First Author: Wang Ruoran, Wang Leping
Corresponding Author: Xu Jianguo
Author Affiliation: West China Hospital, Sichuan University
[REF: Wang R, Wang L, Zhang J, He M, Xu J. XGBoost Machine Learning Algorithm Performed Better Than Regression Models in Predicting Mortality of Moderate-to-Severe Traumatic Brain Injury [published online ahead of print, 2022 Apr 14]. World Neurosurg. 2022;S1878-8750(22)00492-2. doi:10.1016/j.wneu.2022.04.044] PMID: 35430400
Moderate to severe traumatic brain injury (TBI) has drawn significant attention due to its high disability and mortality rates. To prevent disease progression and adverse outcomes in TBI patients, clinicians should classify the severity of injuries and early identify high-risk patients with poor prognosis.
The Glasgow Coma Scale (GCS) has been proposed and used clinically for decades, yet it still has limitations in assessing the severity of TBI. Consequently, many previous studies have constructed more stable and accurate risk scores for TBI patients, such as IMPACT, CRASH, and Marshall. All these predictive models were developed based on generalized linear methods, including logistic regression and Cox proportional hazards regression. However, many risk factors may have a nonlinear relationship with patient outcomes, making traditional linear regression models inadequate in reasonably incorporating these variables.
Machine learning can automatically develop models based on data and make clinical decisions to assist physicians in their daily work. Previous studies have explored the value of several classical machine learning algorithms, including decision trees, random forests, support vector machines, and naive Bayes, in predicting outcomes for TBI patients. The Extreme Gradient Boosting (XGBoost) algorithm, designed by Chen Tianqi, has performed well in terms of computational speed and model accuracy, gaining widespread attention from medical researchers across various fields. This study aims to validate the predictive value of XGBoost for mortality in moderate to severe TBI patients and compare its accuracy with traditional logistic regression-based prognostic models.
Inclusion Criteria and Research Route
This study included patients admitted to West China Hospital for TBI from January 2015 to June 2019. The exclusion criteria were as follows: (1) GCS > 13 at admission; (2) admitted more than 6 hours after the first TBI; (3) transferred from other medical centers; (4) incomplete recording of required variables. After screening, 368 patients with moderate to severe TBI were included in this study.
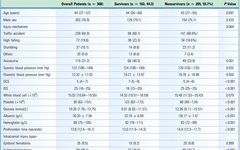
Patient data recorded included age, gender, mechanism of injury, pupil size disparity, blood pressure, GCS at admission, and injury severity score. Laboratory test indicators were collected, including white blood cell count, platelet count, glucose, albumin, hemoglobin, and prothrombin time. Types of intracranial injuries identified via CT and MRI were recorded, including epidural hematoma, subdural hematoma, subarachnoid hemorrhage, and diffuse axonal injury.
The mortality rate among the 368 patients with moderate to severe TBI included in this study was 55.7%. Compared to survivors, non-survivors had lower GCS scores (p < 0.001) and higher injury severity scores (p < 0.001). Laboratory test results showed that non-survivors had significantly higher glucose levels (p < 0.001) and prothrombin times (p < 0.001) compared to survivors, while platelet counts (p < 0.001), albumin (p < 0.001), and hemoglobin (p < 0.001) were significantly lower in non-survivors. Additionally, the incidence of subdural hematoma was significantly higher in non-survivors (p < 0.001). Finally, the ICU stay (p < 0.001) and hospital stay (p < 0.001) were shorter for the non-survivor group. (Table 1)

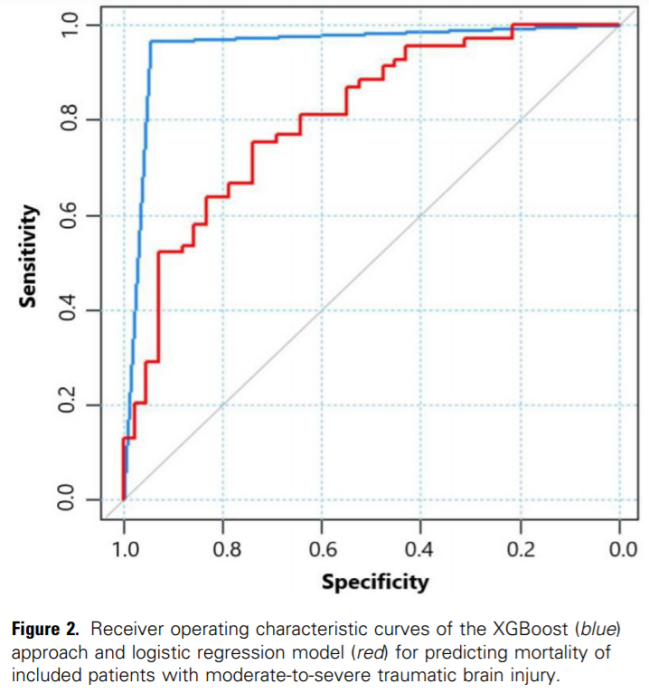
In the XGBoost model, GCS, prothrombin time, and glucose ranked as the top three in feature importance (Figure 1). The AUC for the XGBoost model predicting mortality was 0.955, significantly higher than the 0.805 of traditional logistic regression (Figure 2). The accuracy, sensitivity, and specificity of the XGBoost model were 0.955, 0.945, and 0.964, respectively. In contrast, the accuracy, sensitivity, and specificity of traditional logistic regression were 0.703, 0.738, and 0.754, all lower than those of the XGBoost model. (Table 2)

