All small joints of the hand are hinge joints. The metacarpophalangeal joint (MCP) has a saddle structure, while the proximal interphalangeal joint (PIP) and distal interphalangeal joint (DIP) have a ball-and-socket shape (Figure 1).
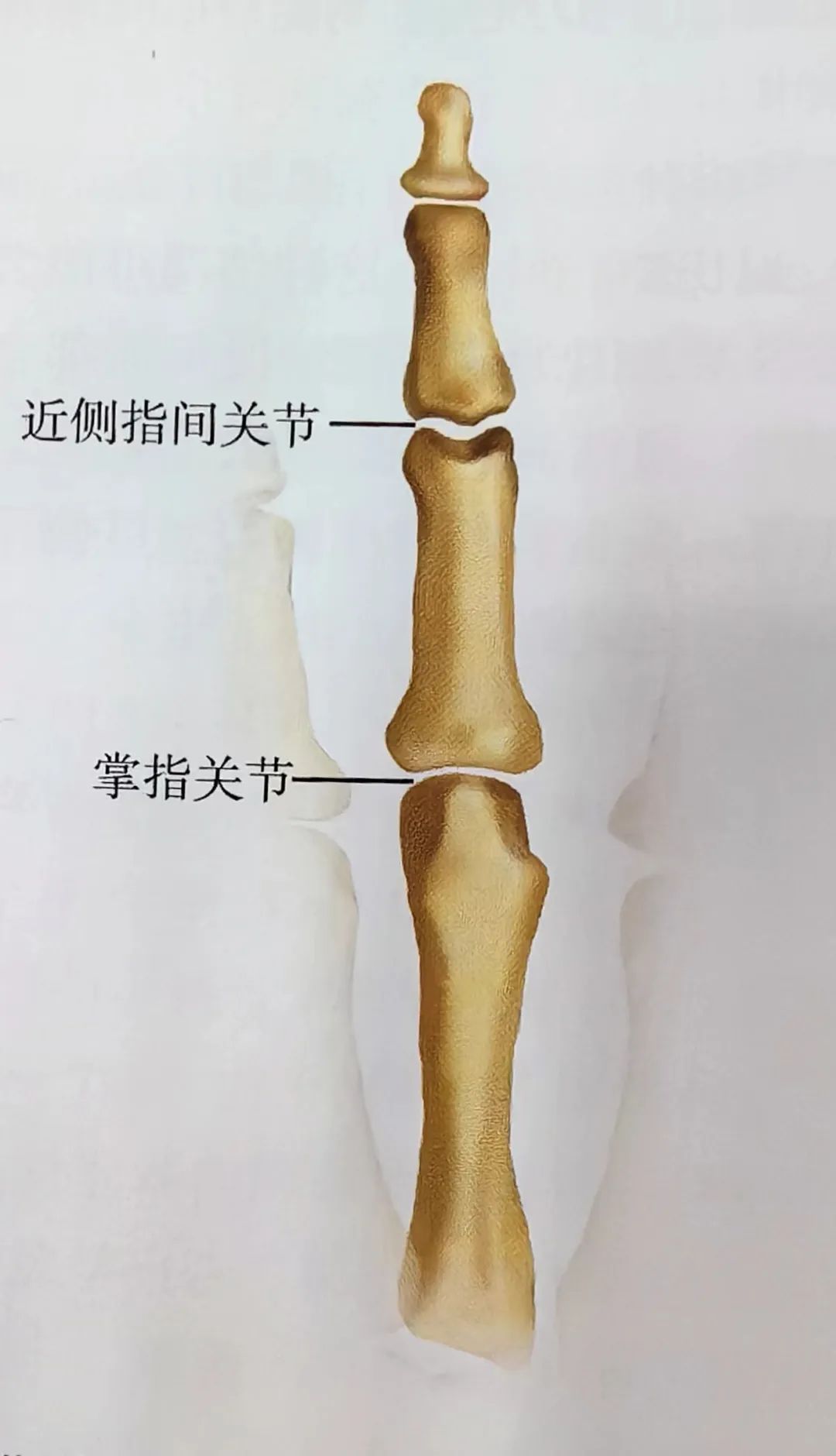
Figure 1: Structure of Hand Joints
The joints are surrounded by collateral ligaments, palmar plates, and tendons, which determine the stability of the joints. The palmar plate has strong attachments on the sides but is thin at the distal end (Figure 2).
