This article is prohibited from being reproduced without authorization.
 Precious learning opportunity, great price, scan to join immediately.
Precious learning opportunity, great price, scan to join immediately.
The small joints of the hand are all hinge joints. The metacarpophalangeal joints (MCP) have a condylar structure, while the proximal interphalangeal joints (PIP) and distal interphalangeal joints (DIP) have a ball-and-socket shape. Their stability depends on the contour of the joint, collateral ligaments, and the palmar plate. The palmar plate has strong attachments on the sides but is thin at the distal end.
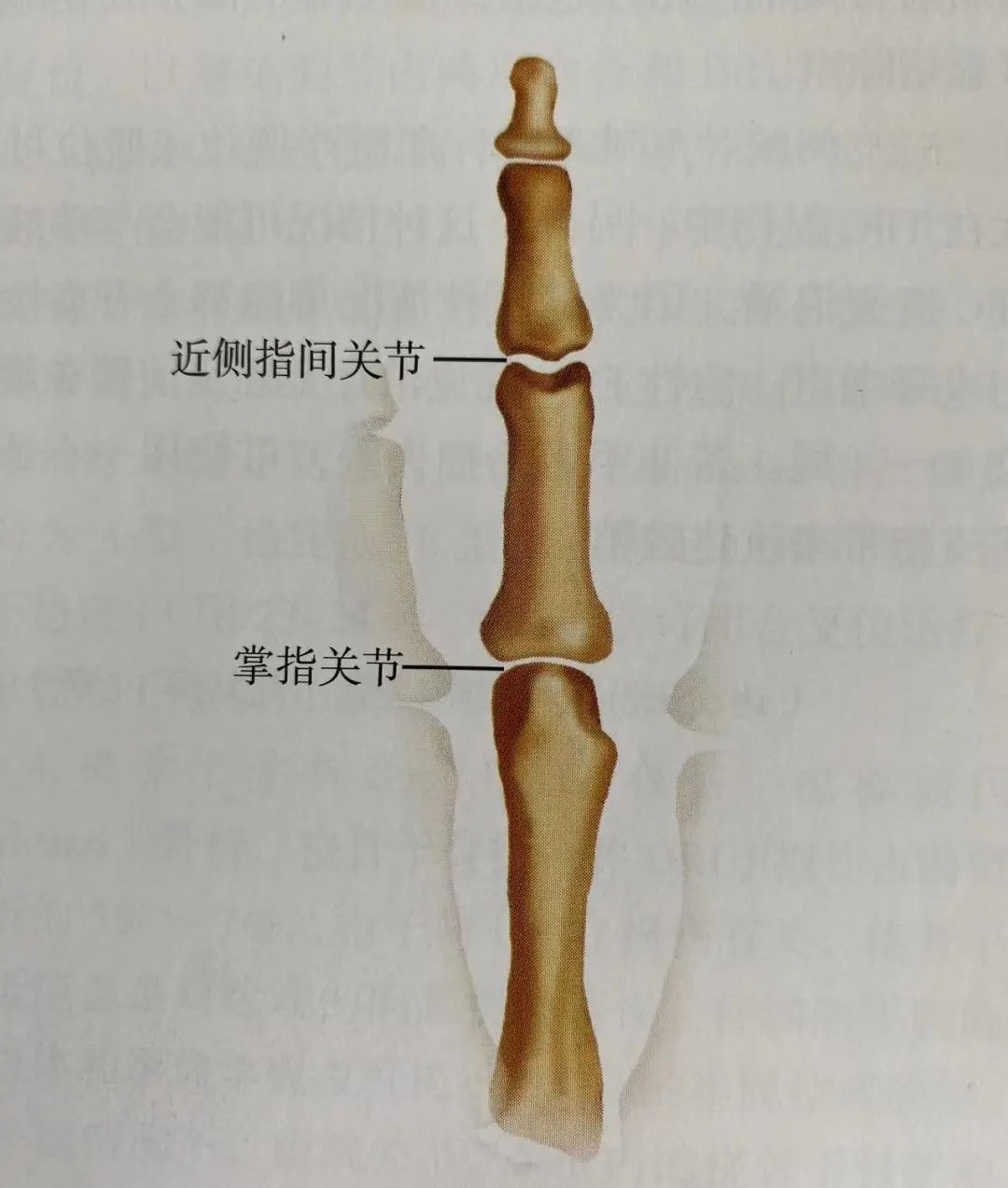 Figure 24-1: The metacarpophalangeal joint is a single condyle, while the proximal interphalangeal joint is a double condyle, making the proximal interphalangeal joint more stable.
Figure 24-1: The metacarpophalangeal joint is a single condyle, while the proximal interphalangeal joint is a double condyle, making the proximal interphalangeal joint more stable.
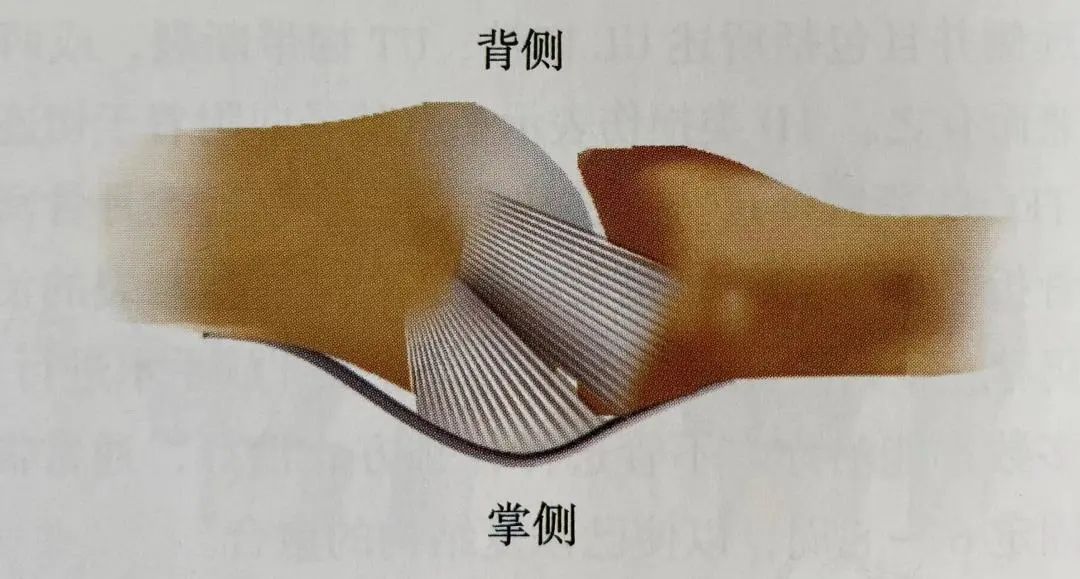
Figure 24-2: The collateral ligaments have a cord-like dorsal part and a fan-shaped palmar part.
