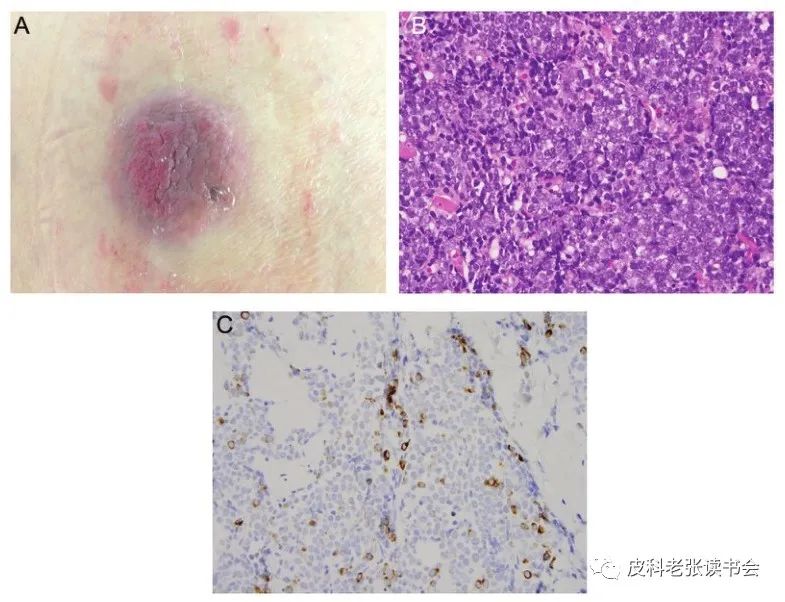
Figure 4 77-year-old patient with chronic lymphocytic leukemia
A. A solitary, asymptomatic, firm, movable purple subcutaneous nodule on the back; B. Histopathology shows single small cell infiltration; C. Some tumor cells are CK20 positive.
Epidemiology
● Rare;
● Incidence: approximately 0.24 per 100,000 per year, showing exponential growth, which is related to aging population, the use of immunosuppressants, advancements in diagnostic technology, and increased clinical awareness[12,15];
● Racial and regional characteristics: The incidence of MCC is higher near the equator, with the incidence in Caucasians being 25 times that of other races, but cases have also been reported in Black and Polynesian individuals (Figure 5[16]), suggesting different sensitivities to ultraviolet exposure among different skin colors. Currently, Australia has the highest incidence of MCC (approximately 1.6 per 100,000 per year)[10];
● Population characteristics: More common in individuals with fair skin or those with prolonged sun exposure, older adults (over 75% of patients are over 65 years old, with an average age of diagnosis around 70 years), and males (the male-to-female ratio is 1.4:1 to 2.3:1);
● Prognosis: MCC is highly aggressive, with over one-third of patients dying from the disease, and almost one-third of patients have local or regional metastases at the time of diagnosis. The mortality rate of MCC is three times that of malignant melanoma. The 5-year overall survival rate is 30-64%[17]. Prognostic factors include: ① Active hematologic malignancies or immunocompromised individuals often have a poorer prognosis; ② The degree of infiltration of the primary tumor, growth pattern, and prognosis are related; ③ Virus-positive MCC patients often respond better to immunotherapy and have a better prognosis; ④ Sentinel lymph node involvement is associated with a poorer prognosis[15].
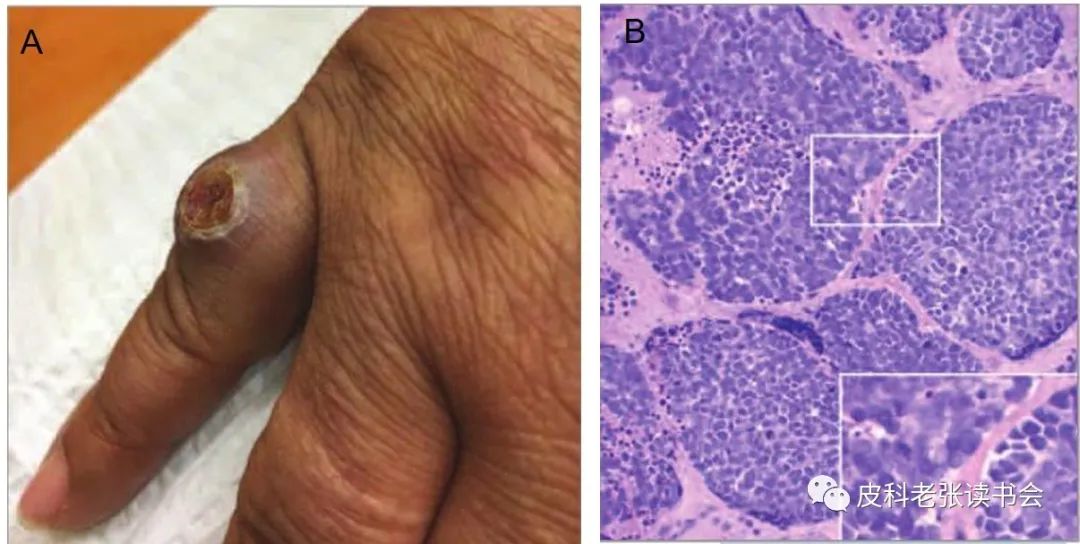
Figure 5 59-year-old Black female
A. A rapidly enlarging, painful nodule on the proximal phalanx of the right little finger; B. Histopathology shows small blue round cell aggregates, with large nuclei and scant cytoplasm.
Clinical Features
Clinical Manifestations
● Location (Figure 6[6]): Most commonly located in sun-exposed areas, with the head and neck being the most common (53%) (Figure 7[12]), other locations include limbs (34-35%), trunk (Figure 8[18]), and occasionally the oral cavity and genital mucosa (<10%) (Figure 9[19]);
● Primary skin lesions: Often present as solitary skin-colored, red, or purple nodules or plaques (Figures 10[20], 11[6]), usually grow rapidly, with a hemispherical outward growth and an iceberg-like growth inward, can be multiple (Figure 12[21]), and may ulcerate or crust (rarely seen in early stages); 15% of patients may experience spontaneous regression of the primary lesion (Figure 13[22]), leading to some cases only showing lymph node metastasis or distant metastasis without identifiable primary lesions;
● Symptoms: Often asymptomatic, occasionally accompanied by itching;
● Metastasis: The most common sites of metastasis are regional lymph nodes (27-60%) (Figures 14[23], 15[24]), followed by distant skin (9-30%), lungs (10-30%), central nervous system (18%), bones (10-15%), and liver (13%); less common distant metastasis sites include testes (Figure 16[25]), pancreas, heart, bone marrow, pleura, salivary glands, gastrointestinal tract, prostate, and bladder.
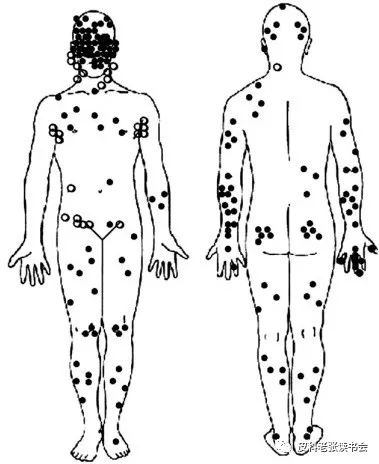
Figure 6 Distribution map of common sites of MCC skin lesions
In 195 patients, 168 (86%) had primary skin lesions (●), and 27 (14%) showed lymph node involvement without visible primary skin lesions (○).

Figure 7 Facial MCC, the tumor grows hemispherically, with ulceration visible in late-stage lesions.

Figure 8 85-year-old male patient
A solid, red, slowly growing skin nodule can be seen on the scar of the sternum for 6 months, prone to bleeding, accompanied by enlarged left axillary lymph nodes, diagnosed as MCC based on histopathology and immunohistochemistry.