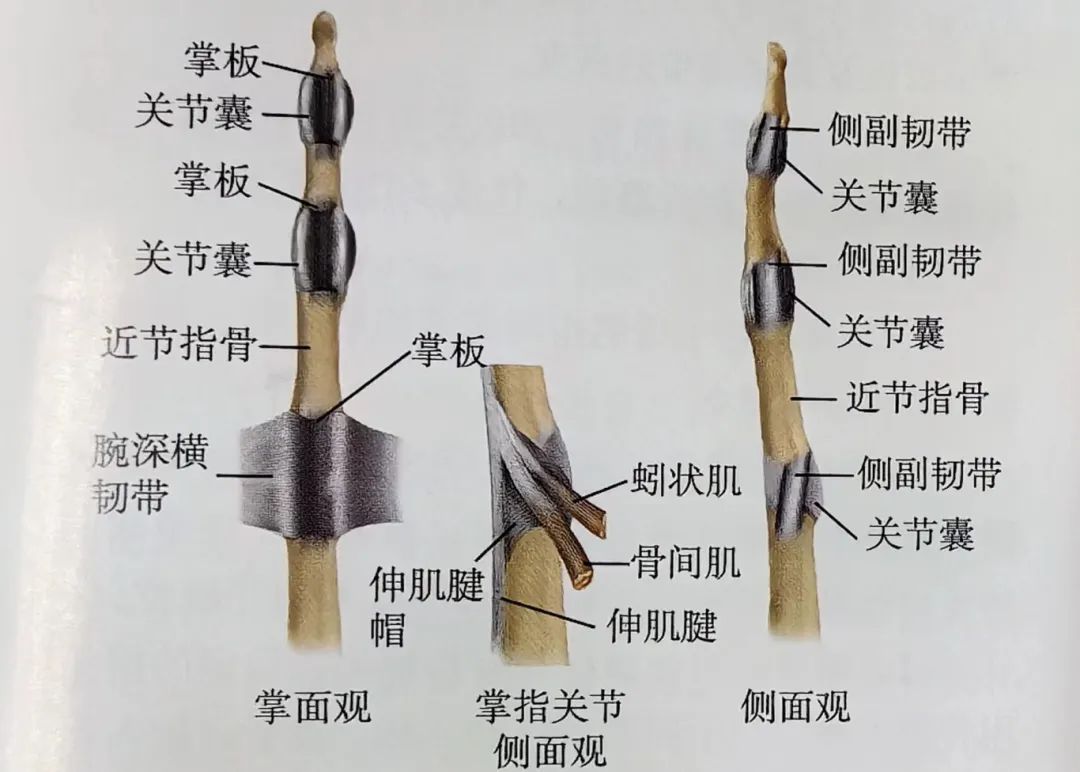
Figure 2: Structure of Interphalangeal Ligaments and Joint Capsules
Assessment of Hand Injuries
Visual and Palpation: Swelling, tenderness, and bruising of the fingers should raise high suspicion of joint injury.
Special Tests: Stress tests can reveal instability caused by potential fractures or ligament injuries, and comparative tests assist in diagnosis.
Kinematic Examination: Limited joint mobility may be caused by subluxation or displaced fracture fragments.
Imaging Examination: High-quality X-rays include anteroposterior (AP), lateral, and oblique views, with CT scans performed if necessary to determine the specifics of the injury.
Distal Interphalangeal Joint (DIP) Injuries
Sudden flexion force applied to the DIP joint can tear the extensor tendon from the distal phalanx, with or without fracture fragments, and may involve more than 30% of the articular surface, with a risk of subluxation of the distal phalanx towards the palmar side (Figure 3).