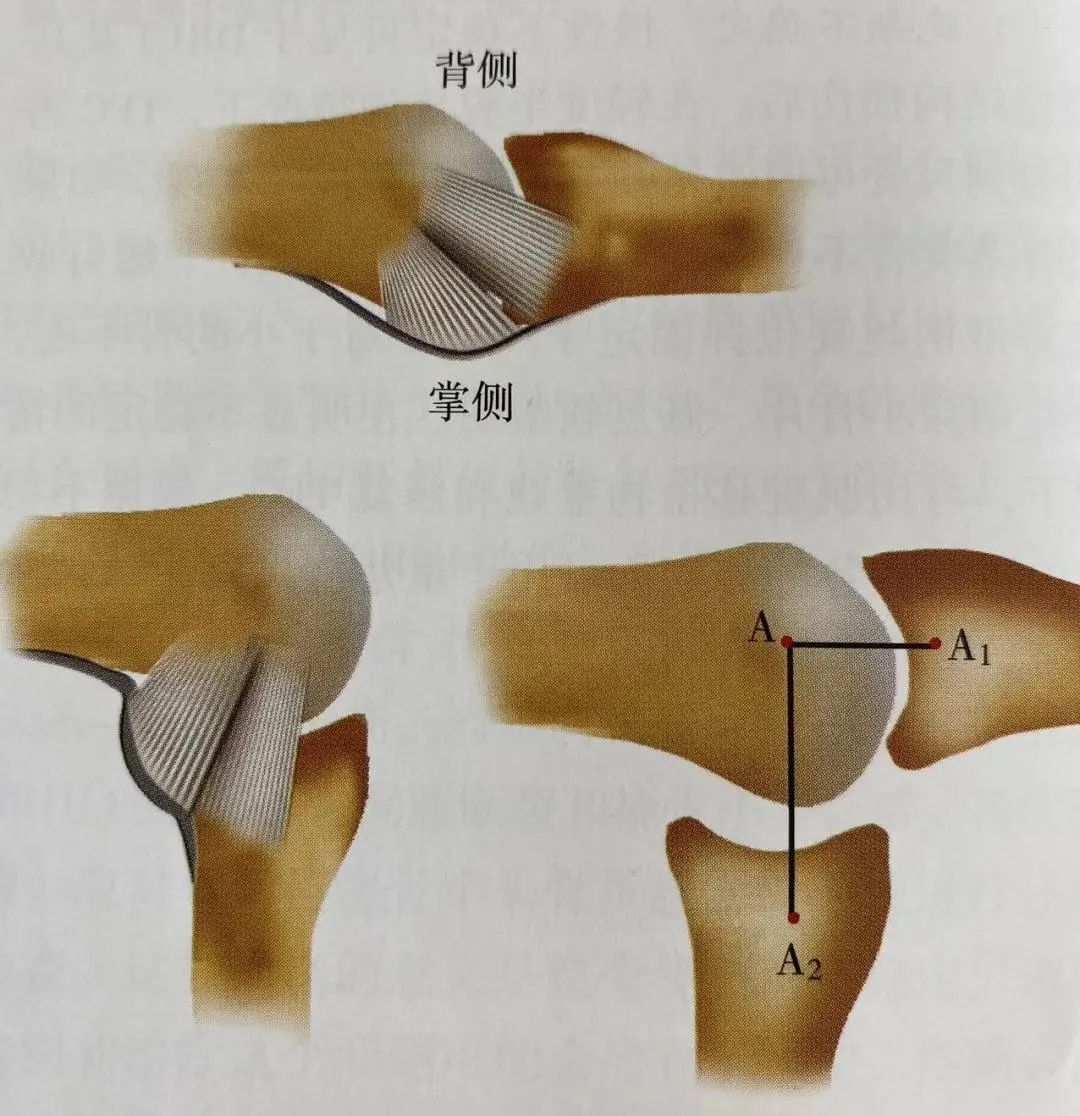
Figure 24-3: The shape of the head of the metacarpal bone is eccentric.
This creates a cam effect, causing the collateral ligaments to be tighter when flexed than when extended (the distance from A to A1 is less than from A to A2).
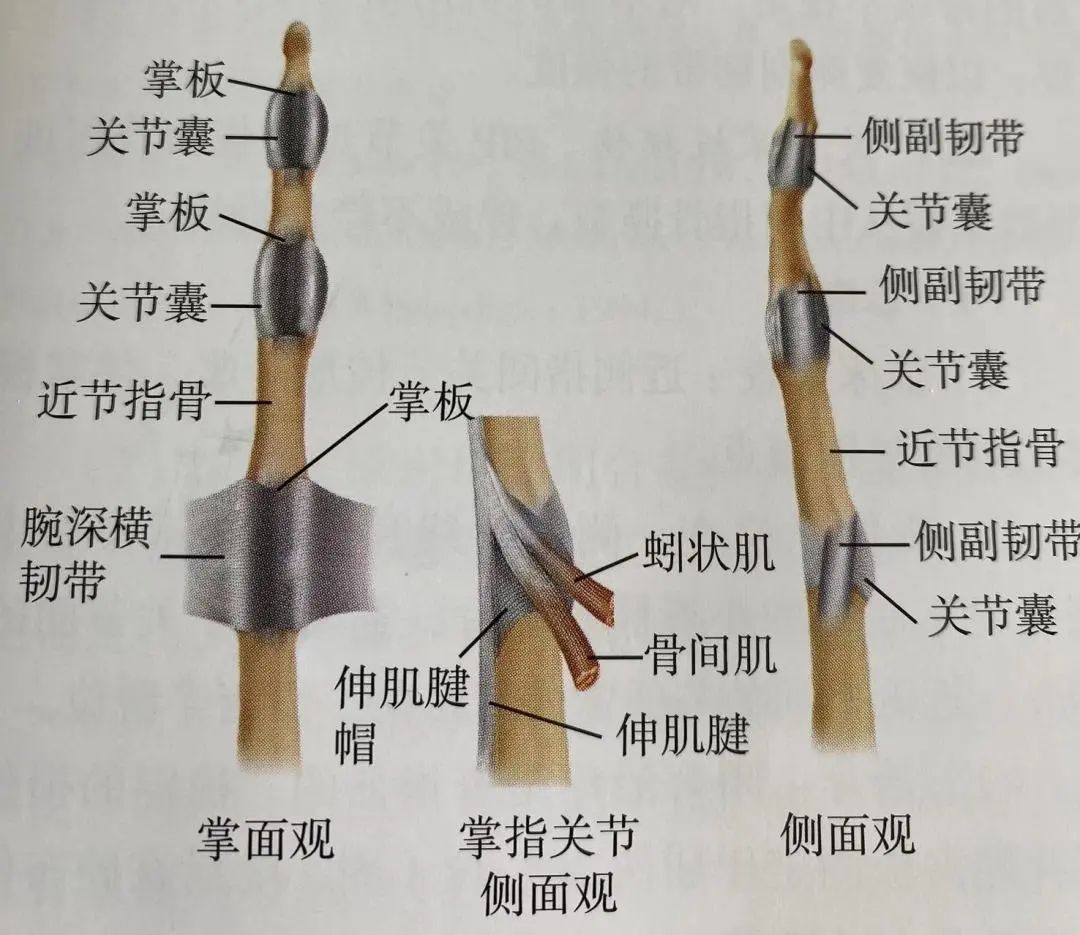
Figure 24-4: Structure of the metacarpophalangeal joint and interphalangeal joints.