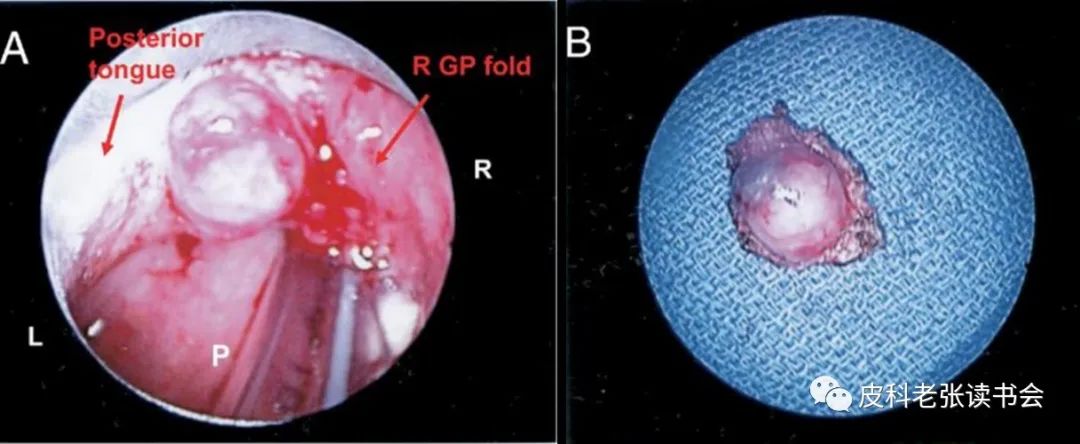
Figure 9 MCC of the tongue and oral mucosa
A. Direct laryngoscopy shows MCC (a raised, painless submucosal mass) located at the circumvallate papilla of the right posterior lateral tongue, near the right glossopharyngeal fold (R right, L left, P posterior pharyngeal wall); B. Gross specimen of a 1.5 cm primary MCC excised.
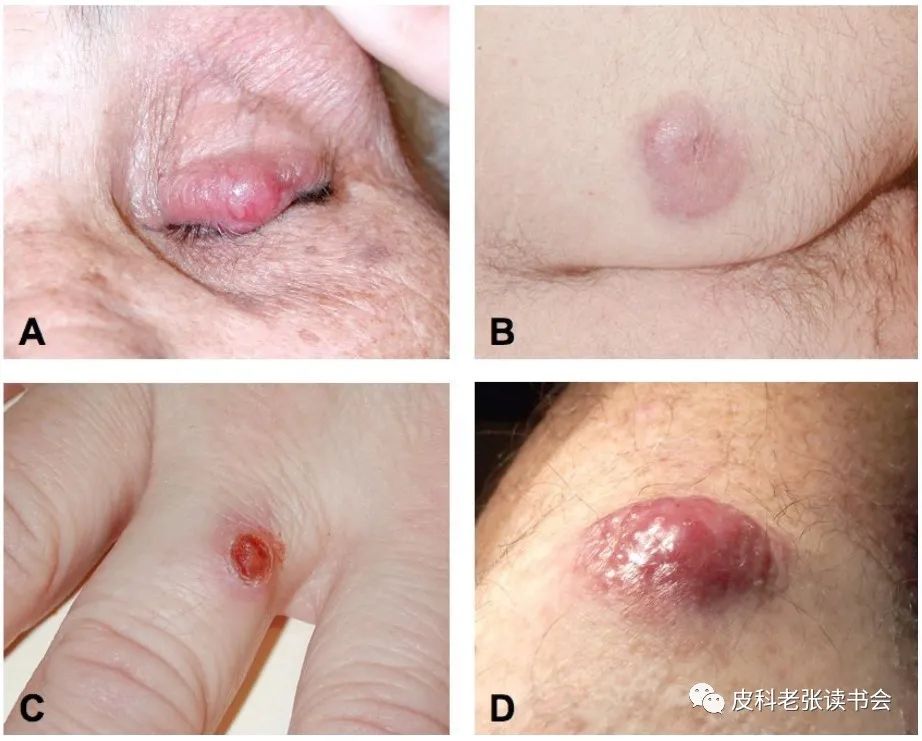
Figure 10 84-year-old female
A rapidly enlarging, painless red nodule can be seen at the base of the right ring finger; B. Histopathology shows nodular infiltration of tumor cells in the dermis.

Figure 11 Clinical manifestations of MCC
A. Red nodule on the eyelid, growing rapidly, previously misdiagnosed as a meibomian gland cyst; B. Painless MCC on the buttock of an HIV patient, diagnosis of which was delayed due to a history of multiple epidermoid cysts; C. Lesion on the extensor side of the finger, clinically suggested as a suppurative granuloma or achromic melanoma; D. MCC on the exposed area of an individual with fair skin.
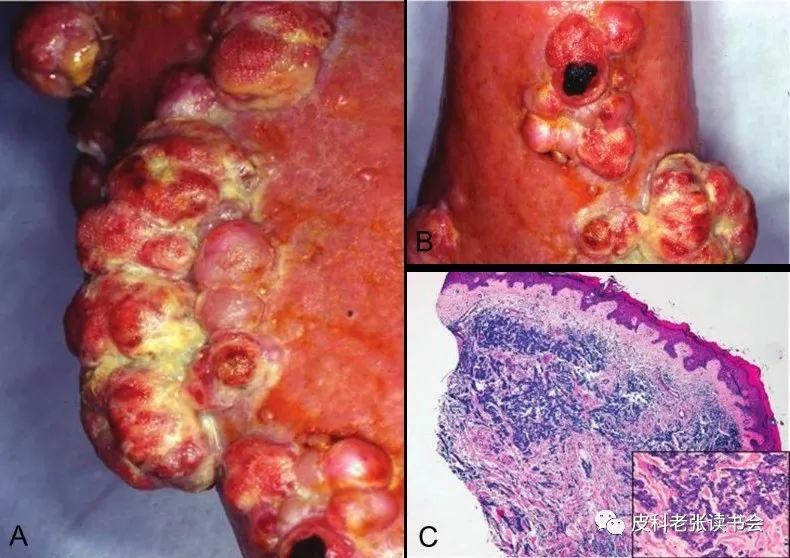
Figure 12 78-year-old female MCC patient
A. Pink dome-shaped, multiple clustered nodules on the left calf; B. The surface of the nodules is covered with yellowish discharge, with local necrosis and ulceration visible; C. Histopathology shows small, uniform round cell infiltration in the dermis, with scant cytoplasm, and round or oval nuclei, with powdery chromatin.
Figure 13 Self-regression of MCC after biopsy
Skin lesion: a. A solitary red nodule on the cheek; b. One month after biopsy, only a scar remains. Histopathology shows diffuse eosinophilic tumor cell infiltration in the dermis; c. Round tumor cells of uniform size, with scant cytoplasm and numerous inflammatory cells; d. Few PD-1 positive cells; e. CD8 positive cells located around the tumor mass.

Figure 14 A. MCC in the left temporal region (3.4 cm), with no lymph node spread (Stage Ib); B. Recurring MCC in the calf, with multiple skin and groin lymph node metastases (Stage II); C. Multiple tumors in the head and neck with local lymph node metastases (Stage II); D. Extensive skin and lymph node metastases after inadequate local treatment.
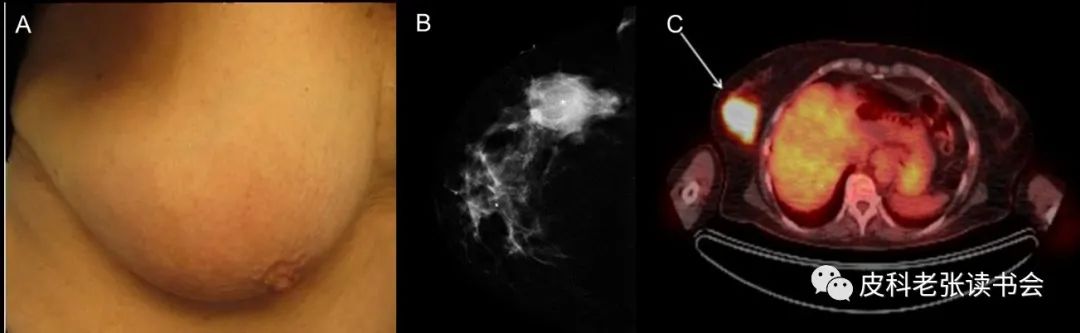
Figure 15 MCC presenting as a subcutaneous mass in the breast
A. No obvious skin lesions, only a pale red patch on the outer side of the right breast; B. X-ray shows a mass in the outer upper quadrant of the right breast; C. PET-CT shows an FDG-positive mass in the right breast (5.0 cm × 4.0 cm), with two lymph node metastases in the axilla.