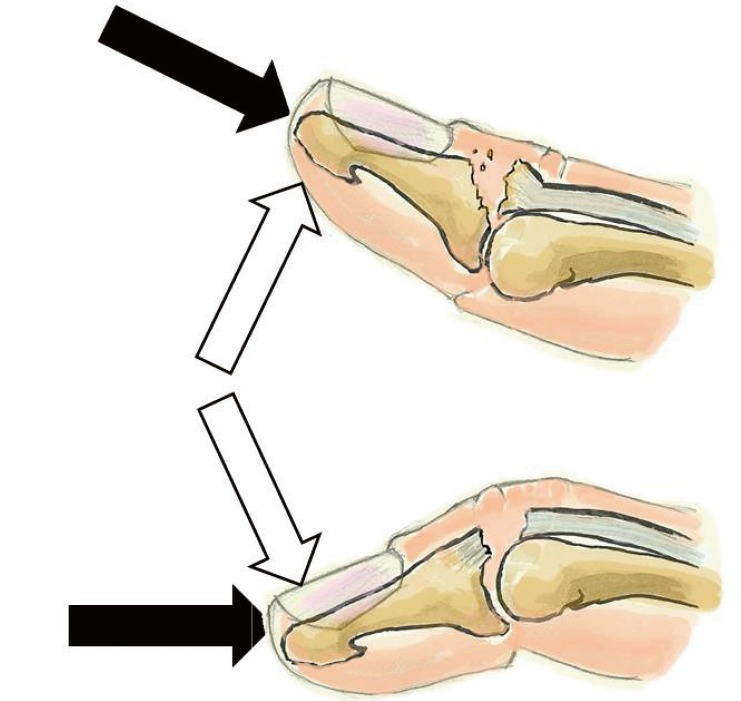
Figure 3: Mechanism of Injury
Pain, swelling, and drooping of the distal interphalangeal joint can be observed (Figure 4); X-rays may show flexion deformity of the DIP joint, with possible fracture fragments attached to the extensor tendon insertion, accompanied by palmar subluxation or fracture of the distal phalanx.
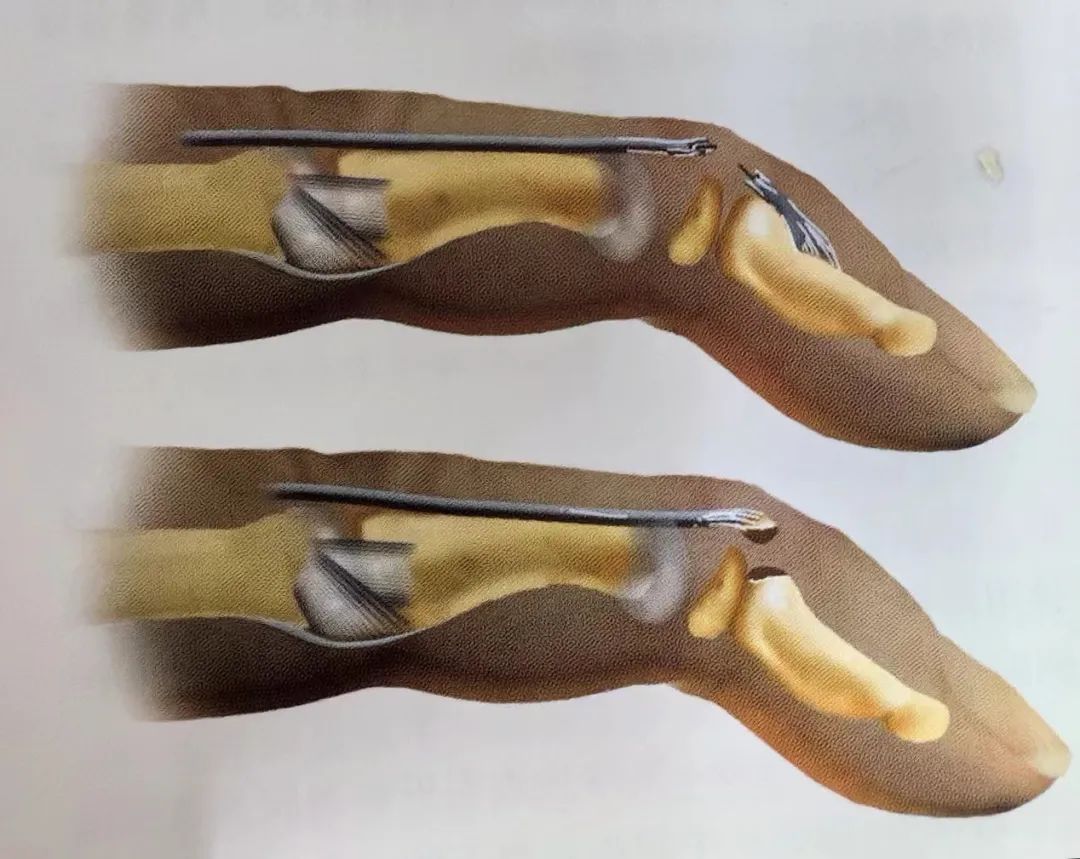
Figure 4: Mallet Finger Diagram
(2) Classification (Tubiana Classification) (Figure 5)
• Type I: Closed injury or blunt injury, continuity injury of the tendon, with or without small fracture fragments.
• Type II: Involves tearing at the plane of the DIP joint or its proximal side, continuity injury of the tendon.