A sudden flexion force applied to the DIP joint can tear the extensor tendon from the distal phalanx, with or without fracture fragments. If a large fracture fragment involves more than 30% of the joint surface, there is a risk of palmar subluxation of the distal phalanx.
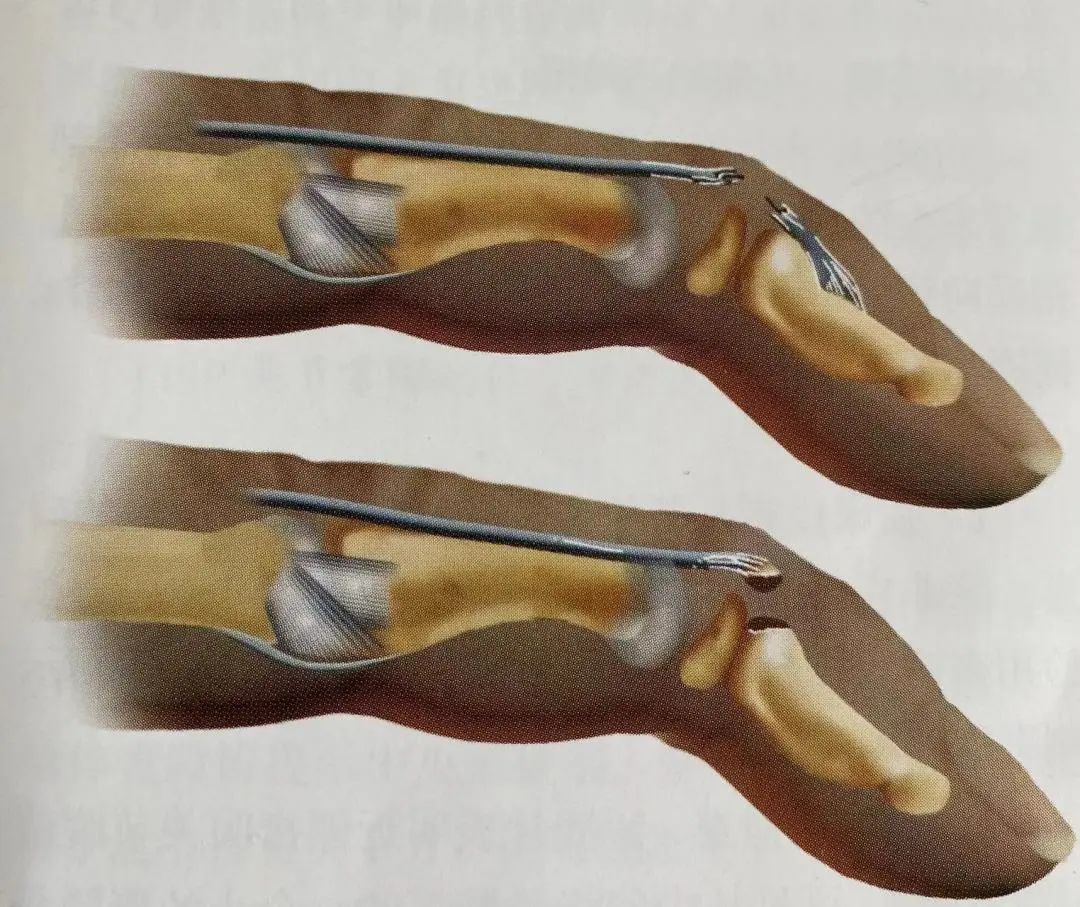
Figure 24-5: Hammer finger.
Soft tissue (tear of the extensor tendon) hammer finger (above) and bony hammer finger (below).
(1) Assessment
Examination reveals pain, swelling, and drooping of the distal interphalangeal joint. X-ray films may show flexion deformity of the DIP joint, with possible fracture fragments attached to the extensor tendon insertion point. Palmar subluxation of the distal phalanx may be associated with fractures, especially when the fracture fragments are large.
(2) Classification of Hammer Finger
-
Type I: Includes closed injuries or blunt injuries, with continuity of the tendon damaged, with or without small fracture fragments.
-
Type II: Involves tearing in the plane of the DIP joint or its proximal part, with continuity of the tendon damaged.
-
Type III: Involves deep abrasion with skin, subcutaneous tissue, and tendon tissue loss.
-
Type IV: Involves avulsion fractures of the phalanx in children, excessive flexion injury resulting in 20%-50% of the joint surface being fractured, or hyperextension injury involving fractures usually greater than 50% of the joint surface, and early or late palmar subluxation of the distal phalanx.
(3) Treatment
-
Non-surgical treatment: For hammer finger injuries with small fracture fragments involving less than 30% of the joint surface or displacement ≥2mm, splinting or casting is recommended. The hammer finger should be fixed in the extended position for 6 weeks, followed by night splinting for 4 weeks (Figure 24-6).
-
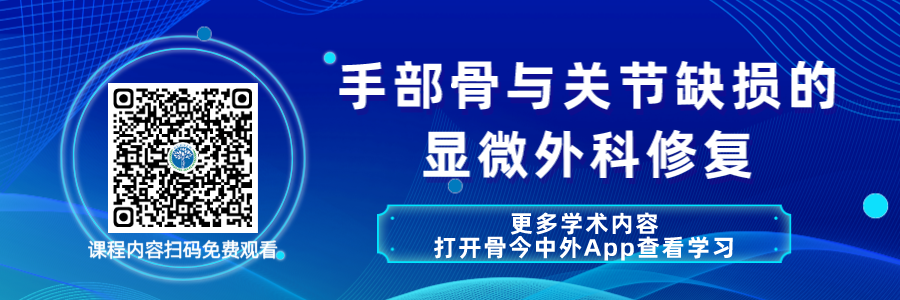
Surgical treatment: Hammer finger deformity and fracture fragments involving more than 30% of the joint surface, with displacement >2mm or associated palmar subluxation of the distal phalanx require surgical treatment. Palmar subluxation of the DIP joint is an absolute indication for surgery. Open reduction and internal fixation (ORIF) is recommended to correct the palmar subluxation of the DIP joint, and to use a longitudinal Kirschner wire to fix the distal interphalangeal joint in the hyperextended position (Figure 24-7). Tendon repair is performed as needed. The pull-out button technique may lead to skin necrosis (below the button). Using suture anchors may be more desirable.