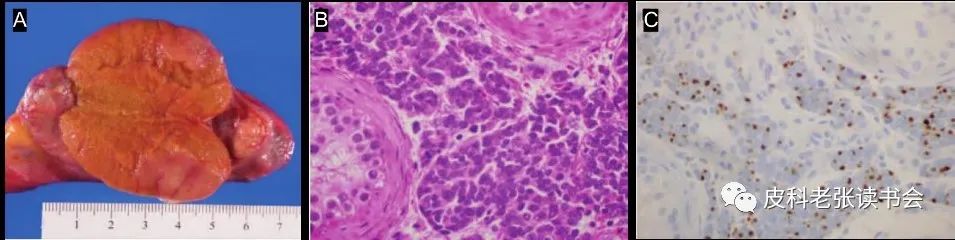
Figure 16 70-year-old Caucasian male, previously with MCC in the right buttock, subsequently developed metastases to the right testis, groin, and anterior thigh sentinel lymph nodes. A. Right radical orchiectomy, with a brownish-yellow to pink, well-defined lobulated mass measuring 2.4 × 1.5 × 1.4 cm at the lower pole; B. Tumor cell infiltration around the seminiferous tubules, with extensive lymphatic invasion, tumor cells being small and round, with scattered chromatin, and abundant mitotic figures; C. CK20 shows perinuclear dot-like positivity.
Dermatoscopy
Non-specific, most commonly showing sparse/dense irregular linear, punctate, and glomerular-like vessels over a cherry-red background, accompanied by a small amount of milky-white unstructured areas (Figures 17, 18[26]).
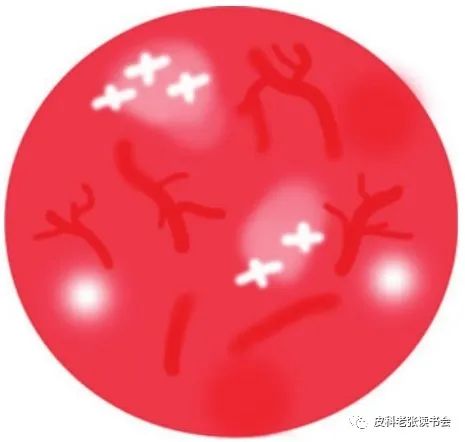
Figure 17 Dermatoscopic pattern of MCC
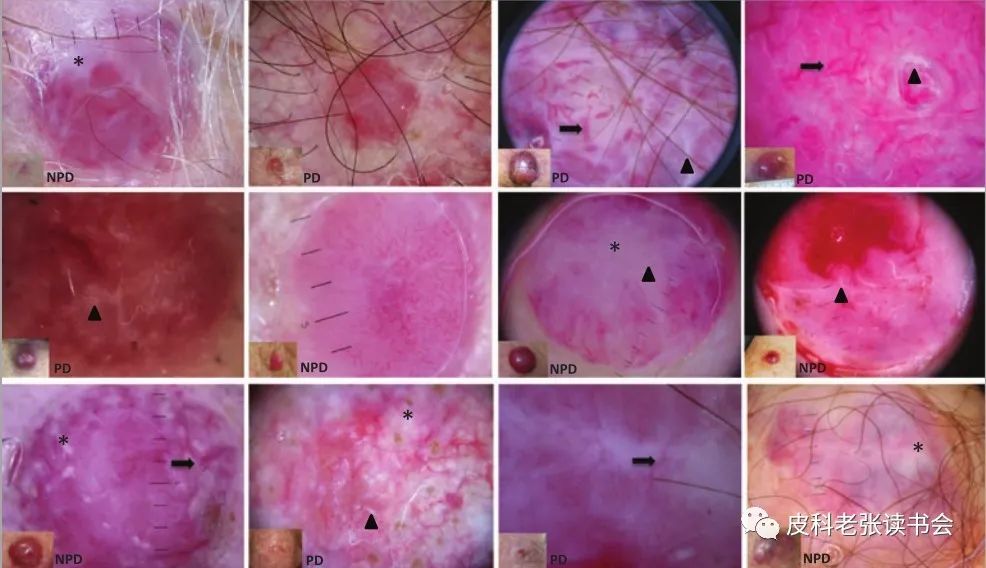
Figure 18 Dermatoscopic features of MCC
*: Non-glossy white areas; ▲: Glossy white areas; Long arrow: Large vessels; PD: Polarized dermatoscope; NPD: Non-polarized dermatoscope.
Skin CT
Solid masses arranged in aggregates of highly reactive small cells can be seen in the fibrous stroma and prominent vascular system (Figure 19[27]).
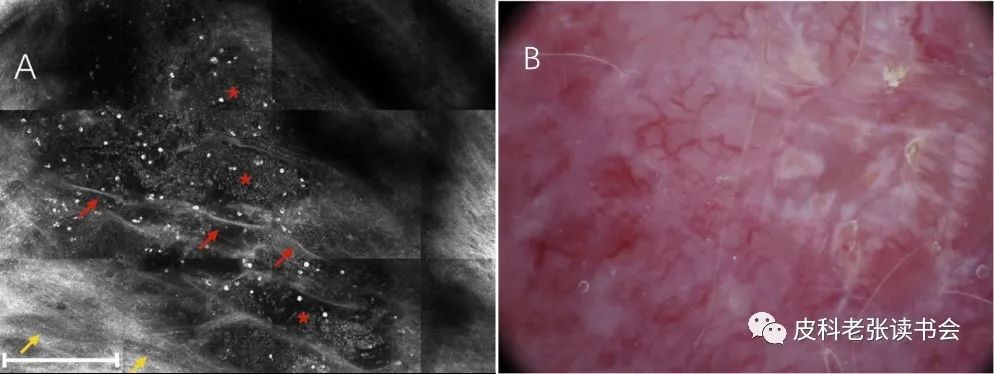
Figure 19 Skin CT and dermatoscopic features of MCC
A. RCM shows small cell aggregates (*) surrounded by fibrous septa (red arrow), with large caliber blood vessels (yellow arrow) surrounding them; B. Dermatoscopy shows irregular branching vessels and milky-white structures on a red background.
Histopathology
Primary Skin Lesions
Histologically, MCC is primarily located in the dermis, consisting of small blue round cells arranged in nests or trabecular patterns, with scant cytoplasm, round to oval nuclei, and “pepper-like” distribution of chromatin, with indistinct nucleoli (Figure 20[10]). The tumor can infiltrate down to the reticular layer of the dermis, generally not involving the dermal papillae (i.e., the Grenz zone), epidermis, and appendages. However, in 5-30% of tumors, the epidermis can be involved, showing an epidermotropic pattern (Figure 21E[28]). Irregular nested infiltration (Figure 21C), giant tumor cell variants (Figure 21D), cellular necrosis, prominent mitotic figures, invasion of blood vessels or lymphatics (Figures 21G, 22[29]), and perineural infiltration can also occur.
Gould et al. described three histopathological patterns (Figure 23[30]): ① Trabecular type (with connective tissue separating interconnected cell trabeculae, tumor cells are slightly larger than in other types, round to polygonal, with abundant cytoplasm); ② Intermediate type (the most common subtype, composed of solid nests surrounded by trabeculae, tumor cells are of medium size, with large lobulated nuclei, scant cytoplasm, and pale staining); ③ Small cell type (the least common, composed of small cell sheets with diffuse infiltration, tumor cells being small, indistinguishable from small cell lung cancer histologically).
Other tumors can accompany MCC lesions or be adjacent to them, including solar keratosis, Bowen’s disease (Figure 21H), invasive squamous cell carcinoma, basal cell carcinoma, and sweat gland tumors.
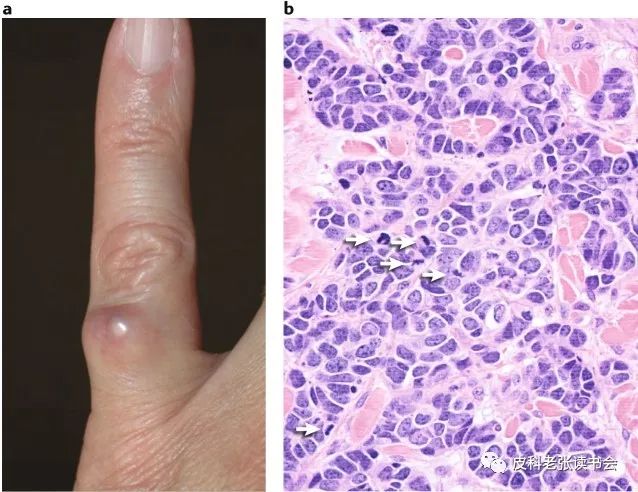
Figure 20 Clinical and histological manifestations of MCC
a. MCC appears as a rapidly growing nodule on the finger; b. Histopathology shows blue round cells exhibiting trabecular infiltration, with scant cytoplasm, neuroendocrine chromatin, and numerous mitotic figures (arrow).