• Type III: Involves deep wear, with skin, subcutaneous tissue, and tendon tissue defects.
• Type IV: Involves phalangeal fractures in children, with excessive flexion injuries involving 20-50% of the articular surface fractures, and hyperextension injuries involving fractures of more than 50% of the articular surface, with distal phalanx subluxation towards the palmar side.
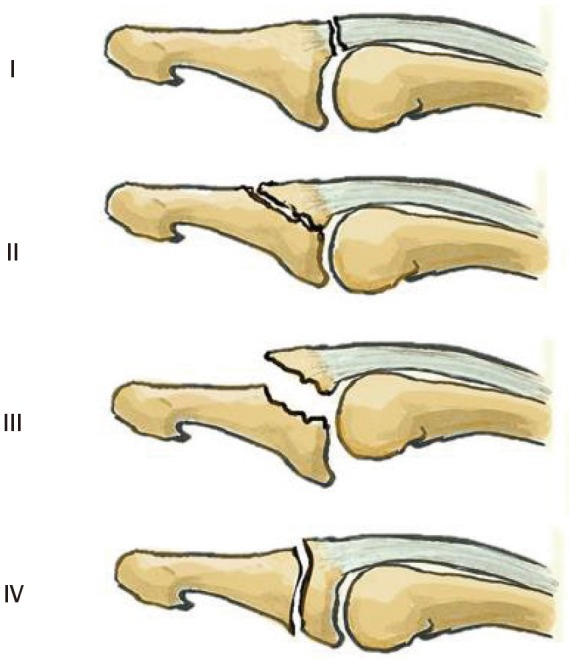
Figure 5: Tubiana Classification
Indicated for small fracture fragments involving less than 30% of the articular surface or displacement ≥2mm, using splints or casts for fixation. Maintain full extension for 6 weeks, with nighttime fixation for 4 weeks (Figure 6).
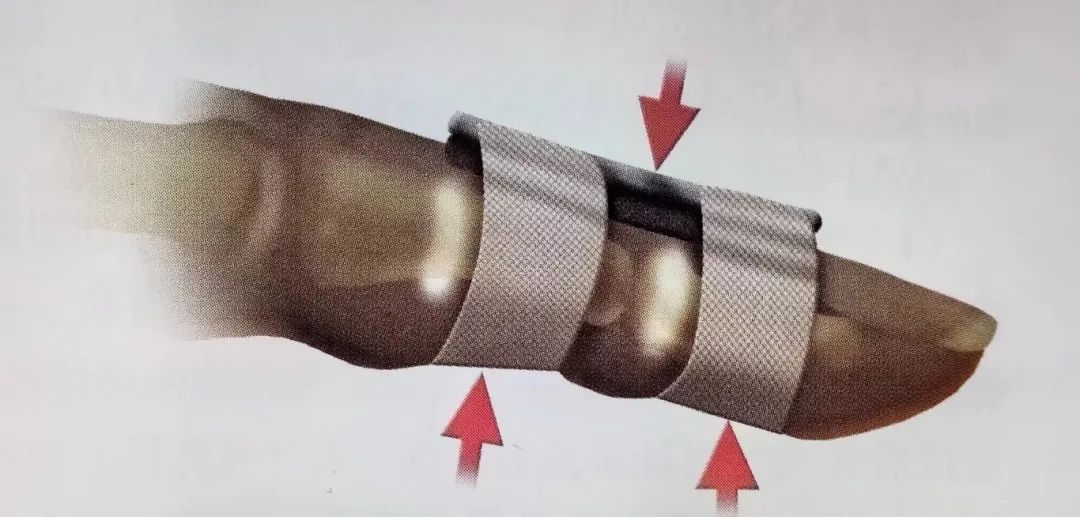
Figure 6: Splint Fixation of the Distal Interphalangeal Joint. Filling between the dorsal of the finger and the splint using a three-point fixation principle.
Mallet finger deformity with fracture fragments involving more than 30% of the articular surface, displacement >2mm, or associated with palmar subluxation of the distal phalanx is treated surgically. Open reduction and internal fixation (ORIF) is performed to correct the palmar subluxation of the DIP joint, using longitudinal Kirschner wires to fix the distal interphalangeal joint in the extended position, with tendon repair performed using button techniques or suture anchors, depending on the patient’s injury condition, to determine if tendon repair is necessary (Figures 7, 8).

