The middle cerebellar peduncles are a unique anatomical structure within the skull, which are specific in certain diseases such as demyelination and neurodegenerative changes, aiding in disease diagnosis. This article starts with the anatomy of the middle cerebellar peduncles, delving into pathological mechanisms, imaging manifestations, and differential diagnostic thinking, helping everyone to better understand and remember related diseases.
Published by the author on Medical Pulse. Please do not reproduce without authorization.
The middle cerebellar peduncles (MCP) aggregate the main afferent fibers of the cerebellum, primarily composed of white matter fibers from the contralateral pontine nuclei (a gray matter structure dispersed along the cortical-pontine-cerebellar pathway, responsible for closed-loop communication between the cerebellum and the anterior central/prefrontal cortex, controlling the initiation, drive, and execution of movement). The ratio of afferent to efferent pathways in the cerebellum is quite high (40:1) — the superior cerebellar peduncles (SCP) are the only efferent fibers, connecting the dentate nucleus to the cortex via the dentate nucleus-red nucleus-thalamus tract. The cerebellar pathways cross twice, once at the level of the pons (pons crossing fibers) and again at the level of the inferior colliculus (SCP crossing). Therefore, clinical symptoms (such as limb ataxia) associated with MCP lesions are ipsilateral, while gait difficulties (cerebellar ataxia), dysarthria (speech interruption), vertigo, and facial weakness are common clinical manifestations of MCP lesions.
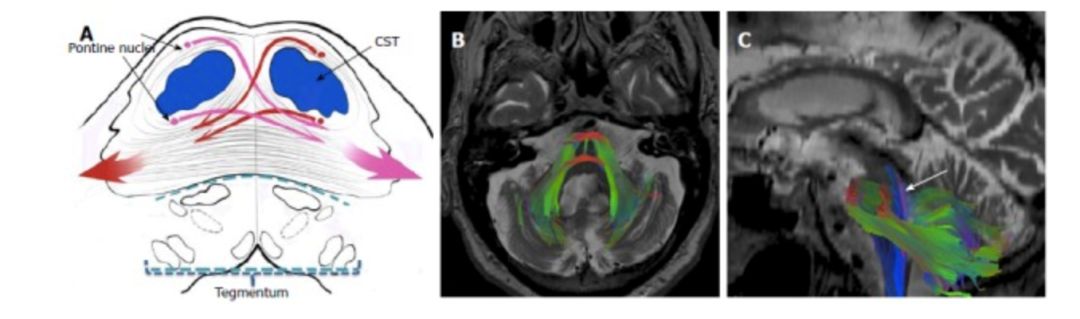
Figure 1 Anatomy of the Middle Cerebellar Peduncles
(A) The image shows the pontine crossing fibers (PCF) originating from the contralateral pontine nuclei (red and pink long arrows) constituting the middle cerebellar peduncles (MCP) (composed solely of afferent fibers);(B, C) Target ROIs (regions of interest) located in the bilateral MCP shown in the fiber tract structure displayed by diffusion tensor imaging (DTI), with PCF in red. The “cross-bun” sign or “trident” sign appearing in the conventional T2 sequence is associated with the PCF or central pontine and affected corticospinal tract (CST) with the midbrain retention. Sagittal DTI (C) shows the main efferent pathways (purple ascending fibers, arrows), forming part of the dentate nucleus-red nucleus-thalamus tract through the pontine and cerebellar peduncles.
There are multiple mechanisms for MCP lesions, primarily related to myelin damage, as detailed in Table 1.