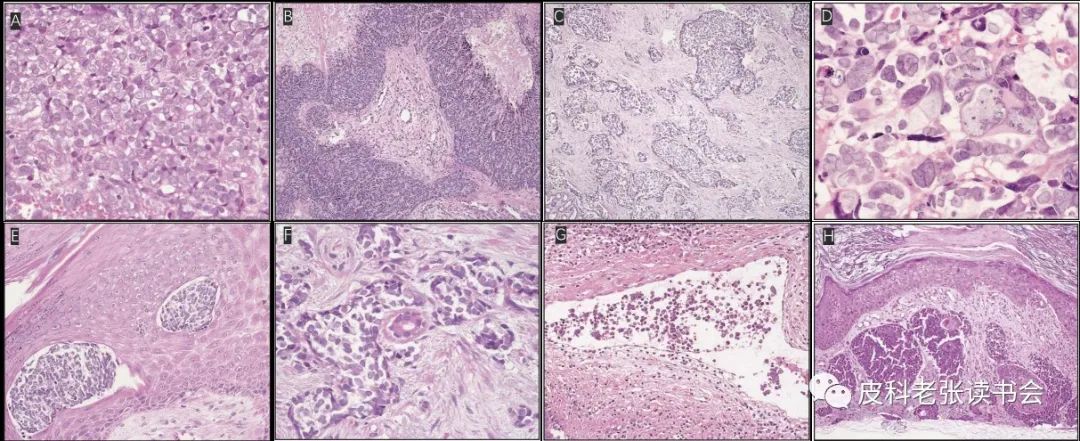
Figure 21 Histopathological features of MCC
A. High magnification shows cytological features of tumor cells. Scant cytoplasm, smooth nuclear contours, and dispersed chromatin can be seen; B. Trabecular infiltration; C. Nodular or nested infiltration; D. Large tumor cell aggregates can be seen, differing in nuclear size and shape, but otherwise similar to traditional MCC; E. Epidermal involvement; F. Sweat glands surrounded by tumor cells; G. Vascular involvement; H. MCC accompanied by Bowen’s disease.
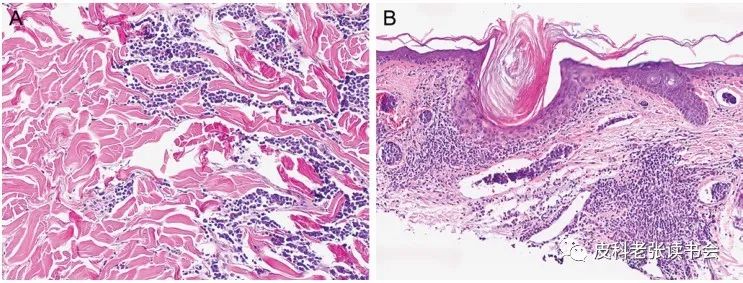
Figure 22 Histopathology of MCC
A. Tumor cells infiltrate and grow through collagen bundles; B. Tumor cell clusters in dilated blood vessels.
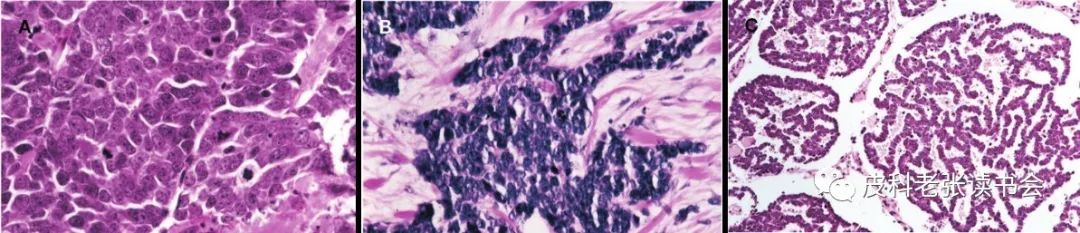
Figure 23 Three histological types of MCC
A. Intermediate type MCC, showing vacuolated eosinophilic nuclei with prominent nucleoli and multiple mitoses; B. Small cell type MCC, histologically indistinguishable from small cell lung cancer; C. Trabecular type MCC, rare, usually considered a small part of mixed subtypes.
Sentinel Lymph Node Biopsy
In MCC, the status of lymph nodes is the strongest predictor of survival and the risk of distant metastasis. Due to the high risk of sentinel lymph node metastasis, even in cases without clinically evident lymph node disease, sentinel lymph node biopsy (SLNB) is routinely recommended for MCC as it maximizes guidance for local treatment of the disease (Figures 24, 25[29]).
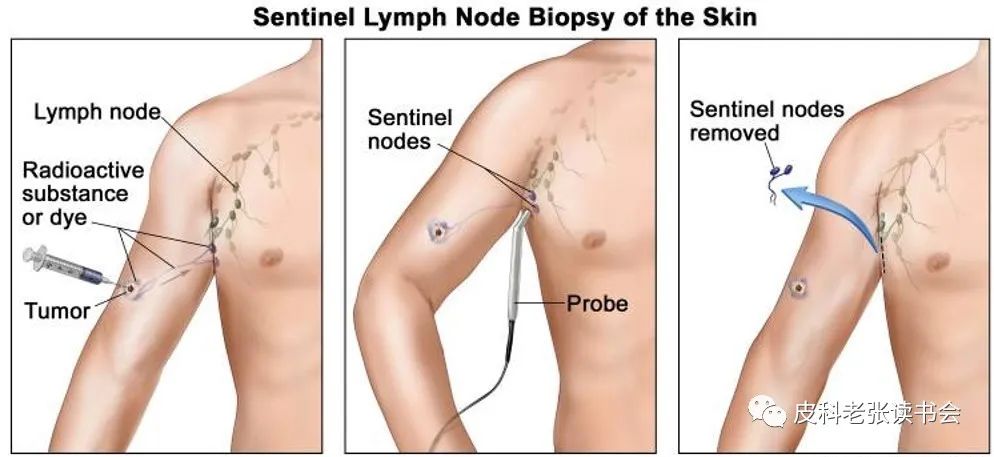
Figure 24 Schematic diagram of sentinel lymph node biopsy
[Source: Online version of literature Merkel Cell Carcinoma Treatment (PDQ®)]
A. Injection of radioactive substances and/or blue dye near the tumor; B. Radioactive probe detection or visual observation of the injected blue dye; C. Sentinel lymph node (the first lymph node detected) is removed and checked for cancer cells.
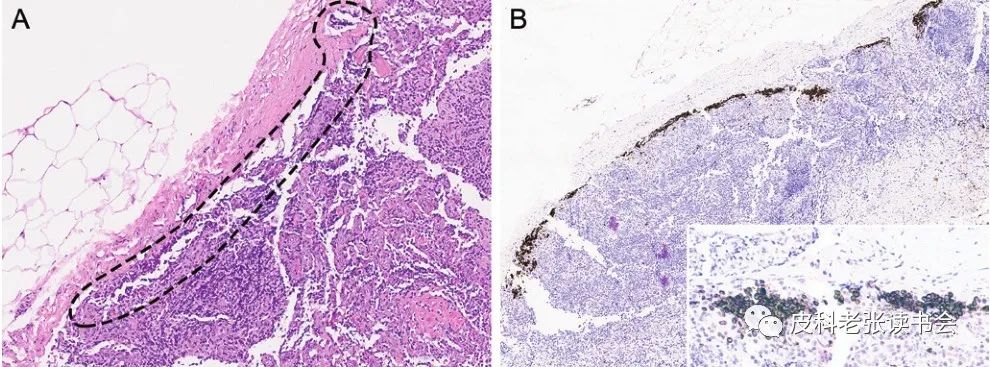
Figure 25 Metastatic MCC in sentinel lymph nodes
A. MCC cells at the dashed line under HE staining; B. MCC cells mainly located in the subcapsular region, positive for broad-spectrum cytokeratin staining (brown).
Immunohistochemistry
The immunohistochemical characteristics of MCC include the simultaneous expression of epithelial markers (AE/1AE3, CAM5.2, broad-spectrum cytokeratin, etc.) and neuroendocrine markers (neurofilament, neuron-specific enolase, etc.). It can also express CD117, CD56, and rarely express CD99 and terminal deoxynucleotidyl transferase (TDT), while thyroid transcription factor 1 (TTF-1), S100, and leukocyte common antigen/CD45 are usually negative (Table 1[31]).
Cytokeratin (CK)20 is a relatively specific and sensitive marker for MCC, usually showing perinuclear dot-like positivity or cytoplasmic positivity (Figures 26[12], 27[18]).
The diagnosis of MCC is generally made using a combination of CK20 and NSE, with the former being highly specific but slightly less sensitive, while the latter is usually highly sensitive but has lower specificity.