Figure 7: Surgical Procedure Diagram
Figure 8: Comparison of Surgical Treatment
Common complications include permanent mallet finger deformity, secondary boutonniere deformity, and traumatic arthritis due to joint mismatch or palmar subluxation (Figure 9).
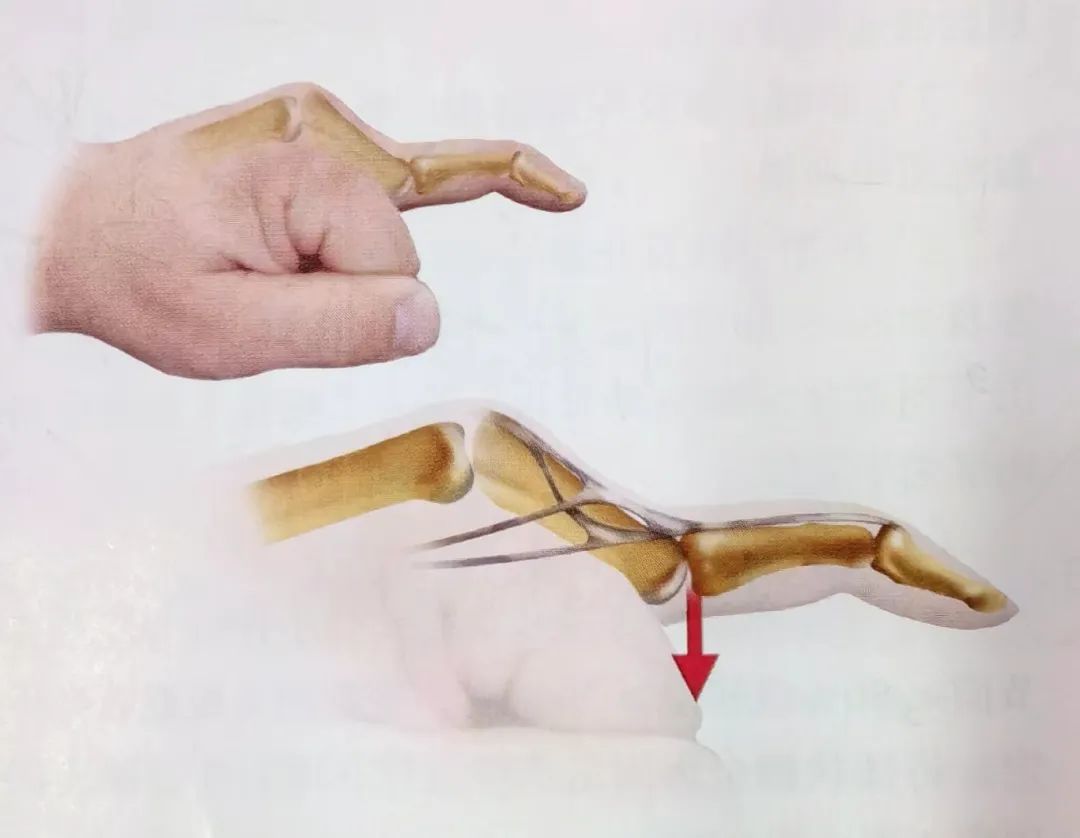
Figure 9: Secondary Boutonniere Deformity
• Dorsal Subluxation of the Distal Interphalangeal Joint
Hyperextension force applied to the interphalangeal joint leads to rupture of the palmar and collateral ligaments, while the deep tendons remain intact. Due to the skin being firmly tethered to the underlying bone, these injuries often accompany tears of the palmar soft tissue.
Tenderness and deformity are present, with inability to flex or extend the joint; X-rays in anteroposterior and lateral views determine if there are associated avulsion fractures (Figure 10).

Figure 10: X-ray of Dorsal Subluxation of the Distal Interphalangeal Joint
Closed dislocation, open dislocation, fracture-dislocation.
Performed under digital nerve block, traction of the distal phalanx is followed by pushing the proximal phalanx back into place. After reduction, X-rays are evaluated for stability and any associated fractures, with short-term fixation for 10-14 days.
Entrapment of the palmar plate, deep flexor tendon, and displaced osteochondral fragments leads to irreducible dorsal dislocation of the distal interphalangeal joint, requiring open reduction to remove the fracture fragments, repair of the damaged collateral ligaments, and postoperative fixation for 3 weeks (Figure 11).