Table 1 Introduction to Different Mechanisms of MCP Lesions
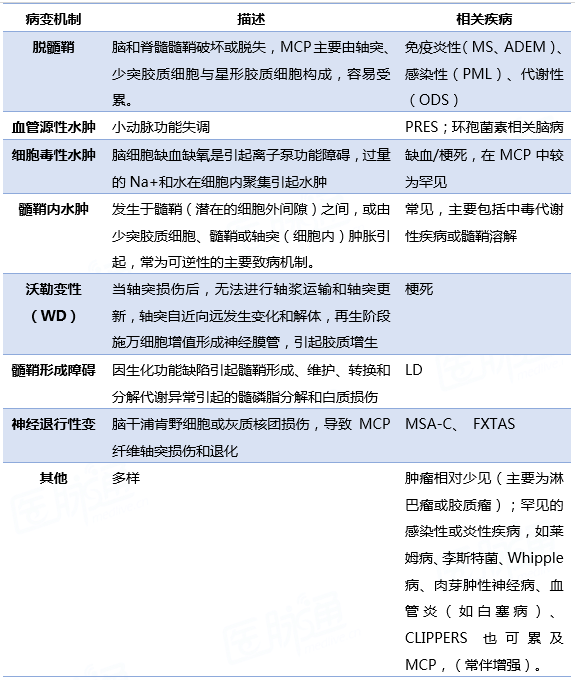
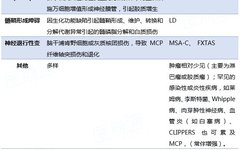
Note:ADEM, acute disseminated encephalomyelitis; CLIPPERS, chronic lymphocytic inflammation with pontine and cerebellar vessel enhancement responsive to steroid treatment; FXTAS, fragile X-associated tremor/ataxia syndrome; MSA-C, multiple system atrophy; LD, leukodystrophy; ODS, osmotic demyelination syndrome; PML, progressive multifocal leukoencephalopathy; PRES, posterior reversible encephalopathy syndrome; WD, Wallerian degeneration.
Imaging Manifestations of Different Diseases
50%-80% of multiple sclerosis (MS) patients may exhibit cerebellar symptoms and signs, with the incidence of brainstem and cerebellar lesions on MRI being 68% and 49%-88%, respectively.
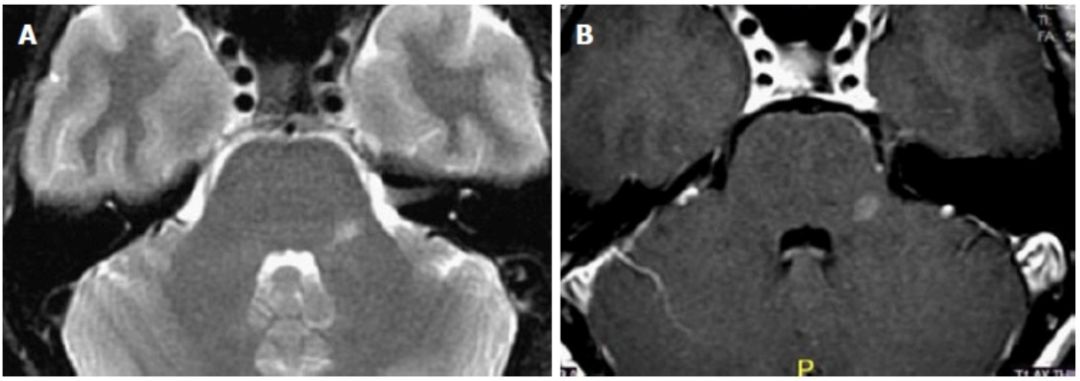
Figure 2 Multiple Sclerosis (Isolated Lesion on Left MCP)
Progressive multifocal leukoencephalopathy (PML) presents as multifocal demyelination with vacuolation, and inflammatory lymphocyte infiltration is rare. The posterior fossa involvement in PML accounts for approximately 58%, with MCP involvement ranging from 64%-100%. The course of PML often lasts for several months, leading to neurological impairment, dementia, and death. Most patients may exhibit white matter lesions that generally do not worsen; if they do worsen, infection, inflammatory response, or tumor reaction should be considered.