Figure 24-6: Distal interphalangeal joint hammer finger injury fixed in the extended position with a splint.
Using the three-point fixation principle to fill the space between the back of the finger and the splint (arrow position).
Figure 24-7 A. X-ray shows hammer finger with avulsion of the tendon insertion; B. Post-operative X-ray shows secure fixation with suture anchors and Kirschner wires.
(4) Complications
Complications include permanent hammer finger deformity, secondary swan neck deformity (Figure 24-8), and traumatic arthritis of the distal interphalangeal joint due to joint mismatch or palmar subluxation.
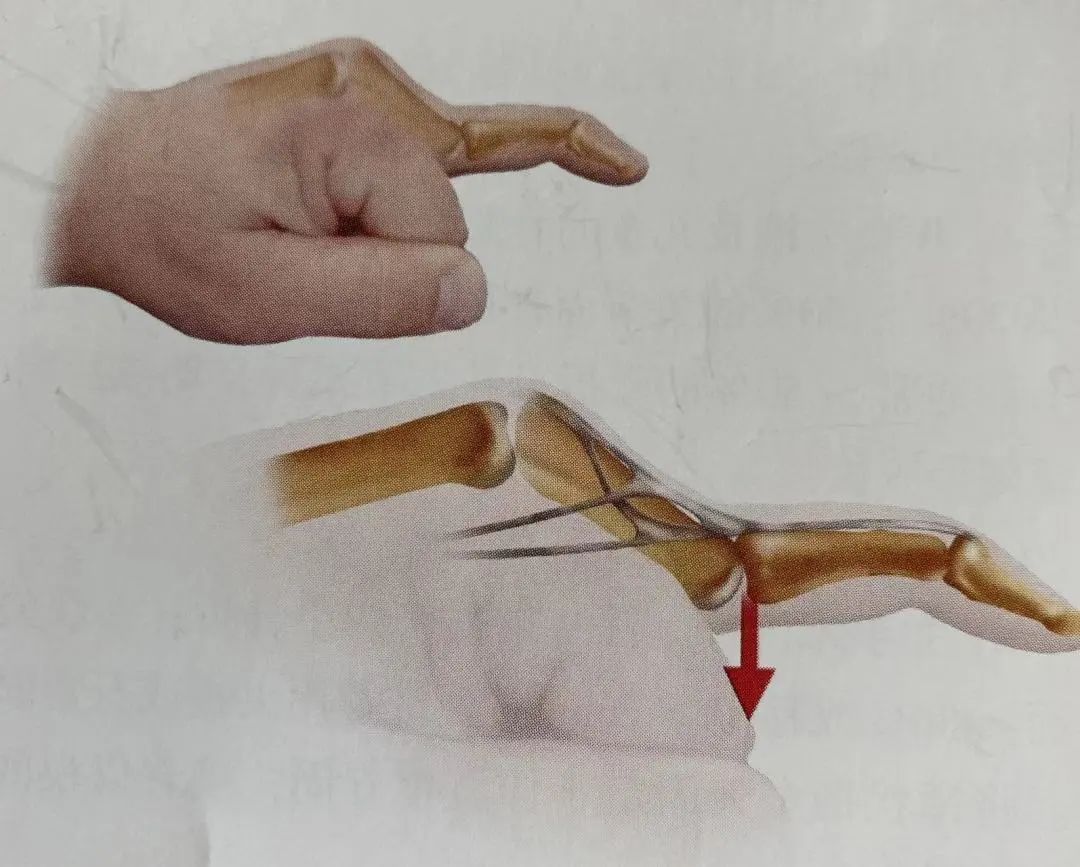
Figure 24-8: Swan neck deformity: lateral band subluxation.
Hyperextension force applied to the fingertip can cause rupture of the palmar plate and collateral ligaments, while the deep tendons remain intact. Due to the skin being tightly bound to the underlying bone, these injuries often accompany tears of the palmar soft tissue (in 64% of cases).
(1) Assessment
-
Clinical examination: The distal interphalangeal joint may have tenderness and deformity. The patient cannot flex or extend the joint.
-
Imaging examination: Anteroposterior and lateral X-rays should be taken before manual reduction. Dislocation is usually dorsal, rarely lateral. Whether there are associated avulsion fractures should be clarified.
(2) Classification
Includes closed dislocation, open dislocation, and fracture dislocation.
(3) Treatment
-
Closed reduction: Gentle closed reduction should be performed under digital block anesthesia. After traction on the distal phalanx, the joint is reduced over the condyle. Although the tendency for re-dislocation is small, the stability of the reduction should be reassessed after reduction. Post-reduction X-rays can confirm joint reduction without associated fractures. Short-term fixation (10-14 days) is usually sufficient. Thorough irrigation and debridement should be performed for open injuries before reduction.
-
Surgical treatment: Entrapment of the palmar plate, deep flexor tendon entrapment, or displaced osteochondral fracture fragments can lead to irreducible distal interphalangeal joint dislocation. In these cases, it is necessary to perform open reduction to release the trapped palmar plate, sesamoid bones, or fracture fragments. Entrapment of deep tendons means that at least one collateral ligament has ruptured, and in this case, fixation should last for 3 weeks.
(4) Complications
Include post-traumatic stiffness, recurrent instability, traumatic arthritis, and infection (septic arthritis and osteomyelitis).
Abduction or adduction forces applied to an extended finger can cause tearing of the radial or ulnar collateral ligaments of the PIP joint. Radial collateral ligament injuries are more common than ulnar collateral ligament injuries.
(1) Diagnosis
Clinical examination may reveal a distinct point of tenderness at the injury site. Ligament ruptures usually occur at the level of the proximal phalanx and are relatively rare in the middle of the ligament. Stress tests should be performed with the joint in extension or flexion at 20°. Lack of a firm endpoint can diagnose a complete tear. Anteroposterior stress X-rays showing an angle >20° can also diagnose a complete tear. Small fracture fragments may be seen at the origin of the collateral ligaments. Digital photographs can facilitate inspection.
(2) Treatment
-
Non-surgical treatment: Partial tears and most complete tears can be managed with static splinting for 7-14 days, followed by taping to the adjacent fingers for 3 weeks. Active motion is encouraged from the outset. Deep scarring often leads to joint discomfort and thickening of the collateral ligaments, which may last 3-6 months.
-
Surgical treatment: Surgical indications include imaging evidence of soft tissue entrapment, displaced phalanx fractures, and persistent instability after 3 weeks of static splinting. Surgery is necessary for the radial collateral ligament of the index finger to restore the strength of the collateral ligament.
PIP joint hyperextension injuries may lead to tearing of the palmar plate from the middle phalanx, with or without fracture fragments.
(1) Diagnosis
-
Clinical examination: The proximal interphalangeal joint may show fusiform swelling with a distinct point of tenderness over the palmar plate.