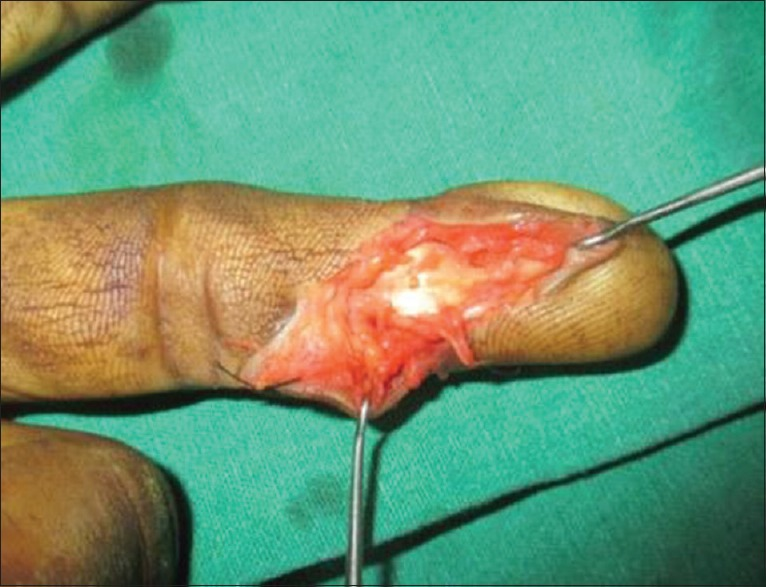
Figure 11: Intraoperative Reduction Diagram
Post-traumatic stiffness, recurrent instability, traumatic arthritis, and infection (purulent arthritis and osteomyelitis).
• Lateral Collateral Ligament Sprain of the Proximal Interphalangeal Joint
Abduction or adduction forces applied to a straight finger can cause tearing of the lateral collateral ligaments of the PIP joint, with radial side injuries being more common than ulnar side injuries.
Palpation reveals a significant tenderness point at the injured site, commonly at the proximal phalanx plane; stress tests are performed with the joint extended or flexed at 20°, lacking a strong endpoint; X-rays show an angle >20°, with small fracture fragments visible.
Static splinting for 7-14 days, followed by tape fixation to the adjacent finger for 3 weeks, encouraging active movement from day one. Deep scar tissue formation may cause joint instability and thickening of the collateral ligaments, lasting 3-6 months.
Indicated for imaging evidence of soft tissue entrapment, displaced condylar fractures, and persistent instability after 3 weeks of static splinting, where surgery on the radial collateral ligament of the index finger is often necessary.
• Injury to the Palmar Plate of the PIP Joint
Overextension injuries may cause tearing of the palmar plate from the middle phalanx, with or without fracture fragments.
Swelling at the proximal interphalangeal joint, with significant tenderness over the palmar plate; lateral X-rays may show small avulsion fracture fragments, typically at 10% of the small articular surface (Figure 12).

Figure 12: Injury to the Palmar Plate of the PIP Joint
Stable injuries are fixed with a dorsal splint in a flexed position of 20° for 1 week, followed by active movement with tape protection.
Post-traumatic flexion contracture, pain, and limited range of motion, with later development of boutonniere deformity.
• Dorsal Dislocation of the PIP Joint
Overextension of the PIP joint causes backward displacement of the finger, leading to dorsal dislocation of the middle phalanx, involving the proximal phalanx and tearing of the palmar plate.
The finger shows significant deformity, with instability confirmed by overextension stress tests; simple dorsal dislocation may indicate stability of the collateral ligaments; X-rays show dorsal dislocation of the proximal interphalangeal joint, distinguishing the distal position of the palmar plate (Figures 13, 14).
