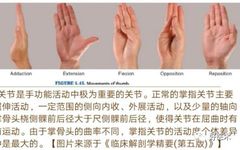
The metacarpophalangeal joint primarily performs flexion and extension, with a few individuals able to hyperextend. The degree of flexion varies significantly. The metacarpophalangeal joint often dislocates due to external forces caused by finger sprains, punctures, or extreme dorsal extension or flexion. Depending on the position of the finger during trauma and the direction of the external force, the metacarpophalangeal joint can experience dorsal or palmar dislocation, with dorsal dislocation being more common. Recently, during my training in the Trauma Orthopedics department of Weihai Municipal Hospital, I encountered two cases of thumb MCP joint dislocation (one palmar and one dorsal dislocation). Throughout the management of these cases, I gained deeper insights into the treatment of metacarpophalangeal joint dislocations. I would like to thank my mentors, Associate Chief Physician Xiao Hongqiang, Associate Chief Physician Chen Kang, attending physician Li Dawei, and other teachers in the Trauma Orthopedics department for their guidance and support during my orthopedic training. This article aims to present relevant knowledge on thumb metacarpophalangeal joint dislocation through the collection and organization of related literature, hoping to enhance understanding of metacarpophalangeal joint dislocations, especially those of the thumb, and to facilitate clinical management of such conditions.
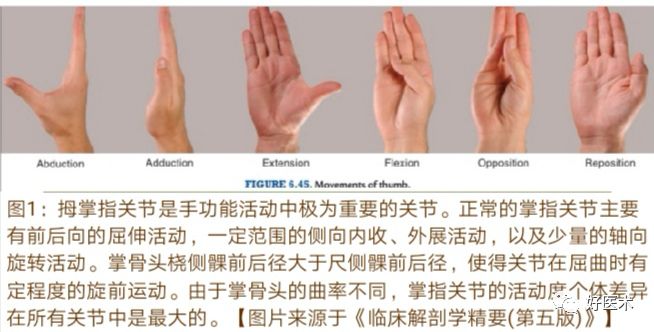
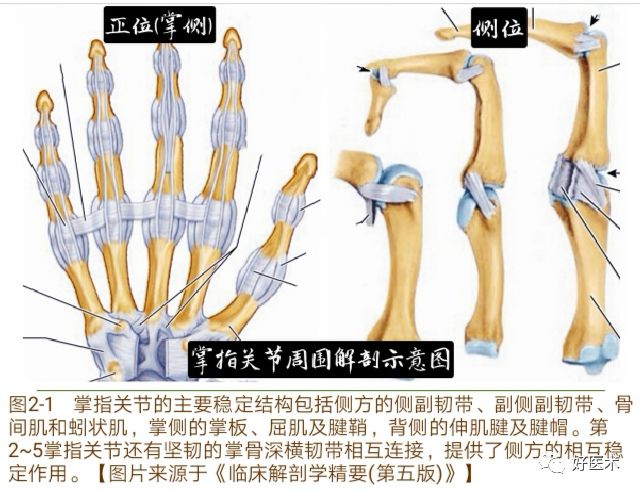
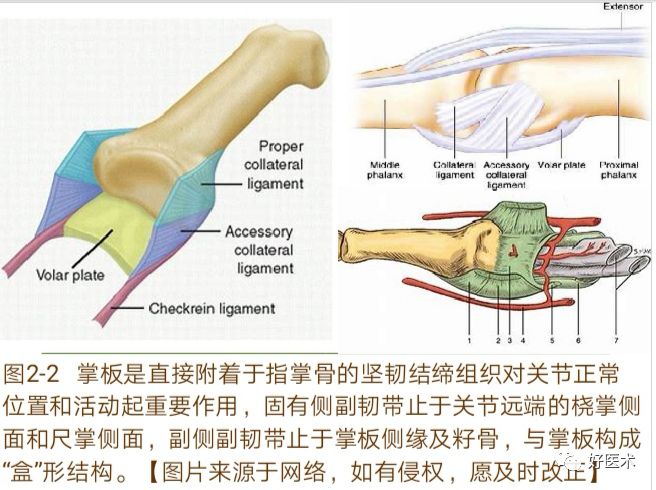
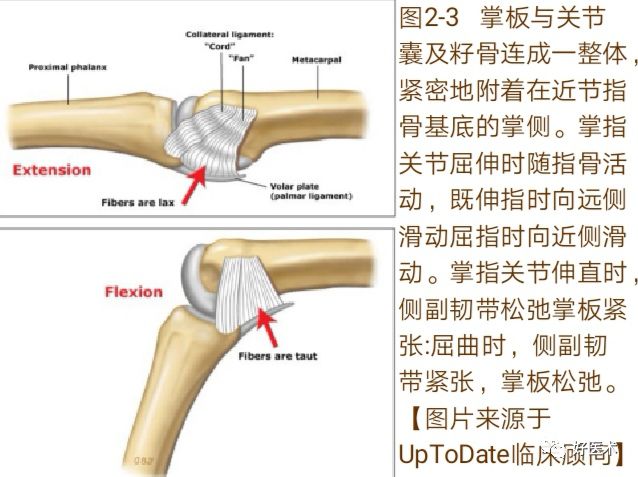
1. Anatomy
2. Causes and Mechanisms


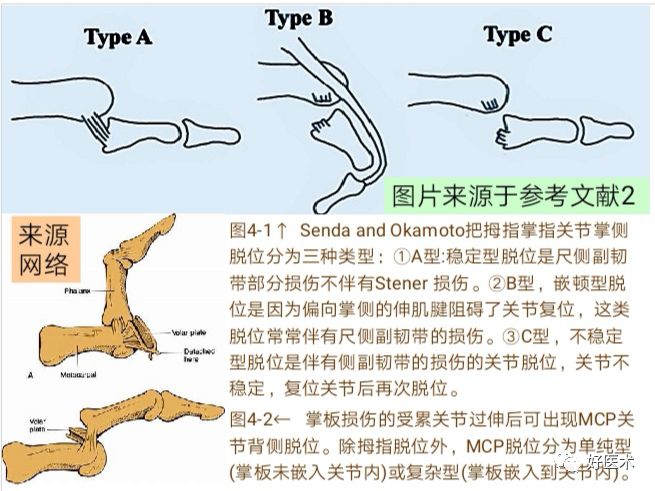
3. Classification
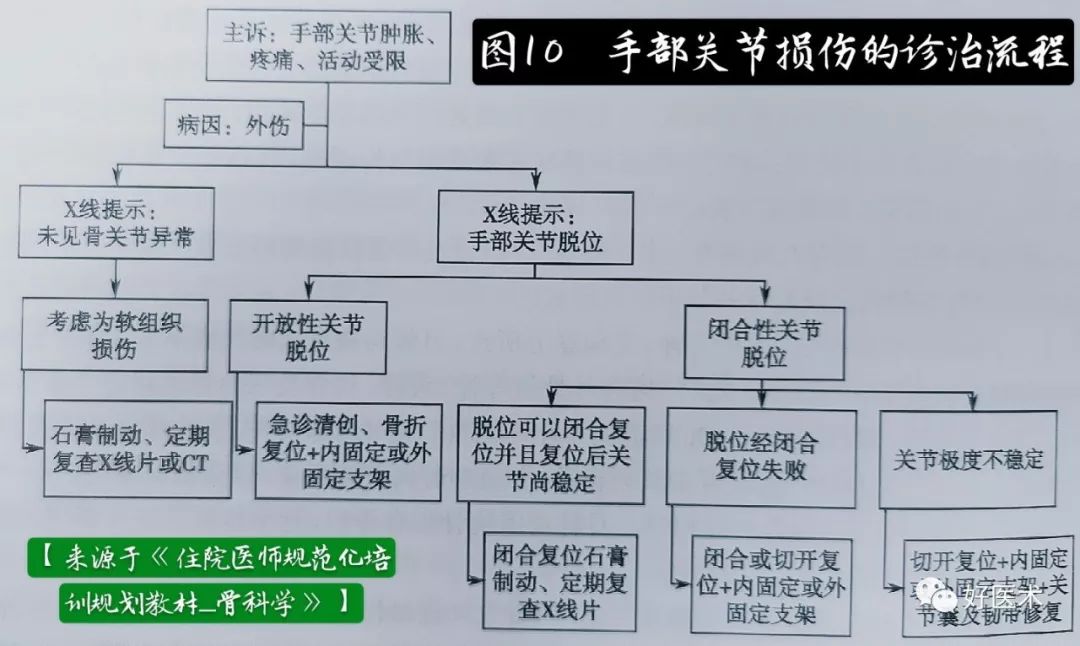
4. Clinical Diagnosis

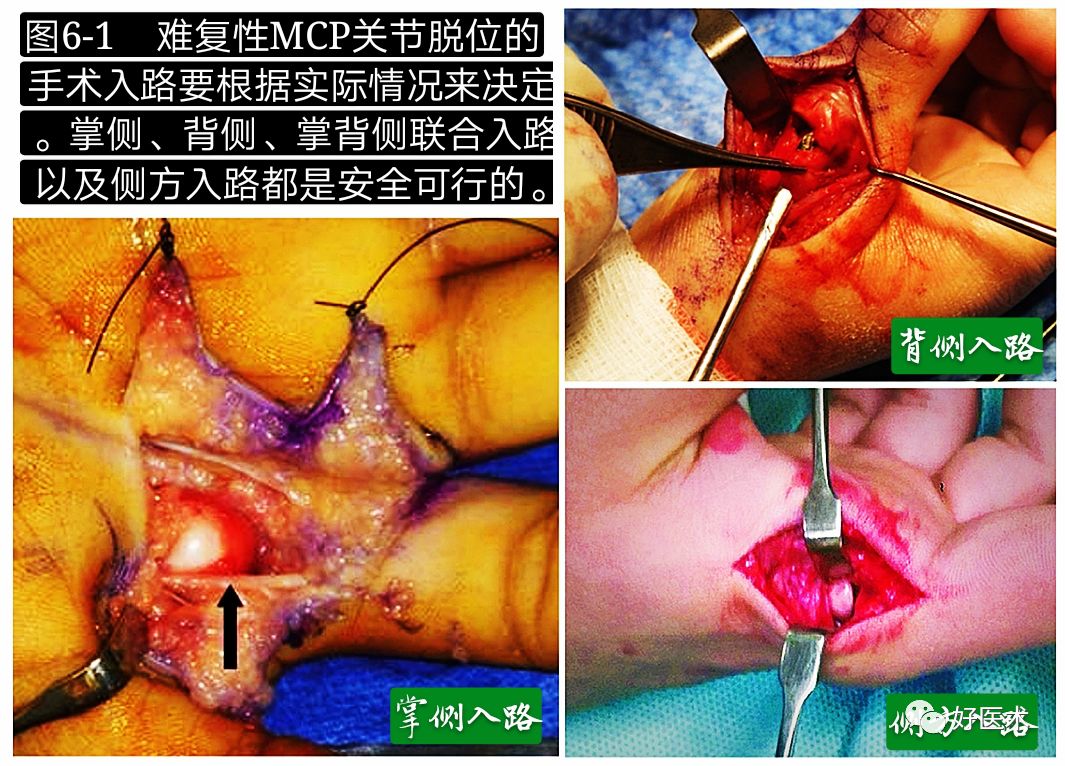
5. Treatment
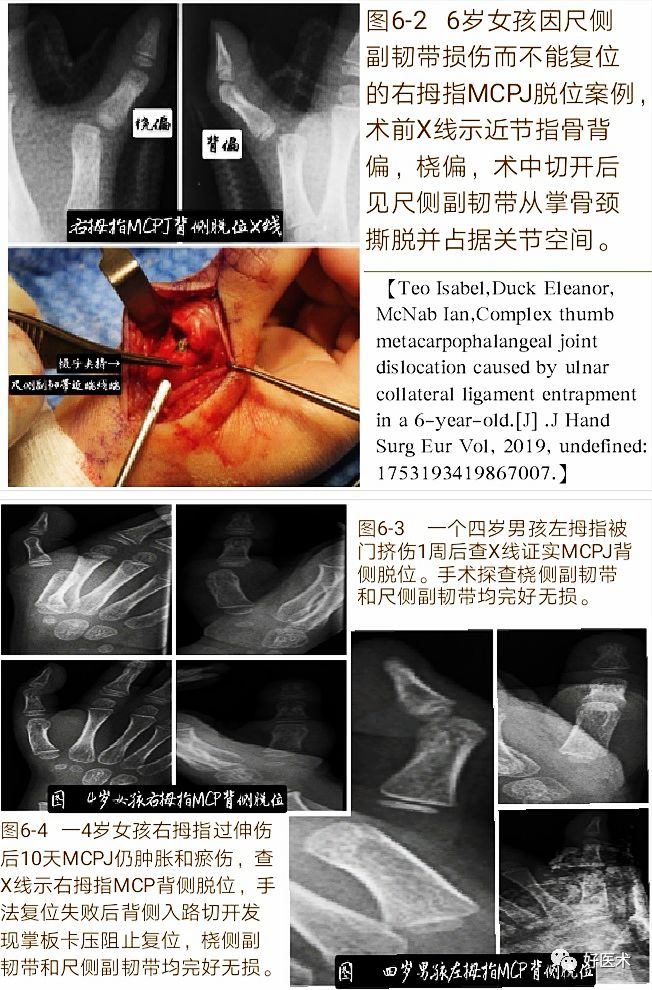