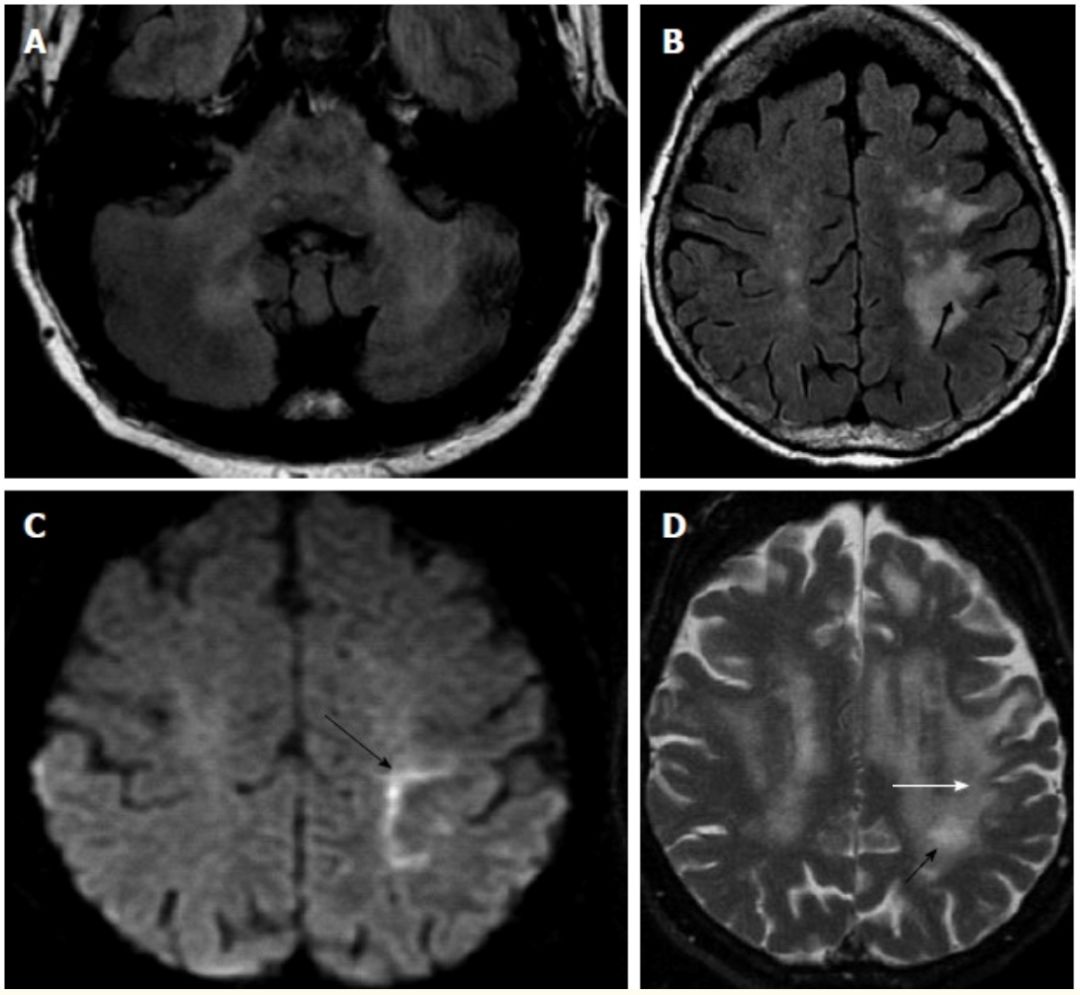
Figure 3 Progressive Multifocal Leukoencephalopathy (PML)
(A) Axial FLAIR images show bilateral MCP involvement;Axial FLAIR (B) and DWI (C) images show asymmetric fused subcortical white matter hyperintensity, U-fiber involvement (arrow), and the linear “edge” on DWI (arrow on C) consistent with the direction of demyelination progression; (D) After three months, white matter lesions progress, and U-fiber involvement is more obvious (white arrow), with characteristic small central cavities/microcysts of PML visible (black arrow).