Table 1 Positive expression of immunomarkers in MCC

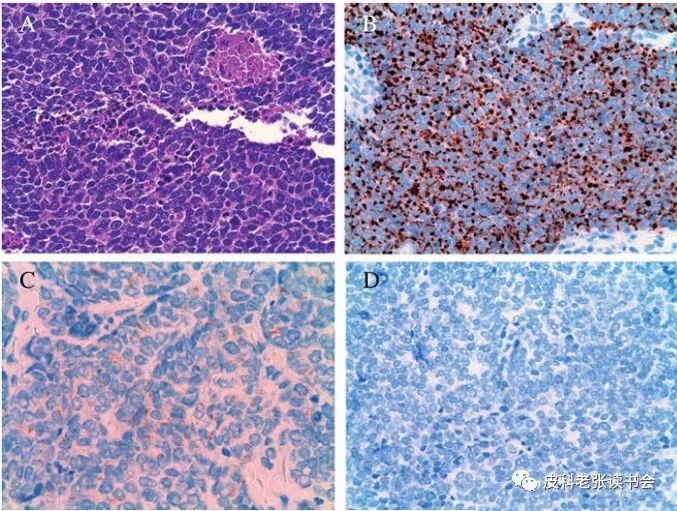
Figure 26 Histopathological and immunohistochemical manifestations of MCC
A. Undifferentiated tumor, scant cytoplasm, coarse chromatin, necrotic foci, and mitotic figures can be seen; B. CK20 positive, showing dense diffuse perinuclear expression; C. Chromogranin A staining shows diffuse positivity in the cytoplasm; D. TTF-1 staining is negative.
Figure 27 Immunohistochemical results of MCC at the sternum scar
A. Positive expression of CD56; B. High expression of Ki67; C. Focal positivity of chromogranin A; D. Perinuclear CK20 positive expression.
Imaging Examination
Skin Ultrasound
A solid mass at the dermal-subcutaneous level shows a mixed echo pattern, primarily composed of hypoechoic bands; low echo lines resembling “smoke columns” can be seen. In patients with local recurrence, hyperechoic areas may be present, possibly due to postoperative scar tissue formation. Another significant feature in most cases is posterior acoustic enhancement, particularly evident in satellite foci. Color Doppler imaging shows strong vascularization within the tumor, including satellite foci, but vascularization is not as pronounced in patients with local skin recurrence (Figure 28[32]).
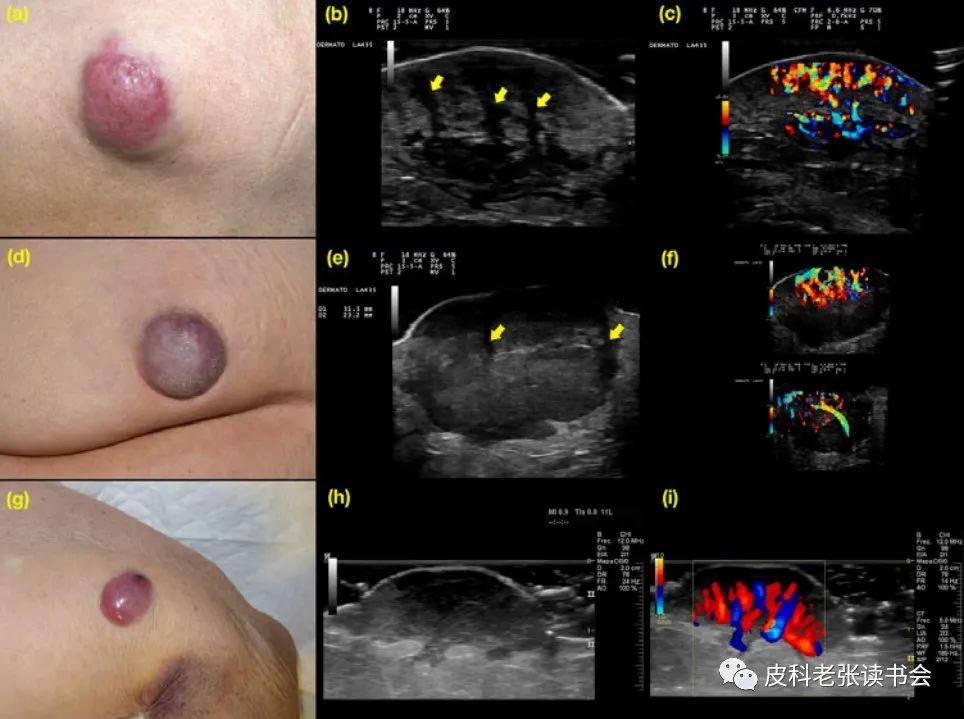
Figure 28 Ultrasound features of MCC
a-c: a. Primary tumor in the left thigh; b. Ultrasound shows a mixed echo skin-subcutaneous mass with linear hypoechoic bands (arrow); c. Color Doppler shows strong vascular formation within the tumor; d-f: d. Primary tumor in the buttock; e. Ultrasound shows a mixed echo skin-subcutaneous mass with linear hypoechoic bands (arrow), infiltrating borders; f. Color Doppler shows dense vascularization within the tumor; g-i: g. Primary tumor in the left arm; h. Ultrasound shows dermal-subcutaneous mass, with thickened epidermis, showing finger-like projections; i. Color Doppler shows strong vascularization of the tumor.
CT/MRI
Used to determine the nature of the lesions, screen for lymph node and distant metastases, assess treatment effects, and for follow-up monitoring (Figures 29[33], 30[34]).
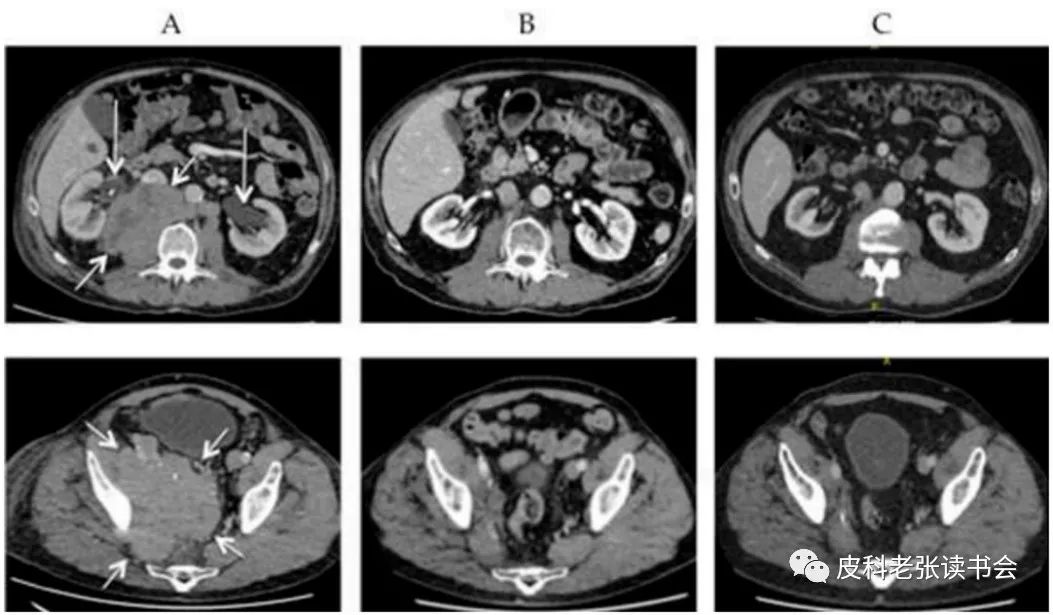
Figure 29 CT images before and after treatment in a 66-year-old male MCC patient
Numerous lymph node metastases in the abdomen and pelvis (short arrow), still progressing during treatment with avelumab, followed by combined radiotherapy. A. Before radiotherapy, bilateral hydronephrosis (long arrow); B. Two months after radiotherapy, hydronephrosis completely resolved; C. Two years after radiotherapy, kidneys remain in normal condition.
Figure 30 A 72-year-old male with a painless enlarging mass on the right foot
A. The tumor (arrow) shows moderate signal intensity on the coronal T1-weighted image, similar to muscle; B. On the sagittal T2-weighted image, it shows uniform moderate to slightly high signal intensity, slightly higher than muscle; C. After injection of gadolinium contrast agent, the lesion shows gadolinium enhancement.
PET-CT
Although CT/MRI are useful, most institutions use PET-CT to identify and quantify lymph node or distant metastases (Figure 31[35]). A systematic review and meta-analysis of 10 imaging studies showed that PET-CT has a sensitivity of 90% and specificity of 98%[15]. Multiple studies suggest that PET-CT may be the preferred method for routine staging of MCC.