This study’s results indicate that the XGBoost algorithm outperforms traditional logistic regression in predicting mortality in moderate to severe TBI patients. Previous research has explored the prognostic value of various machine learning algorithms, including support vector machines, decision trees, random forests, naive Bayes, and artificial neural networks in different TBI populations. However, these algorithms have shown varying prognostic values across studies based on different TBI cohorts, with some studies finding that machine learning algorithms do not perform better than traditional logistic regression models. These discrepancies may arise from differences in TBI populations, treatment strategies at different medical centers, and algorithm optimization methods. No studies have explored the prognostic value of the XGBoost algorithm in TBI patients. The XGBoost algorithm is based on gradient-boosted decision trees, utilizing a second-order Taylor expansion to compute the loss function, demonstrating good performance in both computation speed and prediction accuracy.
In our study, the top three features ranked by importance in the XGBoost algorithm were GCS, prothrombin time, and glucose. The GCS, a routinely used tool for assessing the severity of TBI, has shown some limitations under specific clinical conditions. The accuracy of the GCS can be affected by factors such as alcohol, analgesics, sedation, and intubation. Therefore, many studies have designed and developed new prognostic models that combine other clinical and imaging features with GCS to enhance the stability and accuracy of outcome predictions. Prolonged prothrombin time indicates a decline in coagulation function, which may relate to significant bleeding, anemia, pathological consumption of coagulation factors, and hemodilution due to large-volume crystalloid infusions in trauma patients. Prior literature reports that the incidence of coagulopathy in TBI patients ranges from 10% to 98%, significantly correlating with prognosis. In our study, the median prothrombin times for survivors and non-survivors were 13.0 and 14.9, respectively, indicating a significant proportion of the included TBI patients exhibited coagulation dysfunction. As a recognized risk factor for poor prognosis in TBI, hyperglycemia may be associated with coagulopathy, worsening brain metabolism, neuroinflammation, and apoptosis. In addition to GCS, prothrombin time, and glucose, other factors such as pupil size disparity, diastolic pressure, injury severity score, age, white blood cells, platelets, and albumin also showed varying degrees of importance in the XGBoost model. Based on these features, our developed XGBoost model performed excellently in predicting inpatient mortality for moderate to severe TBI, with an AUC of 0.955. Prognostic models based on the XGBoost algorithm can assist clinicians in assessing mortality risk in moderate to severe TBI patients, enabling appropriate treatment strategies and enhanced medical supervision.
The XGBoost method is more effective and accurate than logistic regression in predicting mortality in moderate to severe TBI patients. In the future, creating a user-friendly program based on the XGBoost algorithm for mobile devices will help identify TBI patients at high risk of mortality, guiding healthcare professionals in formulating appropriate treatment plans.
West China Hospital, Sichuan University
-
Department of Neurosurgery, West China Hospital, Sichuan University
-
First-year PhD student, majoring in neuro-oncology and neurocritical care
-
Published multiple SCI papers as the first author, with a highest impact factor of 5.71
-
Participated in a project funded by the Sichuan Provincial Science and Technology Department as the first principal investigator
-
Awarded the National Scholarship in 2020
-
Reviewer for Frontiers series journals
Corresponding Author Biography
West China Hospital, Sichuan University
-
Medical postdoctoral fellow, professor, chief physician, doctoral supervisor, and director of neurosurgery
-
Leader in academic and technology in Sichuan Province, standing committee member of the Neurosurgery Branch of the Chinese Medical Doctor Association, deputy leader of the Skull Base Surgery Group, deputy director of the Skull Base Surgery Branch of the China International Medical Exchange Promotion Association, deputy director of the Neurosurgery Branch of the China Research Hospital Association, chairman of the Skull Base Neurosurgery Group of the Sichuan Provincial Medical Association, and incoming chairman of the Neurosurgery Branch of the Chengdu Medical Association
-
Specializes in skull base surgery (e.g., pituitary adenomas, craniopharyngiomas, tuberculum sellae meningiomas, anterior clinoid meningiomas, chordomas, etc.), has published over 100 papers in core journals both domestically and internationally, with 63 articles in authoritative foreign journals such as Neurosurgery, J Neurosurg, J Neuro-oncology, and Neurology. He has hosted three general projects funded by the National Natural Science Foundation and received the First Prize of the Chinese Medical Science and Technology Progress Award, the Second Prize of the Ministry of Education Science and Technology Progress Award, and one national invention patent, and was the recipient of the “Wang Zhongcheng Physician Award” in 2016.

Scan the QR code to visitProfessor Xu Jianguo’sAcademic Homepage
See more exciting content
Statement: The intellectual property of the content published by the Brain Medical Exchange, including Neurosurgery Information, Neurointervention Information, Brain Medical Consultation, and AiBrain, belongs to Brain Medical Exchange and the organizers, original authors, and related rights holders. Unauthorized reproduction, excerpting, copying, cropping, recording, etc., is prohibited. Authorized use must also indicate the source. Forwarding and sharing are welcome.
For submissions/conference releases, please contact 400-888-2526 ext. 3.
Brain Medical Exchange App (formerly Neurosurgery Information/ Neurointervention Information App) has launched a new “short video” feature, allowing content learning during fragmented time. Click “Read the original text” below to experience it first!