Changes in the immune system (such as highly active antiretroviral therapy for AIDS) can sometimes cause a paradoxical inflammatory response in the central nervous system, known as IRIS (immune reconstitution inflammatory syndrome). IRIS can be associated with tumors, fungal, or bacterial infections, making it easy to confuse; however, steroids are effective in supporting the diagnosis of IRIS.
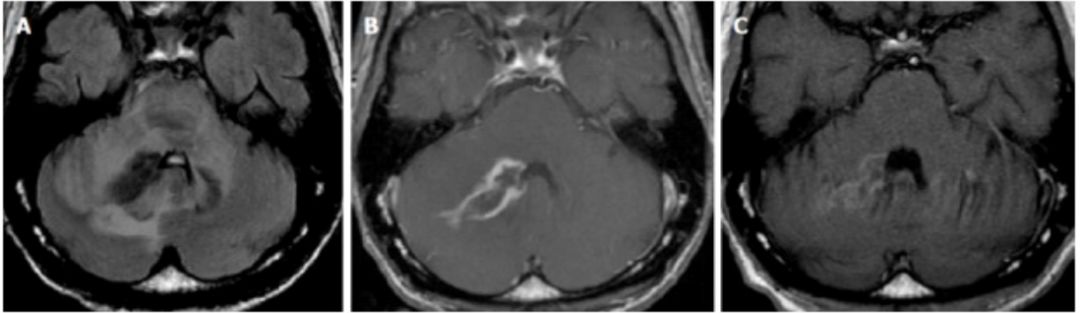
Figure 4 Immune Reconstitution Inflammatory Syndrome—Progressive Multifocal Leukoencephalopathy (IRIS—PML)
Axial FLAIR (A) and contrast-enhanced axial sequences (B) show bilateral MCP asymmetry with high signal, more extensive on the right, accompanied by enhancement; (C) After 2 months of steroid and antiretroviral treatment, significant improvement is observed in the enhancement sequence.
Approximately 18% of patients with reversible posterior leukoencephalopathy syndrome (PRES) have brainstem involvement, and about 4% (the main variant of PRES) may show isolated lesions in the brainstem or basal ganglia (without cortical or subcortical edema).

Figure 5 Reversible Posterior Leukoencephalopathy Syndrome (PRES)
(A, B) Axial FLAIR images in hypertensive patients show symmetric bilateral abnormal signals in MCP and pons, with “vascular edema” visible in the subcortical white matter (arrow on B);(C, D) After three months of hypertension control, lesions in MCP, pons, and supratentorial regions disappear.
Osmotic demyelination syndrome (ODS) is primarily secondary to long-term alcohol use and rapid correction of hyponatremia, leading to demyelination, with imaging showing lesions sparing the pontine margin and corticospinal tract while involving the center (the “trident” sign). Some patients may exhibit diffusion restriction on DWI during the acute phase, but not crossing the midline (to differentiate from ischemic injury).
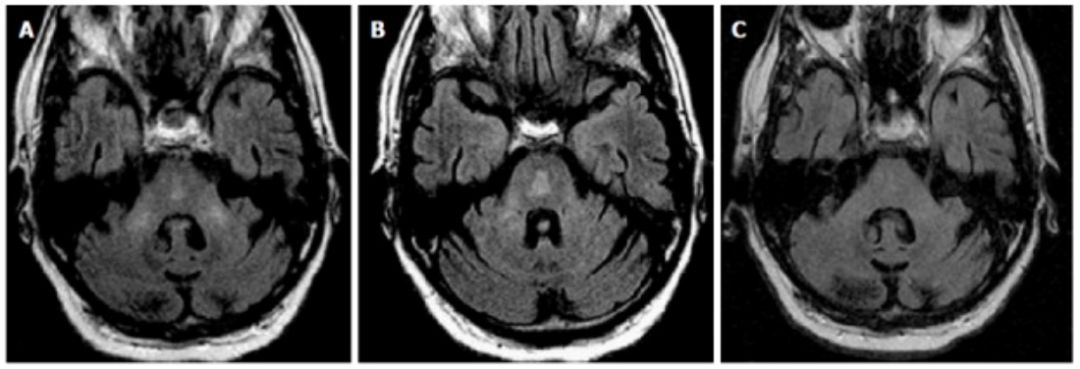
Figure 6 Osmotic Demyelination Syndrome (ODS)
(A, B) Two different axial levels of the pons on FLAIR images show bilateral MCP abnormal signals, with central abnormal signals presenting a slight “trident” appearance;(C) After three months, the abnormal signals in MCP and pons are reduced.