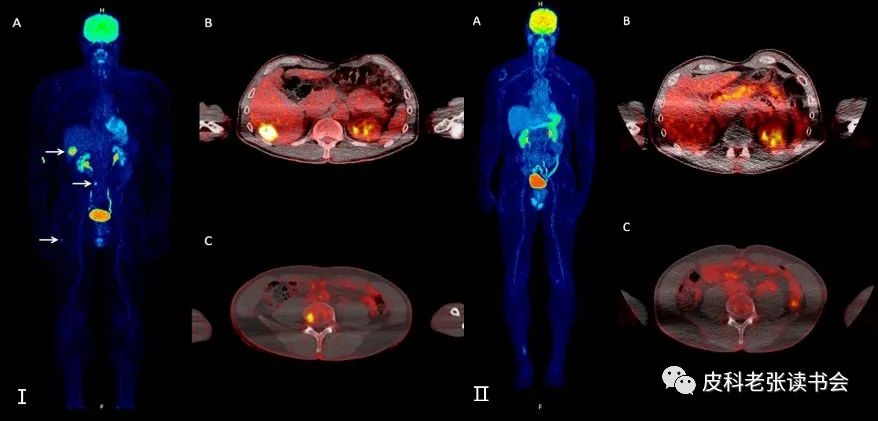
Figure 31 60-year-old MCC patient with liver metastasis
I: (A) Whole-body 18F-FDG PET shows increased tracer uptake in the liver, lumbar vertebrae, and right femur, corresponding to metastatic tumors (arrow); transverse fusion 18F-FDG PET/CT (B) shows increased tracer uptake in the liver segment VI, corresponding to liver metastasis; (C) Pathological tracer accumulation in the fourth lumbar vertebra, corresponding to bone metastasis; II: Follow-up results after 1 year of treatment with Avelumab show complete metabolic response of previously observed metastatic tumors in both whole-body (A) and fused 18F-FDG PET/CT images (B, C).
Diagnosis
The diagnosis of MCC relies on a comprehensive assessment of multiple factors including medical history, clinical manifestations, histopathology, immunohistochemistry, molecular markers, and imaging.
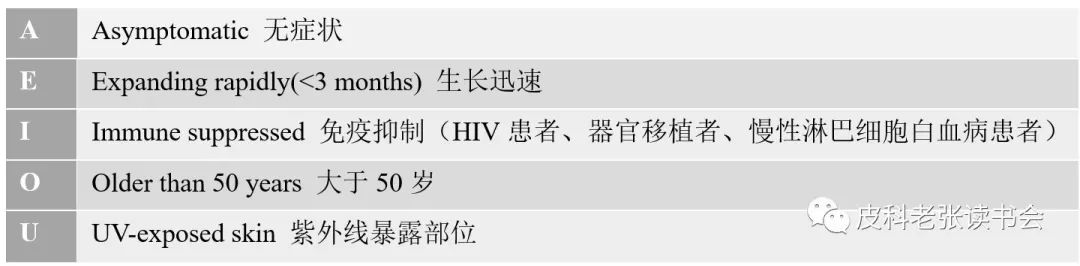
In 2008, Heath et al.[6] summarized 195 cases and proposed the clinical features of “AEIOU” for preliminary diagnosis of MCC (Table 2); among patients with primary skin MCC, 89% exhibited three or more features.
Table 2 AEIOU clinical features of MCC
Staging
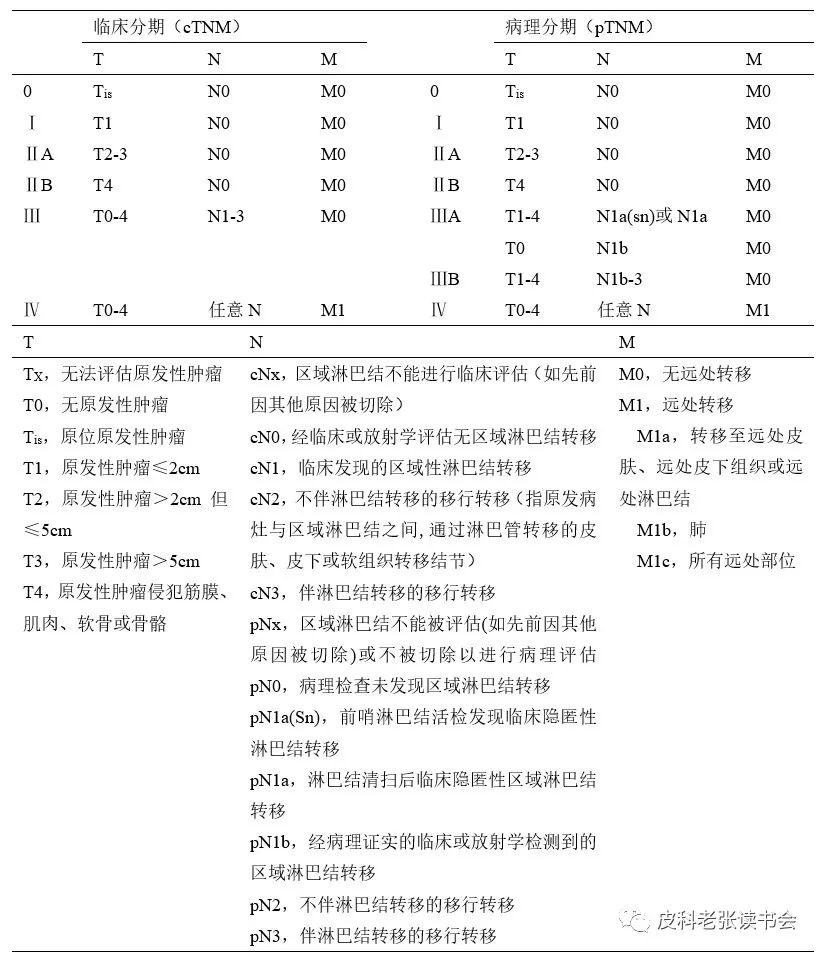
The staging of tumors is crucial for treatment options and prognosis assessment. Before 2010, due to the rarity of MCC and the limited number of diagnosed cases, there was a lack of consensus on its staging and prognosis. In 2010, the American Joint Committee on Cancer (AJCC) first developed a consensus staging/prognostic system for MCC based on an analysis of 5823 cases from the National Cancer Database (NCDB). In 2017, an analysis of 9387 MCC patients diagnosed from 1998 to 2012 led to a revision of the AJCC staging system, now in its 8th edition. The updated system separates clinical and pathological staging, allowing for more accurate staging and prognosis assessment for MCC patients (Table 3[8]).
Table 3 8th edition AJCC revised TNM staging criteria for MCC
Differential Diagnosis
MCC needs to be differentiated from various benign or malignant tumors due to its skin lesions and histopathology being similar to other diseases (Table 4[9]), with the final diagnosis primarily based on histopathological and immunohistochemical characteristics (Table 5[12,36]).
Table 4 Differential diagnosis of MCC
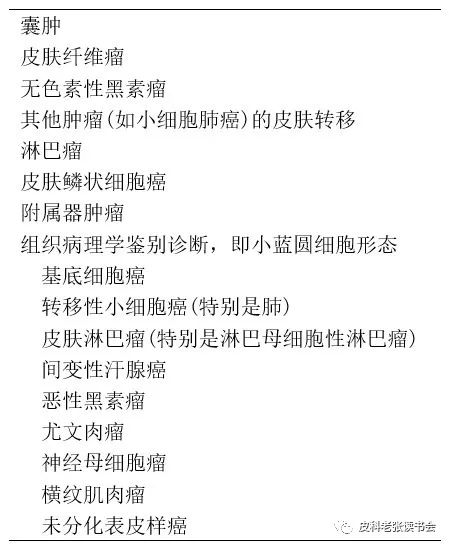
Table 5 Immunohistochemical markers for MCC and common differential diagnoses

Treatment
The rarity of MCC makes prospective studies on its treatment challenging. Until 2009, the National Comprehensive Cancer Network (NCCN) published treatment guidelines. The latest NCCN guidelines recommend treatment plans based on the patient’s presentation of primary tumors, lymph node involvement, and distant metastases, including surgical treatment, radiation therapy, chemotherapy, and immunotherapy[15]. A simplified treatment flowchart is shown in Figure 32[9].