-
Imaging examination: Lateral X-rays may show small avulsion fracture fragments at the base of the middle phalanx, usually less than 10% of the joint surface. The proximal interphalangeal joint is usually reduced without subluxation.
(2) Treatment
Closed treatment is indicated. Stable injuries are fixed in a dorsal splint at 20° flexion for 1 week, followed by active joint movement under tape protection.
(3) Complications
Include post-traumatic flexion contracture, pain, and limited range of motion, and late swan neck deformity.
Dorsal dislocation of the PIP joint is one of the most common joint injuries of the hand. Hyperextension of the PIP joint causes the fingers to dislocate dorsally, resulting in dorsal dislocation of the middle phalanx, involving the proximal phalanx, and tearing the palmar plate.
(1) Diagnosis
-
Clinical examination: Dislocation usually results in a noticeable deformity of the finger unless it has been reduced by a coach or bystanders. Hyperextension stress tests are used to determine residual instability. Simple dorsal dislocation may indicate stability of the collateral ligaments.
-
Imaging examination: X-rays show dislocation of the proximal interphalangeal joint (Figure 24-9). A small avulsion fracture fragment may be seen from the middle phalanx, distinguishing the distal position of the palmar plate.
(2) Treatment
Longitudinal traction closed reduction is performed under digital nerve block anesthesia. Most dorsal dislocations are relatively easy to reduce. For stable reductions, active flexion and extension activities can begin early under tape protection. Lasting 3-6 weeks. Unstable injuries may require extended splinting for 3 weeks to prevent the last 20° of extension. If the palmar fracture fragment involves more than 15% of the joint surface, surgical intervention is necessary. Open dislocations should be thoroughly irrigated in the operating room, and if necessary, the original skin wound may be extended. Rotational deformities of the fingers may indicate entrapment of the middle phalanx between the lateral bands and central slip. This situation is often irreducible by closed traction and requires open reduction and repair of the extensor structure.
(3) Complications
Include post-traumatic flexion contracture, wide gap deformity, and hyperextension instability.
Entrapment of the central slip after injury may lead to entrapment at the proximal phalanx.
(1) Diagnosis
-
Clinical examination: Deformity and limited motion are usually evident. If the joint has spontaneously reduced, resistance to active extension of the middle phalanx suggests rupture of the central slip. If the lateral bands or central slip are trapped beneath the proximal phalanx, irreducible dislocation may occur.
-
Imaging examination: X-rays may show palmar dislocation of the proximal interphalangeal joint (see Figure 24-9). A small avulsion fracture may be seen on the dorsal side of the middle phalanx, caused by tearing and trapping of the central slip.
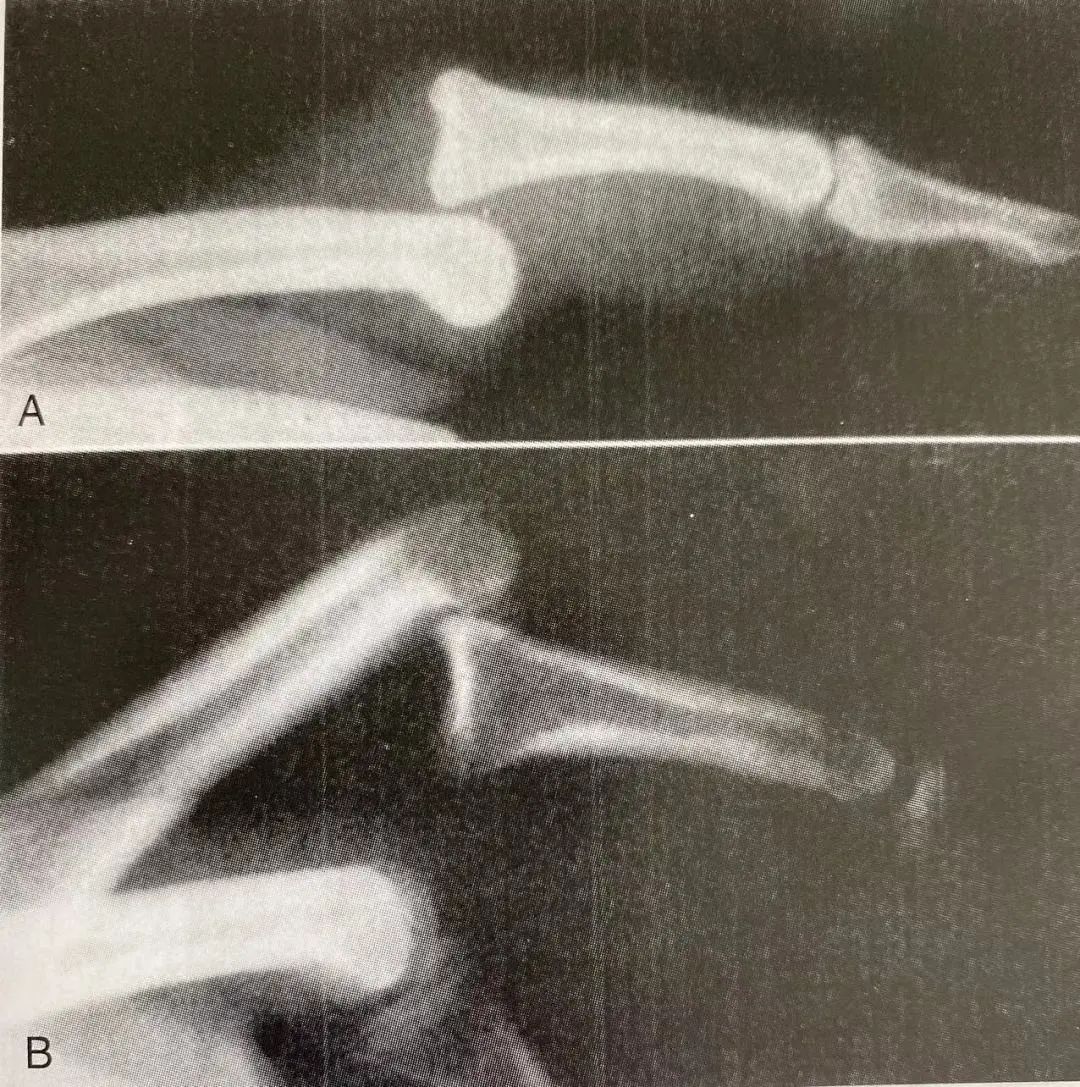 Figure 24-9: Proximal interphalangeal joint dislocation.
Figure 24-9: Proximal interphalangeal joint dislocation.
A. Dorsal dislocation (most common) can often be reduced closed, treated with tape. If the reduction is lost during extension, dorsal blocking splinting is needed; B. Palmar dislocation (rare) requires surgical repair of the extensor tendon central slip.
(2) Treatment
Longitudinal traction and flexion of the MCP and PIP joints may be attempted for closed reduction. After reduction, test the stability and strength of the central slip. If the central slip is intact, limited range of motion functional exercises can be performed after a short period of splinting. Rupture of the central slip must be fixed in the extended position with a static splint for 6 weeks or undergo open surgical repair of the damaged central slip apparatus.