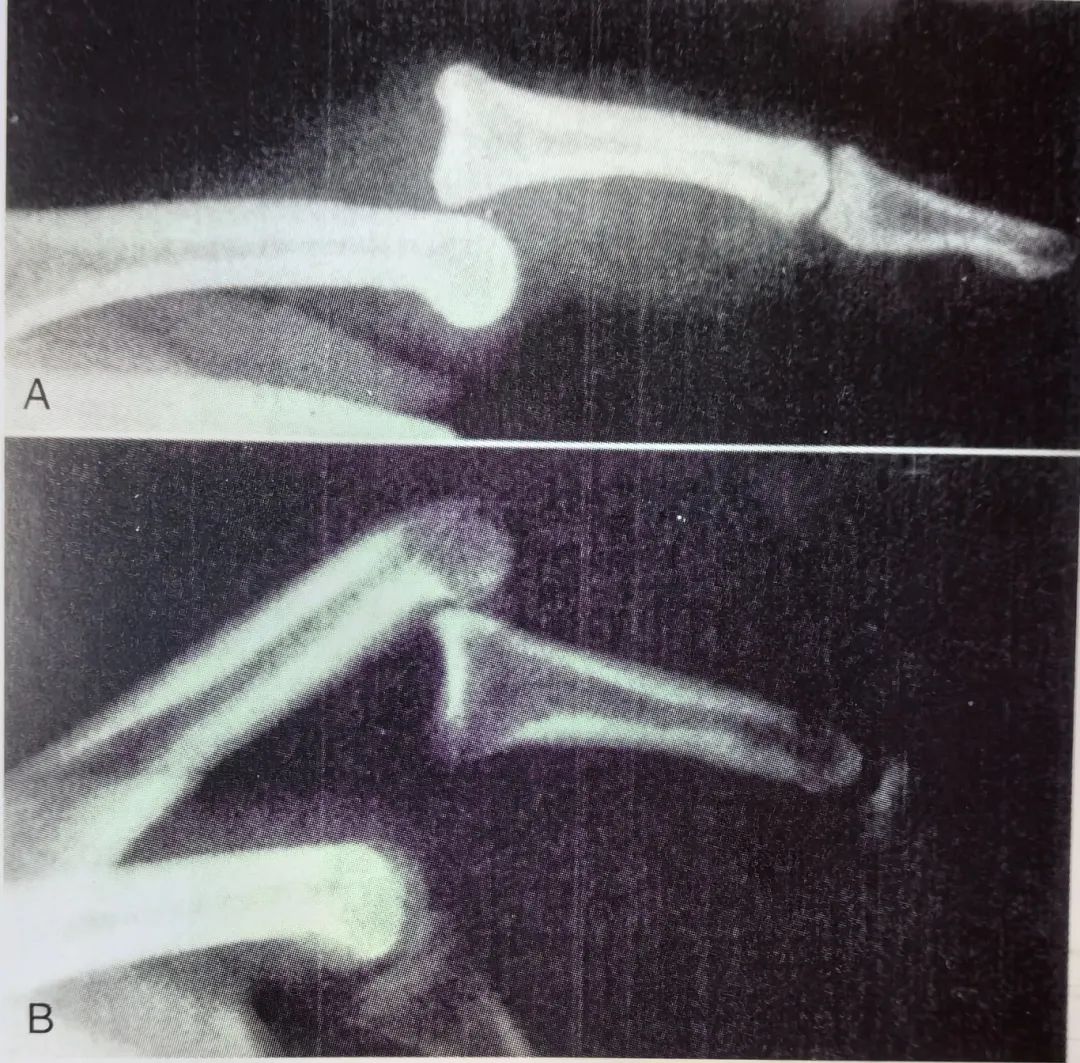
Figure 13: X-ray of Proximal Interphalangeal Joint Dislocation. A. Dorsal dislocation (most common); B. Palmar dislocation (rare)
Figure 14: Diagram of Proximal Interphalangeal Joint Dislocation
Under digital nerve block, longitudinal traction is used for closed reduction, with tape protection allowing early flexion movements for 3-6 weeks. For less stable injuries, splint fixation should be extended for 3 weeks to prevent the last 20° of extension.
Indicated for palmar fracture fragments involving more than 15% of the palmar joint surface, open dislocation, or rotational deformity of the finger.
Post-traumatic flexion contracture, stiffness of the PIP or DIP joints, and progressive boutonniere deformity (Figure 15).
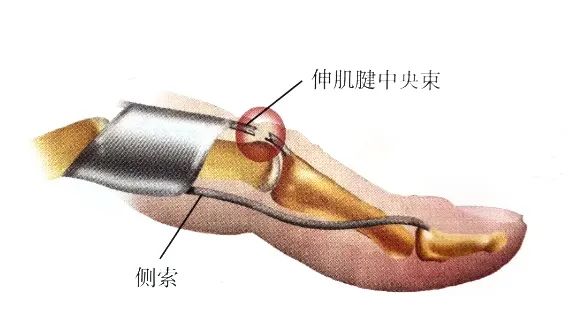
Figure 15: Complications after Lack of Treatment
• Fracture-Dislocation of the PIP Joint
Joint injuries due to overextension, compression, or shear forces may lead to pilon fracture-dislocation, which is the most disabling joint injury.
Swelling, pain, and limited mobility can be seen, often without significant deformity, easily misdiagnosed as a sprain; lateral X-rays may show intra-articular fracture fragments, with the fracture fragments occupying up to 50% of the joint surface, and the flexed position of the proximal interphalangeal joint helps diagnose dislocation (Figure 16).