Heroin intoxication can also lead to MCP involvement, characterized in the initial stage by diffuse leukoencephalopathy, which is challenging to distinguish from hypoxic-ischemic disease (the latter often involves the cortex), with restricted diffusion visible in the lesion area, associated with acute myelin edema or excitotoxic edema. This process is reversible, or may lead to chronic lesions, or spongiform leukoencephalopathy (often involving posterior white matter, midbrain, and bilateral MCP). Other toxic drugs such as toluene or methotrexate can also cause cerebellar and MCP lesions.
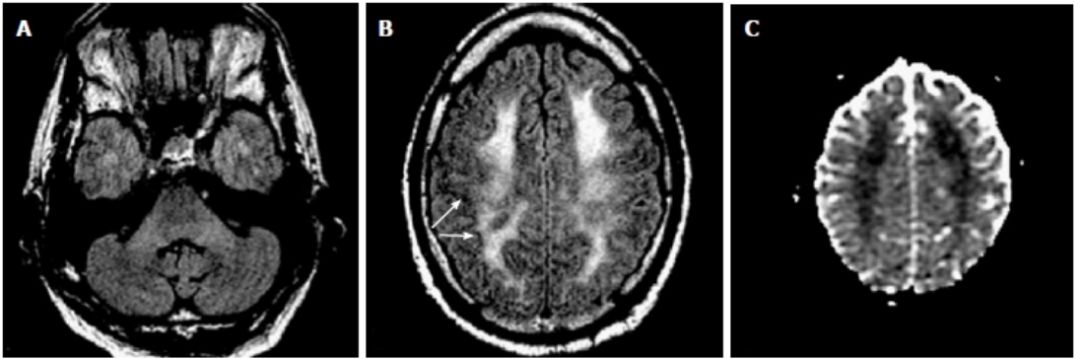
Figure 7 White Matter Disease Induced by Acute Heroin Intoxication
(A) Axial FLAIR images show mild enhancement of MCP signal;Axial FLAIR (B) and ADC images (C) show consistent diffuse and fused white matter hyperintensity, restricted diffusion, and preserved subcortical—U-fibers (arrow on B) and cortex.
Wilson’s disease is characterized by the loss of neurons in the putamen and caudate nucleus, with reduced volume, and abnormal signals in the midbrain tegmentum presenting as “panda face sign.” MCP involvement is rare overall, though it can be seen in the early or “active” phases of the disease.
The MCP is primarily supplied by the anterior inferior cerebellar artery (AICA), with partial supply from the superior cerebellar artery. Isolated AICA infarction due to thromboembolism or severe atherosclerotic disease of the basilar artery and branches is relatively rare, with corresponding high signals observed in MCP on DWI.
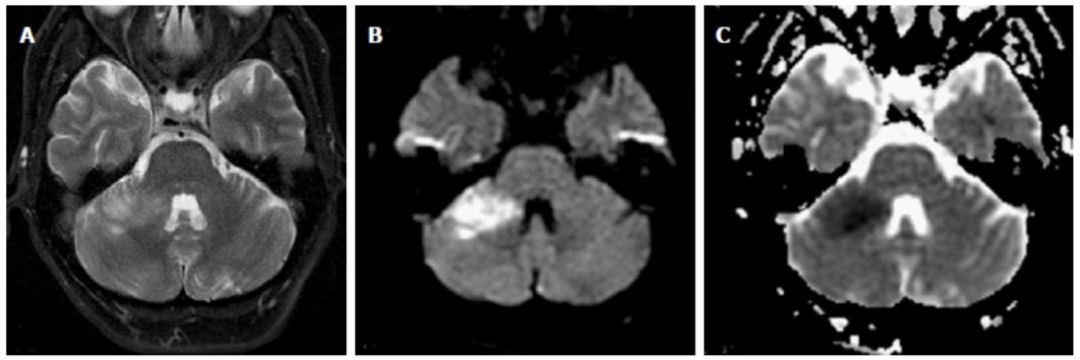
Figure 8 Anterior Inferior Cerebellar Artery (AICA) Infarction
Axial T2 (A), DWI (B), and ADC images (C) show lesions consistent with the local ischemic area in the T2 high signal region.