(3) Complications
Include extension contracture, stiffness of the PIP or DIP joints, and progressive boutonniere deformity. Missed diagnosis of central slip rupture can lead to progressive extension structure damage and palmar dislocation, resulting in boutonniere deformity (Figure 24-10). Overall instability is another complication.

Figure 24-10: Damage to the central slip, if untreated, can lead to lateral band displacement and boutonniere deformity. Palmar dislocation of the proximal interphalangeal joint, though rare, can also lead to central slip damage. As long as the patient can actively extend the proximal interphalangeal joint within 30° of full extension, a splint can be used to fix the proximal interphalangeal joint (excluding the distal interphalangeal joint) in the extended position and encourage passive flexion of the distal interphalangeal joint, which is the correct method for treating acute central slip injuries.
Hyperextension, compression, and shear forces may lead to pilon fracture dislocation. These injuries are the most disabling PIP joint injuries.
(1) Diagnosis
-
Clinical examination: Swelling, pain, and limited motion may be observed, often without severe deformity. This injury is often misdiagnosed as a sprain.
-
Imaging examination: X-rays are essential for assessment. Lateral X-rays centered on the injured joint may show intra-articular fracture fragments. The size of the bone fragments varies from a small piece to up to 50% of the joint surface, depending on the severity of the dorsal subluxation of the middle phalanx. Lateral X-rays of the proximal interphalangeal joint in flexion can help to assess the likelihood of re-dislocation.
(2) Treatment
Effective treatment methods include dorsal extension splinting, bone traction, open reduction and internal fixation, and palmar plate repair.
-
Closed reduction treatment: Flexion-stable PIP joints can be treated with dorsal extension splints. Active flexion is allowed, and gradual extension activities are permitted after 4 weeks. Fracture fragments occupying less than 30% of the joint surface are also very suitable for this approach.
-
Surgical treatment: ① Open reduction and internal fixation: Large fracture fragments involving more than 50% of the joint surface can be surgically repaired using pull-out wires, Kirschner wires, or compression screws. Pilon fractures with joint surface compression require elevation and bone grafting with Kirschner pin fixation.
② Palmar plate repair: Comminuted fractures require removal of palmar bone fragments, with the palmar plate advanced to the middle phalanx to regain stability and reshape the damaged joint surface.
③ Bone traction: For severely comminuted fractures, there may be no other choice but to maintain longitudinal traction until the fracture heals.
④ Complications: Include recurrent dislocation, limited joint motion (in the hinged motion of the subluxated proximal interphalangeal joint), and post-traumatic arthritis.
Ulnar collateral ligament injury of the thumb MCP joint is also known as skier’s thumb or gamekeeper’s thumb. The strong ulnar collateral ligament of the MCP joint is crucial for effective lateral pinch grip.
(1) Assessment
-
Clinical examination: Tenderness may be palpable on the ulnar side of the MCP joint. If there is significant swelling, it may indicate a Stener lesion (entrapment of the adductor pollicis tendon between the torn ends of the ulnar collateral ligament and the proximal phalanx). Stress testing of the ulnar collateral ligament should be compared with the contralateral thumb. Testing the intrinsic collateral ligament is performed in slight flexion, while the palmar collateral ligament is tested in extension. If laxity is noted at both flexion and extension, a complete tear of the ligament and joint instability can be confirmed. Digital radiography should be performed prior to clinical examination.
-
Imaging examination: X-rays of the thumb should be taken before stress testing to check for associated fractures. Stress position X-rays showing an opening of the MCP joint >35° indicate complete tear of the ligament (Figure 24-11).
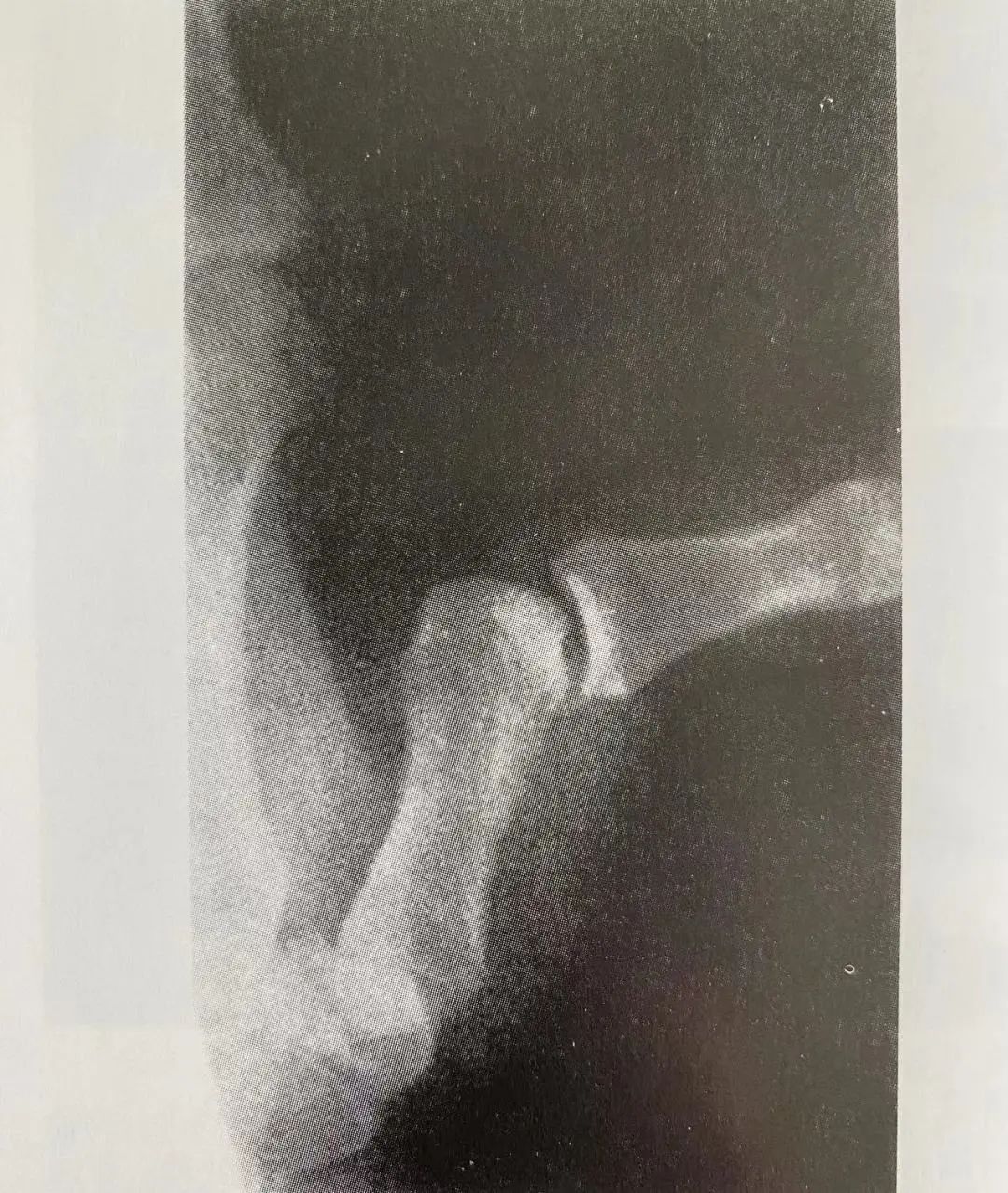
Figure 24-11: Stress testing of the ulnar collateral ligament of the first MCP joint shows significant radial deviation of the thumb as shown in this stress position X-ray.