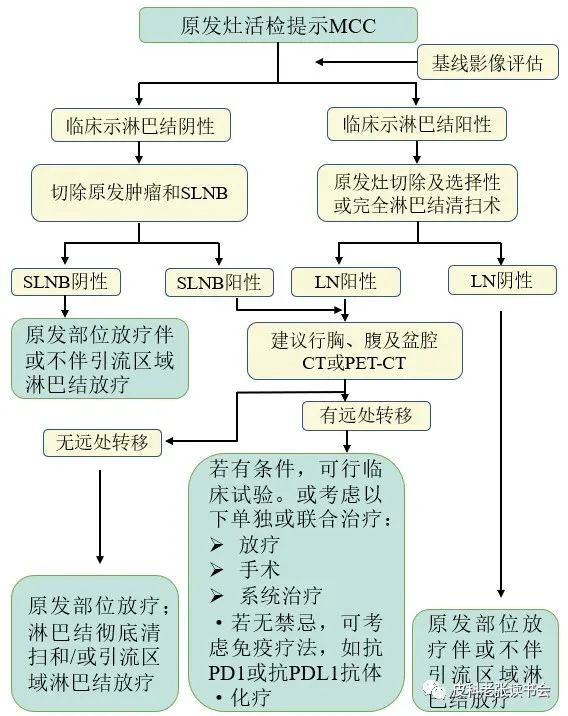
Figure 32 Simplified assessment and treatment of primary MCC
Surgical Treatment
Primary tumors can be considered for surgical excision, using Mohs micrographic surgery, modified Mohs micrographic surgery, etc., with margins of 1-2 cm up to fascia or periosteum. It is recommended to combine surgery with postoperative radiotherapy (Figure 33[37]).

Figure 33 Surgical treatment of hand MCC
I: A slightly raised, pale red lesion above the proximal phalanx of the left middle finger; II: Intraoperative photos show (a) complete excision of the lesion, with margins of 1-2 cm, (b) full-thickness skin graft to close the wound; III: Postoperative follow-up (a) at 2 months, early healing of the wound with small areas of epidermal detachment, (b) at 6 months, the wound healed well, with good finger function.
Radiation Therapy
① Extensive adjuvant radiation therapy to the site of the resected primary tumor (Figure 34[33]); ② Radiation therapy for draining lymph nodes; ③ Radiation therapy for primary lesions in patients unable to tolerate surgery.

Figure 34 A 94-year-old patient with MCC on the right side of the face receiving radiation therapy
A. A large red mass on the right side of the face before treatment; B. After 8 sessions of radiation therapy (32 Gy); C. After 12 sessions of radiation therapy (48 Gy); D. 6 weeks after the end of radiation therapy.
Chemotherapy
The chemotherapy regimen is based on small cell lung cancer protocols, with carboplatin/cisplatin and etoposide as first-line drugs; second-line treatments include various combinations of anthracyclines, cyclophosphamide, vincristine, bleomycin, and 5-fluorouracil. Although MCC is sensitive to chemotherapy, the effects are often not long-lasting.
Immunotherapy
In recent years, immunotherapy has significantly extended the survival of patients with metastatic MCC, with various potential therapeutic targets reported for tumor immunity (Figure 35[10]), particularly the application of PD-1 and PD-L1 pathway immunotherapy. These drugs are currently the standard first-line treatment for metastatic MCC. On March 23, 2017, the FDA approved Avelumab (Bavencio), a product of Merck/Pfizer, for the treatment of metastatic MCC. In addition, Pembrolizumab (Figure 36[38]) and Nivolumab (Figure 37[39]) have also been reported for the treatment of MCC.
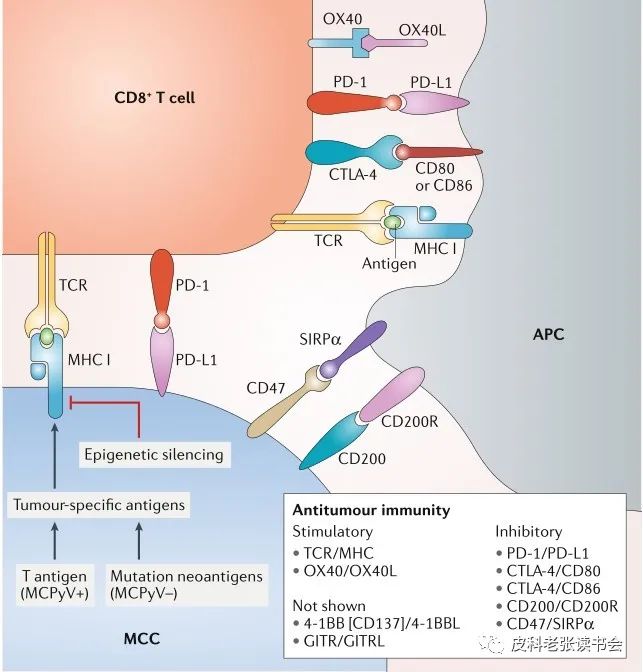
Figure 35 Signaling pathways and potential therapeutic targets for anti-MCC tumor immunity.
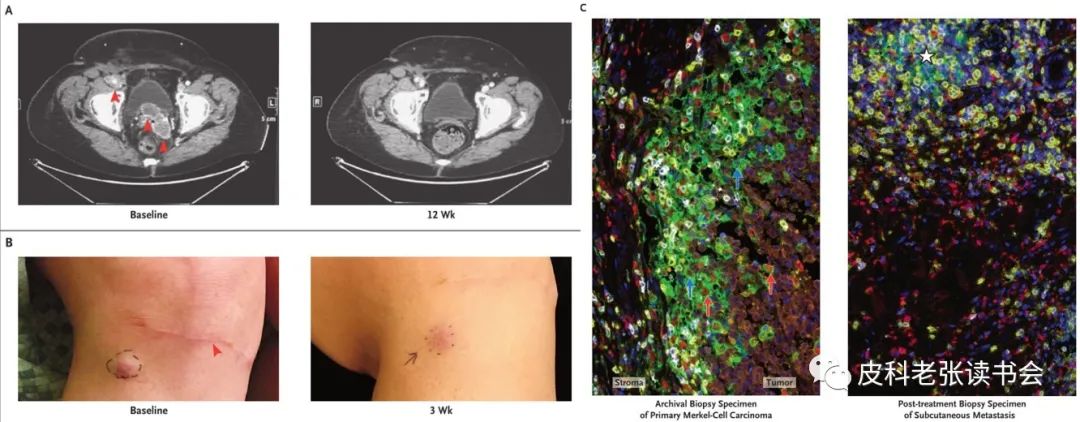
Figure 36 Response to Pembrolizumab treatment in a stage IV MCC patient
New peritoneal and lymph node metastases (A, red arrow) appeared after excision of the primary skin lesion and lymph node dissection, along with several subcutaneous metastatic foci located just below the site of the previously excised primary tumor (B; red arrow indicates the site of the previously excised primary tumor). During anti-PD-1 treatment, the metastatic foci rapidly regressed; C. Multispectral immunohistochemical results of the primary tumor (left) and adjacent post-treatment subcutaneous metastatic tumor (right): the pathological biopsy specimen shows immune infiltration most intense at the tumor-stroma interface, and the post-treatment biopsy specimen shows diffuse immune phagocyte infiltration with no evidence of residual tumor (orange indicates MCC expressing NSE, yellow indicates CD8+ T cells, red indicates CD68+ macrophages, white indicates PD-1, green indicates PD-L1, blue indicates DAPI nuclear staining).
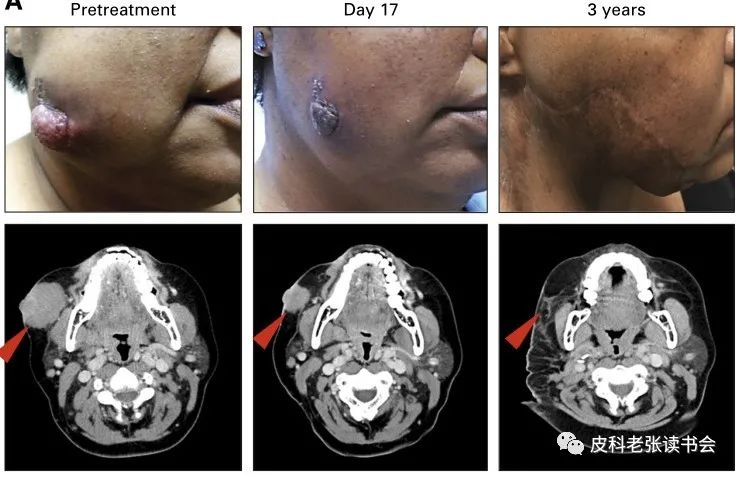
Figure 37 53-year-old female, advanced primary MCC on the face, T3N0
Received two doses of Nivolumab treatment before surgery, with both physical examination and CT scan showing rapid tumor regression on day 17; on day 20, the patient underwent surgery (radical facial resection, parotid gland resection, and neck lymph node dissection); no recurrence of the tumor during 3.5 years of follow-up.