Wallerian degeneration (WD) of the MCP can occur during ischemia or hemorrhage of the pons, with T2 high signals commonly seen in the third stage of WD, which appears 10-14 weeks after axonal injury.
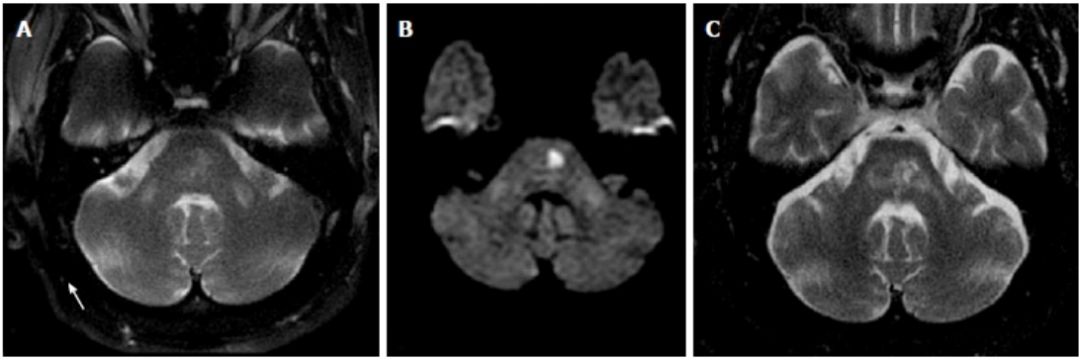
Figure 9 Wallerian Degeneration (WD)
Axial T2 (A), DWI (B) images show symmetrical abnormal signals in bilateral MCP, with restricted diffusion in the left pons (characteristic retention in the midline area due to occlusion of the basilar artery’s paramedian branches);Axial T2 images (C) show progression of pontine lacunar infarction three years later, with reduced abnormal signals in the right MCP, persistent abnormal signals in the left MCP, and further atrophy of the lesions. The “acute” early changes in bilateral MCP and greater left-sided involvement during follow-up (ipsilateral infarction) are consistent with the WD process of MCP.
Multiple system atrophy (MSA) is a sporadic neurodegenerative disease, clinically presenting with Parkinson’s disease, autonomic nervous system symptoms, cerebellar symptoms, or pyramidal signs. Previously classified as Shy-Drager syndrome, striatal nigral degeneration, and olivopontocerebellar atrophy, the latest classification highlights widespread loss of neurons in the cerebellum, pons, and olivary nucleus, and subsequent degeneration of MCP as the main feature of MSA-C type, with approximately 43% of MSA-C patients showing homogeneous atrophy and abnormal signals in MCP on T2 images.
Fragile X-associated tremor/ataxia syndrome (FXTAS) is a hereditary disease related to overexpression of the FMR1 gene, more common in males, accompanied by progressively worsening ataxia. Pathologically, ubiquitin-positive eosinophilic nuclear inclusions appear in the brain, especially in the hippocampus and in cerebellar neurons and astrocytes outside of Purkinje cells, while Purkinje cells mainly show axonal degeneration and neuronal loss. Unlike MSA, FXTAS inclusions mainly appear in neural nuclei, neurons, and astrocytes, while MSA mainly appears in cytoplasm and oligodendrocytes. Up to 82% of FXTAS patients exhibit abnormal signals in MCP.