(2) Treatment
-
Non-surgical treatment: Partial tears of the ulnar collateral ligament with intact endpoints and stress testing opening <35° can be treated with casting or functional splinting to maintain slight flexion of the MCP joint for 3-4 weeks.
-
Surgical treatment: Complete tears of the ulnar collateral ligament associated with MCP joint instability (stress testing opening >35°) or displaced fracture fragments require surgical reattachment of the ulnar collateral ligament. In these cases, a Stener lesion is often present, and non-surgical treatment will not heal to the proximal phalanx. Surgical repair of the ligament can be achieved using suture anchors or pull-out wires. Chronic ulnar collateral ligament injuries require ligament reconstruction or advancement of the adductor pollicis tendon to the proximal phalanx.
(3) Complications
Include residual instability with associated pain, weakness of lateral pinch strength, palmar subluxation of the MCP joint, and late changes of arthritis.
Radial collateral ligament injury of the thumb MCP joint is less common. However, it is often missed, leading to delayed treatment.
(1) Assessment
-
Clinical examination: Swelling and tenderness may be palpable on the radial side of the thumb MCP joint. Stress testing may elicit pain or confirm radial opening of the joint. Palmar subluxation is often associated with radial collateral ligament injury of the thumb MCP joint.
-
Imaging examination: X-rays of the thumb in two positions are used to assess associated fractures. Small osteochondral fracture fragments from the metacarpal may often be visible.
(2) Treatment
-
Casting: Almost all radial collateral ligament injuries, once diagnosed, require tubular casting or thumb spica splinting for 4-6 weeks. Tubular casting is necessary to prevent palmar subluxation of the MCP joint.
-
Surgical treatment: If the MCP joint is unstable or there is palmar subluxation, surgical repair of the radial collateral ligament is necessary. The ligament usually ruptures from the metacarpal head and needs to be repaired with suture anchors or pull-out wires.
(3) Complications
Similar to those listed for ulnar collateral ligament injury of the thumb MCP joint.
Force applied to the finger can lead to injury of the radial or ulnar collateral ligaments of the metacarpophalangeal joint. The collateral ligaments of the metacarpophalangeal joint usually rupture at the attachment point on the proximal phalanx, sometimes including an avulsion fracture fragment.
(1) Diagnosis
-
Clinical examination: Mild swelling may be visible between the metacarpal heads. Local tenderness may confirm the site of injury. Gentle stress testing of the metacarpophalangeal joint may elicit pain or demonstrate instability in extension or flexion.
-
Imaging examination: X-rays may show small avulsion fragments from the metacarpal head.
(2) Treatment
-
Non-surgical treatment: Most finger collateral ligament injuries can be managed non-surgically. Taping of the fingers is recommended to protect the collateral ligaments of the MCP joint, and intermittent splinting of the metacarpophalangeal joint in a flexed position of more than 50° may be used for unstable injuries. Symptoms may slowly improve over more than 3 months.
-
Surgical treatment: Surgical treatment is indicated for avulsion fractures involving more than 20% of the joint surface or displacement >2mm. Relative indications for surgical repair include radial collateral ligament injury of the index or little finger.
(3) Complications
Include instability, laxity, weakness, or pain. Chronic pain and secondary adhesions are more common sequelae than instability, hence the recommendation to use static splints for no more than 3 weeks. Extension contractures may also occur.
MCP joint dislocation most commonly occurs in dorsal dislocation, particularly in the index finger, thumb, and little finger. Dorsal dislocation may be simple (reducible) or complex (irreducible).
(1) Assessment
-
Simple dislocation: The metacarpophalangeal joint is visibly hyperextended with a noticeable deformity. X-rays show the proximal phalanx in a hyperextended position of 60°-90° over the metacarpal head.
-
Complex dislocation (Figure 24-12): Deformity may not be obvious, and the joint is only slightly hyperextended. A common finding is skin indentation (wrinkle) at the distal transverse crease. X-rays show the proximal phalanx and metacarpal bones aligned parallel. If a sesamoid bone appears in the widened metacarpophalangeal joint space, it indicates entrapment.