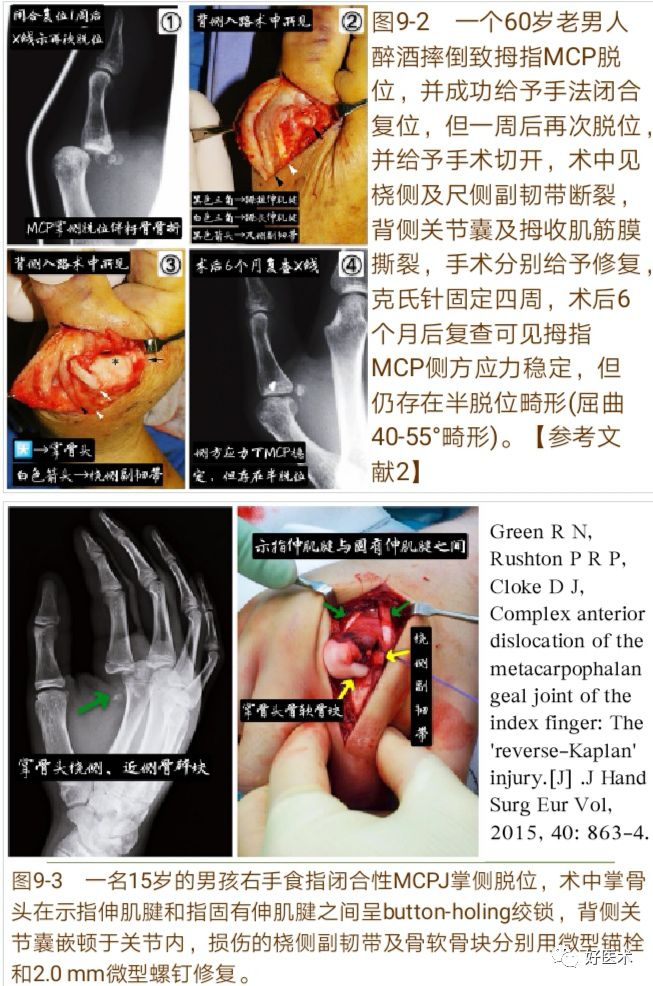
1. Treatment of Dorsal Dislocation


2. Treatment of Palmar Dislocation

6. Complications
Recommended Reading

Yan Xingchao
Orthopedics, Weihai People’s Hospital
From 2012 to 2015, I studied for a master’s degree in the Department of Hand and Foot Surgery at the First Hospital of Jilin University. After graduation, I have been working in the Hand and Foot Surgery department of Weihai People’s Hospital. In 2017, I participated in the standardized training for orthopedic residents and am currently undergoing standardized training at Weihai Municipal Hospital.