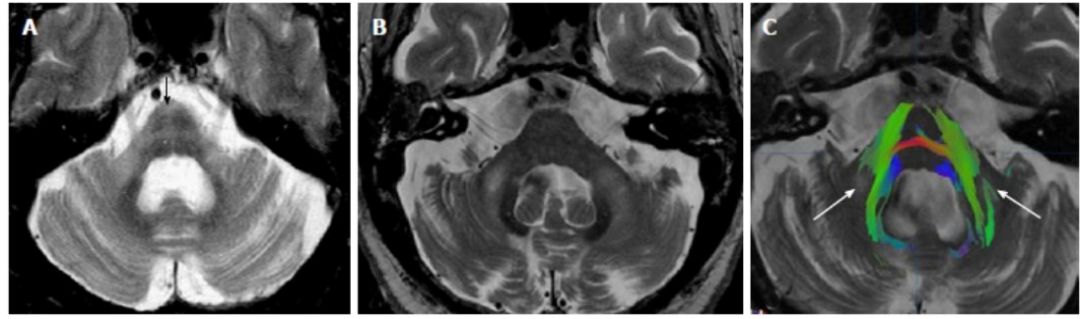
Figure 10 Multiple System Atrophy (MSA-C) and Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS)
Axial T2 (A) images show pontine atrophy in MSA-C patients, with degeneration of MCP and crossing fibers (“cross-bun sign,” black arrow), and T2 high signals in bilateral MCP.Axial T2 (B) and diffusion tensor imaging (DTI) fiber tract imaging (C) show reduced cerebellar volume and increased T2 signals in FXTAS patients, with reduced MCP volume. Due to reduced fractional anisotropy (white arrow on C), no fiber imaging is visible in the T2 signal abnormal area on DTI.
LD is a hereditary metabolic disorder that causes biochemical defects leading to myelin formation disorders. LD is associated with peroxisomal defects (such as adrenal leukodystrophy) or lysosomal defects (such as metachromatic LD). LD can affect MCP but is often accompanied by symmetric involvement of supratentorial white matter, with preservation of subcortical U-fibers. Some rare forms of LD, such as Canavan or Pelizaeus-Merzbacher disease (PMLD), may involve subcortical U-fibers.
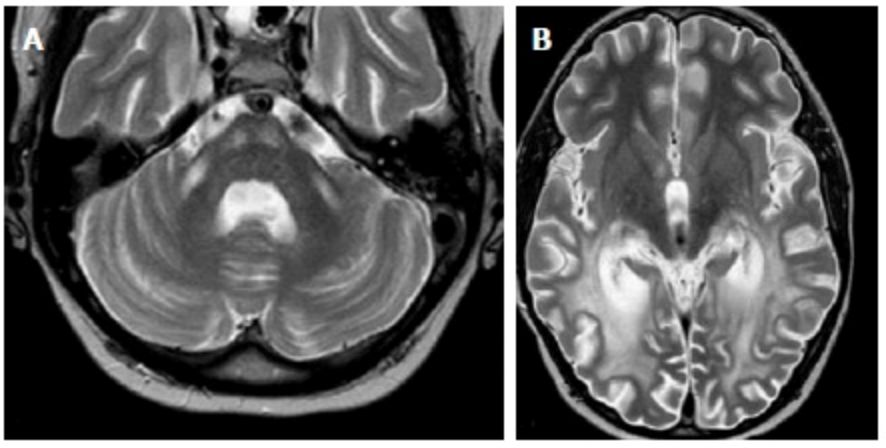
Figure 11 Adrenal Leukodystrophy (ADL)
(A) Axial T2 images show symmetric T2 high signals in MCP and bilateral corticospinal tracts;(B) Axial T2 images show symmetric white matter fusion high signals in bilateral occipital-parietal regions, preserving subcortical U-fibers, typical imaging manifestations of ADL.