Monitoring and Follow-Up
Since MCC most commonly recurs within the first two years after diagnosis, NCCN guidelines recommend close monitoring every 3-6 months for the first two years, with comprehensive skin and lymph node examinations, followed by monitoring every 6-12 months thereafter. For high-risk patients for recurrence and metastasis, PET-CT is the preferred examination method, and CT and MRI may also be considered.
40.5% of patients with active MCC can detect antibodies against MCPyV tumor-associated antigens, while only 0.9% in the normal population. For patients with high antibody titers, successful treatment correlates with a rapid decline in titers, while recurrence correlates with a rapid rise in titers; seropositivity at diagnosis is also associated with a reduced risk of recurrence. Therefore, the NCCN guidelines recommend detecting baseline MCPyV cancer protein antibodies as indicators for assessing efficacy and prognosis[15].
The content of this article is for academic discussion only and is intended for medical professionals.
Participants:
Sun Liting, Fu Deshuang, Zhang Hanyin, Mao Yu, Hu Yuan, Sun Yuzhen, He Jiangman, Xin Wuyan, Yuan Mengjin, Yang Xiaoxiao, Zhang Yang, Shi Weihua, Wei Xuhua, Zhao Bingjie, Zhang Jiang’an
References:


[1] Harms PW. Update on Merkel Cell Carcinoma. Clin Lab Med. 2017;37(3):485-501.
[2] Halata Z, Grim M, Bauman KI. Friedrich Sigmund Merkel and his “Merkel cell”, morphology, development, and physiology: review and new results. Anat Rec A Discov Mol Cell Evol Biol. 2003;271(1):225-239.
[3] Toker C. Trabecular carcinoma of the skin. Arch Dermatol. 1972 Jan;105(1):107-110.
[4] Tang CK, Toker C. Trabecular carcinoma of the skin: an ultrastructural study. Cancer. 1978;42(5):2311-2321.
[5] Feng H, Shuda M, Chang Y, et al. Clonal integration of a polyomavirus in human Merkel cell carcinoma. Science. 2008;319(5866):1096-1100.
[6] Heath M, Jaimes N, Lemos B, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008;58(3):375-381.
[7] Lemos BD, Storer BE, Iyer JG, et al. Pathologic nodal evaluation improves prognostic accuracy in Merkel cell carcinoma: analysis of 5823 cases as the basis of the first consensus staging system. J Am Acad Dermatol. 2010;63(5):751-761.
[8] Harms KL, Healy MA, Nghiem P, et al. Analysis of prognostic factors from 9387 Merkel cell carcinoma cases forms the basis for the new 8th edition AJCC staging system. Ann Surg Oncol. 2016;23(11):3564-3571.
[9] Becker JC, Stang A, DeCaprio JA, et al. Merkel cell carcinoma. Nat Rev Dis Primers. 2017;3:17077.
[10] Harms PW, Harms KL, Moore PS, et al. The biology and treatment of Merkel cell carcinoma: current understanding and research priorities. Nat Rev Clin Oncol. 2018;15(12):763-776.
[11] Chang Y, Moore PS. Merkel cell carcinoma: a virus-induced human cancer. Annu Rev Pathol. 2012;7:123-144.
[12] Prieto Muñoz I, Pardo Masferrer J, Olivera Vegas J, Fortes Alen JR, Pérez Casas AM. Merkel cell carcinoma: what do we know about it and what should we do? Clin Transl Oncol. 2012;14(6):401-412.
[13] Lipner SR. Merkel cell carcinoma in a patient with CLL/Atypical AML. J Cutan Med Surg. 2018;22(3):324.
[14] Koljonen V, Sahi H, Böhling T, Mäkisalo H. Post-transplant Merkel cell carcinoma. Acta Derm Venereol. 2016;96(4):442-447.
[15] Xue Y, Thakuria M. Merkel cell carcinoma review. Hematol Oncol Clin North Am. 2019;33(1):39-52.
[16] Vangipuram R, Haley C, Tyring SK. A woman with a large ulcerated nodule on the finger. JAMA. 2018;319(1):78-79.
[17] Garcia-Carbonero R, Marquez-Rodas I, de la Cruz-Merino L, et al. Recent therapeutic advances and change in treatment paradigm of patients with Merkel cell carcinoma. Oncologist. 2019;24(10):1375-1383.
[18] Grippaudo FR, Costantino B, Santanelli F. Merkel cell carcinoma on a sternotomy scar: atypical clinical presentation. J Clin Oncol. 2015;33(5):e22-24.
[19] Yom SS, Rosenthal DI, El-Naggar AK, Kies MS, Hessel AC. Merkel cell carcinoma of the tongue and head and neck oral mucosal sites. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(6):761-768.
[20] Gomez-Arias PJ, Salido-Vallejo R. Merkel-Cell Carcinoma. N Engl J Med. 2019;381(23):e40.
[21] Bassi A, Arunachalam M, Galeone M, et al. Multiple clustered nodules on the leg. Diagnosis: Merkel cell carcinoma. J Clin Oncol. 2014;32(17):e61-e62.
[22] Fujimoto N, Nakanishi G, Kabuto M, et al. Merkel cell carcinoma showing regression after biopsy: Evaluation of programmed cell death 1-positive cells. J Dermatol. 2015;42(5):496-499.
[23] Poulsen M. Merkel-cell carcinoma of the skin. Lancet Oncol. 2004;5(10):593-599.
[24] Nambudiri VE, Vivero M, Watson AJ, et al. Merkel cell carcinoma presenting as subcutaneous breast masses: an uncommon presentation of a rare neuroendocrine neoplasm. Breast J. 2016;22(1):113-115.
[25] Whitman EJ, Brassell SA, Rosner IL, Moncur JT. Merkel cell carcinoma as a solitary metastasis to the testis. J Clin Oncol. 2007;25(24):3785-3786.
[26] Jalilian C, Chamberlain AJ, Haskett M, et al. Clinical and dermoscopic characteristics of Merkel cell carcinoma. Br J Dermatol. 2013;169(2):294-297.
[27] Longo C, Benati E, Borsari S, et al. Merkel cell carcinoma: morphologic aspects on reflectance confocal microscopy. J Eur Acad Dermatol Venereol. 2017;31(11):e480-e481.
[28] Smith PD, Patterson JW. Merkel cell carcinoma (neuroendocrine carcinoma of the skin). Am J Clin Pathol. 2001;115 Suppl:S68-S78.
[29] Trinidad CM, Torres-Cabala CA, Prieto VG, Aung PP. Update on eighth edition American Joint Committee on cancer classification for Merkel cell carcinoma and histopathological parameters that determine prognosis. J Clin Pathol. 2019;72(5):337-340.
[30] Goessling W, McKee PH, Mayer RJ. Merkel cell carcinoma. J Clin Oncol. 2002;20(2):588-598.
[31] Khanna U, North JP. Large-cell variant of Merkel cell carcinoma with clear-cell change. J Cutan Pathol. 2020;47(1):1-5.
[32] Hernández-Aragüés I, Vázquez-Osorio I, Alfageme F, et al. Skin ultrasound features of Merkel cell carcinoma. J Eur Acad Dermatol Venereol. 2017;31(7):e315-e318.
[33] Zwijnenburg EM, Lubeek SFK, Werner JEM, et al. Merkel cell carcinoma: new trends. Cancers (Basel). 2021;13(7):1614.
[34] O’Rourke H, Meyers SP, Katzman PJ. Merkel cell carcinoma of the foot: case report and review of the literature. J Foot Ankle Surg. 2007;46(3):196-200.
[35] Sachpekidis C, Sidiropoulou P, Hassel JC, Drakoulis N, Dimitrakopoulou-Strauss A. Positron emission tomography in Merkel cell carcinoma. Cancers (Basel). 2020;12(10):2897.
[36] Naseri S, Steiniche T, Ladekarl M, et al. Management recommendations for Merkel cell carcinoma-a danish perspective. Cancers (Basel). 2020;12(3):554.
[37] Westerveld DR, Hall DJ, Richards WT. Merkel cell carcinoma of the hand: a case report and review of the literature. Hand (N Y). 2016;11(4):NP24-NP29
[38] Nghiem PT, Bhatia S, Lipson EJ, et al. PD-1 blockade with Pembrolizumab in advanced Merkel-cell carcinoma. N Engl J Med. 2016;374(26):2542-2552.
[39] Topalian SL, Bhatia S, Amin A, et al. Neoadjuvant Nivolumab for patients with resectable Merkel cell carcinoma in the CheckMate 358 trial. J Clin Oncol. 2020;38(22):2476-2487.

Scan the QR code
Follow us
Official Account| Dermatology Book Club