Figure 16: X-ray of PIP Joint Fracture-Dislocation
• Closed Reduction Treatment
Indicated for stable flexion of the PIP joint and fracture fragments occupying <30% of the joint surface, using dorsal extension splinting, allowing voluntary flexion, with gradual extension activities after 4 weeks.
Open reduction and internal fixation: Indicated for large fracture fragments involving more than 50% of the joint surface, using wires, Kirschner wires, or compression screws for fixation.
Palmar plate reconstruction: Indicated for comminuted fractures, removing palmar fracture fragments, and advancing the palmar plate to the middle phalanx to regain stability and reshape the joint surface.
Bone traction: Indicated for severely comminuted fractures, with continuous longitudinal traction until fracture remodeling occurs.
Recurrent dislocation, limited joint mobility, and post-traumatic arthritis.
• Ulnar Collateral Ligament Injury of the Thumb MCP Joint
Tenderness and swelling on the ulnar side of the MCP joint may suggest Stener lesion; stress testing of the ulnar collateral ligament and comparative tests determine if the ligament is completely torn and associated with joint instability; X-rays assess for associated fractures, with stress X-rays showing an opening of the MCP joint >35° indicating complete ligament rupture (Figure 13)..

Figure 13: Stress X-ray
Indicated for partial tears of the ulnar collateral ligament, with intact endpoints, and stress tests showing <35° opening; casts or functional braces should be fixed at a slight flexion position of the MCP joint for 3-4 weeks.
Indicated for complete tears of the ulnar collateral ligament associated with MCP joint instability or displaced fracture fragments, reconstruction is achieved through suture anchors or pull-out wires.
Residual instability with pain, weakness of pinch strength, palmar subluxation of the MCP joint, and late-stage arthritis.
• Radial Collateral Ligament Injury of the Thumb MCP Joint
Less common, often missed, potentially leading to delayed treatment.
Swelling and tenderness on the radial side of the thumb MCP joint, with stress tests eliciting pain or confirming radial opening of the joint, often accompanied by palmar subluxation; X-rays may show small osteochondral fragments of the metacarpal.
Almost all can be treated with tubular casts or thumb spica splints for 4-6 weeks, with tubular casts needing to prevent palmar subluxation of the MCP joint.
Indicated for MCP joint instability or palmar subluxation, with surgical repair through suture anchors or pull-out wires.
• Lateral Collateral Ligament Injury of the Finger MCP Joint
Resulting from trauma to the finger, causing injury to the radial or ulnar collateral ligaments of the metacarpophalangeal joint, often with avulsion fractures at the attachment of the proximal phalanx, sometimes including avulsion fragments.
Slight swelling between the metacarpal heads, local tenderness positive, gentle stress tests of the metacarpophalangeal joint may elicit pain or show instability; X-rays show avulsion fragments from the metacarpal heads.
Most finger collateral ligament injuries can be managed non-surgically, using finger tape to protect the collateral ligaments of the MCP joint, with splinting at a flexed position of 50° for unstable injuries, expecting relief of symptoms after more than 3 months.
Indicated for avulsion fractures involving 20% of the articular surface or displacement >2mm, particularly for radial collateral ligament injuries of the index or little finger.
Joint instability, laxity, weakness or pain, with secondary adhesions.
• Dorsal Dislocation of the MCP Joint
Commonly occurs in the index, thumb, and little finger, dorsal dislocation is the most frequent dislocation, which can be very complex or very simple.
The metacarpophalangeal joint is in a hyperextended position with obvious deformity; X-rays show the proximal interphalangeal joint in a hyperextended position of 60-90°; complex dislocations may not be apparent, with slight hyperextension and a depression in the palm skin, with X-rays showing the proximal phalanx and metacarpal aligned parallel (Figure 14).

Figure 14: Complex Dorsal Dislocation of the MCP Joint. A. Diagram; B. Clinical Photo; C. X-ray
Perform gentle closed reduction, first hyperextending the MCP joint, then pushing the proximal phalanx forward past the metacarpal head, avoiding direct longitudinal traction.
Complex dislocations that fail closed reduction attempts require open reduction, by removing the entrapped palmar plate, avoiding nerve damage, and addressing fractures. Ensure stability after reduction, while performing flexion and extension exercises under tape protection.
Nerve injury, joint stiffness, and arthritis.