ADEM or meningitis can affect MCP, possibly related to recent systemic infections or vaccinations. The most common associated viruses are varicella, mumps, measles, rubella, and rotavirus. Bacterial infectious diseases such as Lyme disease, listeriosis, or Whipple’s disease may also affect the posterior cranial fossa and damage MCP, but are less common.
Diagnosis and Differentiation
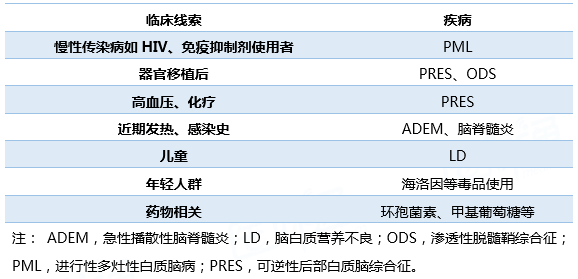
When MCP lesions appear, it is necessary to combine the patient’s general condition to find clues; possible clues are summarized in Table 2.
Table 2 Diseases Related to MCP Involvement and Clues
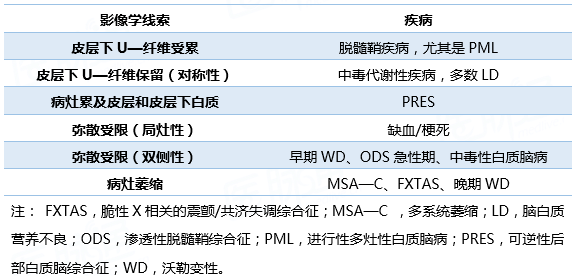
The distribution characteristics of MCP involvement can aid in differentiating related diseases, as seen in Table 3.
Table 3 Imaging Clues of Different Diseases Related to MCP
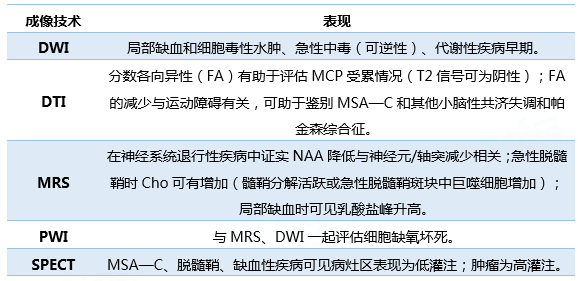
Different diseases related to MCP involvement can be differentiated through MRI imaging, where DWI and DTI hold significant diagnostic value; other imaging techniques include magnetic resonance spectroscopy (MRS), magnetic resonance perfusion imaging (PWI), and single-photon emission computed tomography (SPECT), as detailed in Table 4.
Table 4 Relevant Imaging Techniques for Differentiating MCP Lesions
3. Summary
MCP involvement is common in neurodegenerative diseases and demyelinating diseases. When T2 high signals appear on MCP during routine MRI scans, a preliminary evaluation based on the general condition is necessary to find clinical clues, followed by further imaging examinations to clarify the general direction of the disease.
References:
[1] Humberto M , Thomas T . Middlecerebellar peduncles: Magnetic resonance imaging and pathophysiologiccorrelate[J]. World Journal of Radiology, 2015, 7(12):438.
[2] Miall R C.Cerebellum: Anatomy and function[J]. Neuroscience in the 21st Century: FromBasic to Clinical, 2016: 1277-1295.
[3] Zhang Z Y, Liu Z Q, Qin W, etal. Clinical and Radiological Features of Wallerian Degeneration of the MiddleCerebellar Peduncles Secondary to Pontine Infarction[J]. Chinese MedicalJournal, 2018, 131(6):665.
[4] Dong Q, Jing G, Han J. Theendovascular treatment of bilateral infarction of middle cerebellar peduncles.Etiology and endovascular treatment analysis. [J]. Neurosciences, 2017, 22(1):56.
[5] Paucar M, Engvall M, Gordon L,et al. POLG-Associated Ataxia Presenting as a Fragile X Tremor/Ataxia PhenocopySyndrome[J]. Cerebellum, 2016, 15(5):1-4.