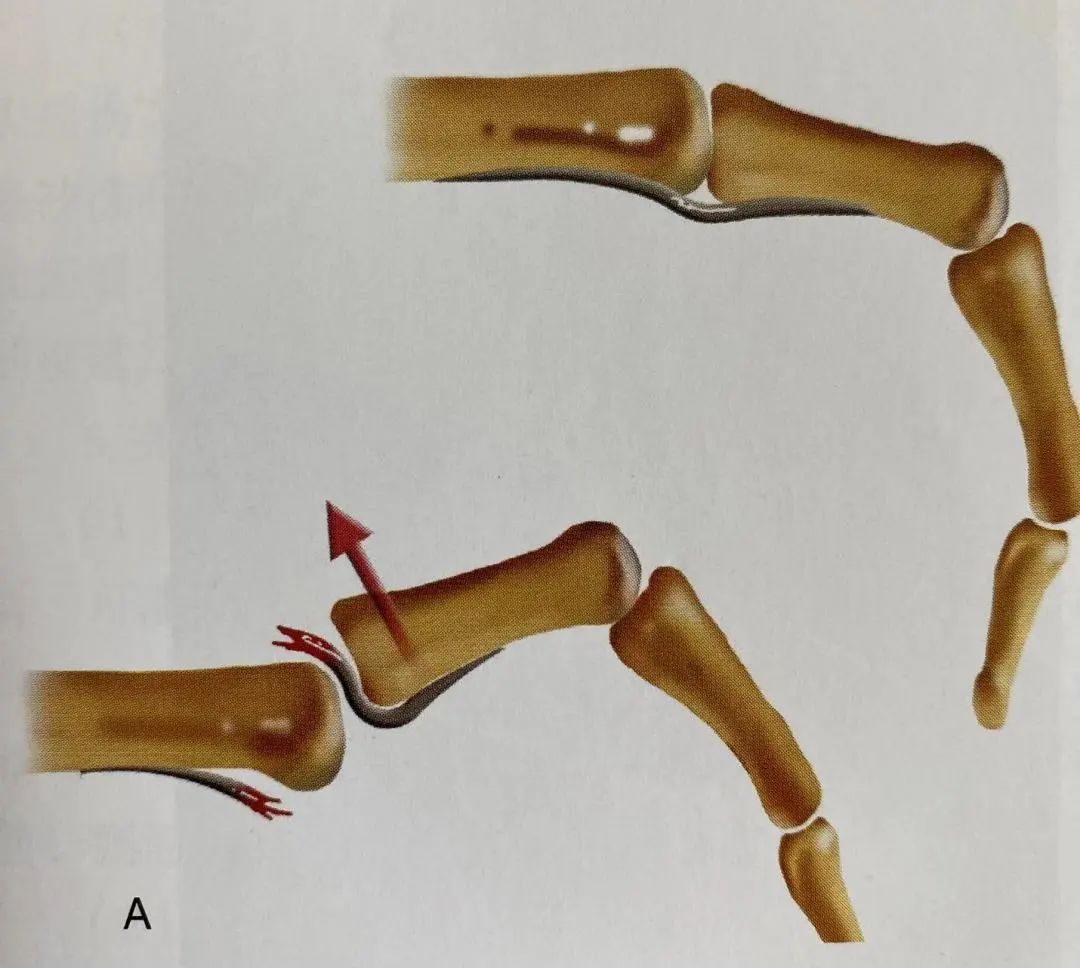
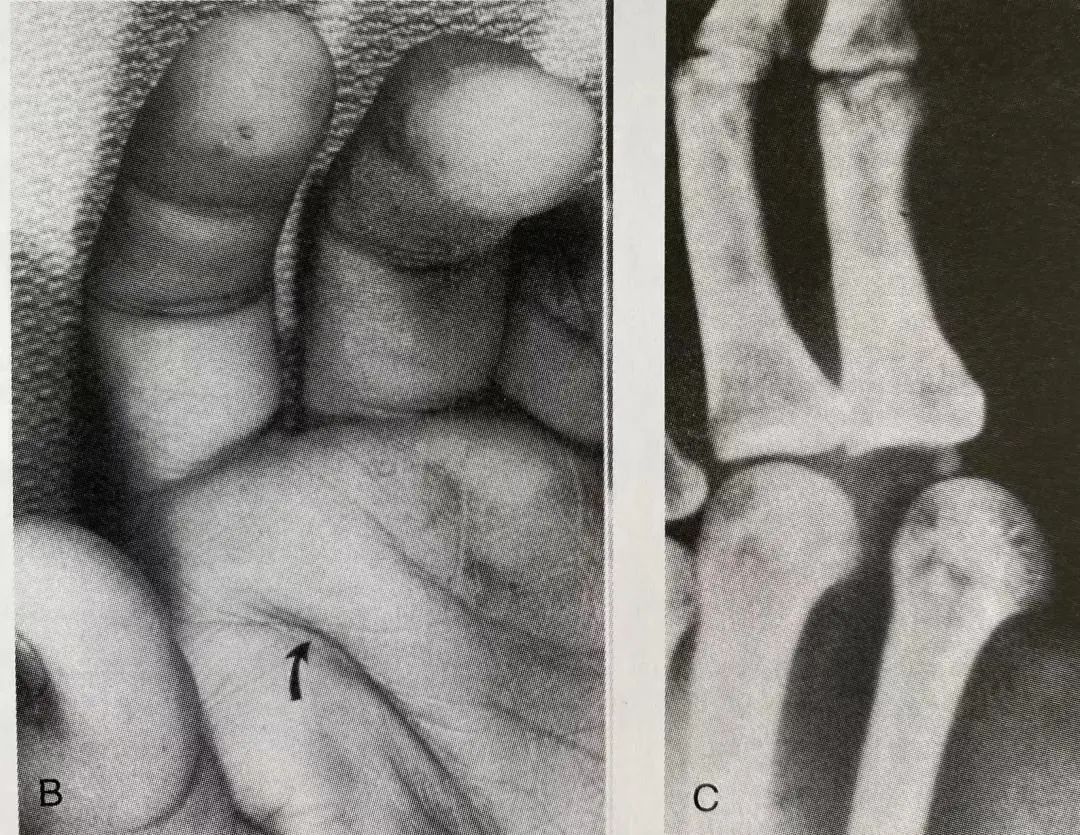
Figure 24-12: Complex dorsal dislocation of the metacarpophalangeal joint.
Illustration shows how the palmar plate displaces dorsally, blocking the dorsal dislocation of the metacarpophalangeal joint; B clinical photos show the skin wrinkles of the hand (arrow): C. X-ray shows the sesamoid bone trapped in the widened metacarpophalangeal joint space.
(2) Treatment
-
Simple dislocation: Gentle closed reduction should be performed by hyperextending the metacarpophalangeal joint and then pushing the proximal phalanx forward over the metacarpal head. Direct longitudinal traction should be avoided as it may convert a simple dislocation into a complex one.
-
Complex dislocation: Closed reduction may be attempted once, but the most complex dislocations require open reduction in the operating room. Open reduction can be achieved through dorsal or palmar approaches, and it may be necessary to release the trapped palmar plate. In the palmar approach, the radial digital nerve may cross over the metacarpal head of the index finger, or the ulnar digital nerve may cross over the metacarpal head of the little finger. If necessary, the palmar plate may be longitudinally incised to assist in joint reduction. The dorsal approach may avoid fractures. After reduction, the MCP joint is usually stable, allowing for active flexion and extension exercises under tape protection.
(3) Complications
May include digital nerve injury, joint stiffness, and arthritis (if associated with metacarpal head fractures).
The second, third, and fourth carpometacarpal joints are stable joints that allow only slight gliding motion, classified as micro-motion joints. The fifth carpometacarpal joint has greater mobility, resembling the first carpometacarpal joint. As a saddle joint, the fifth carpometacarpal joint allows both gliding and rotational movements to facilitate thumb movement. The stability of the carpometacarpal joint is maintained by strong intermetacarpal ligaments and ligaments such as the carpometacarpal ligaments. Fracture dislocation of the carpometacarpal joint requires significant force. Dislocation generally occurs dorsally (unless the force acts directly from the dorsal side, causing palmar dislocation of the carpometacarpal joint). Palmar dislocation is less common than dorsal dislocation, but due to the increased mobility of the fifth carpometacarpal joint, palmar dislocation is relatively common in the fifth carpometacarpal joint.
1. Assessment
Due to the overlapping bone structures of the carpometacarpal joint, X-ray assessment of injuries is very difficult. Various angles of X-rays are needed to accurately understand the injury. X-rays may show subluxation or dislocation of the carpometacarpal joint (with or without associated fracture fragments involving the CMC joint surface) (Figure 24-13). Computed tomography (CT) may reveal more difficult diagnostic issues. A 30° pronated view of the hand may be necessary to assess the alignment of the joint surfaces.
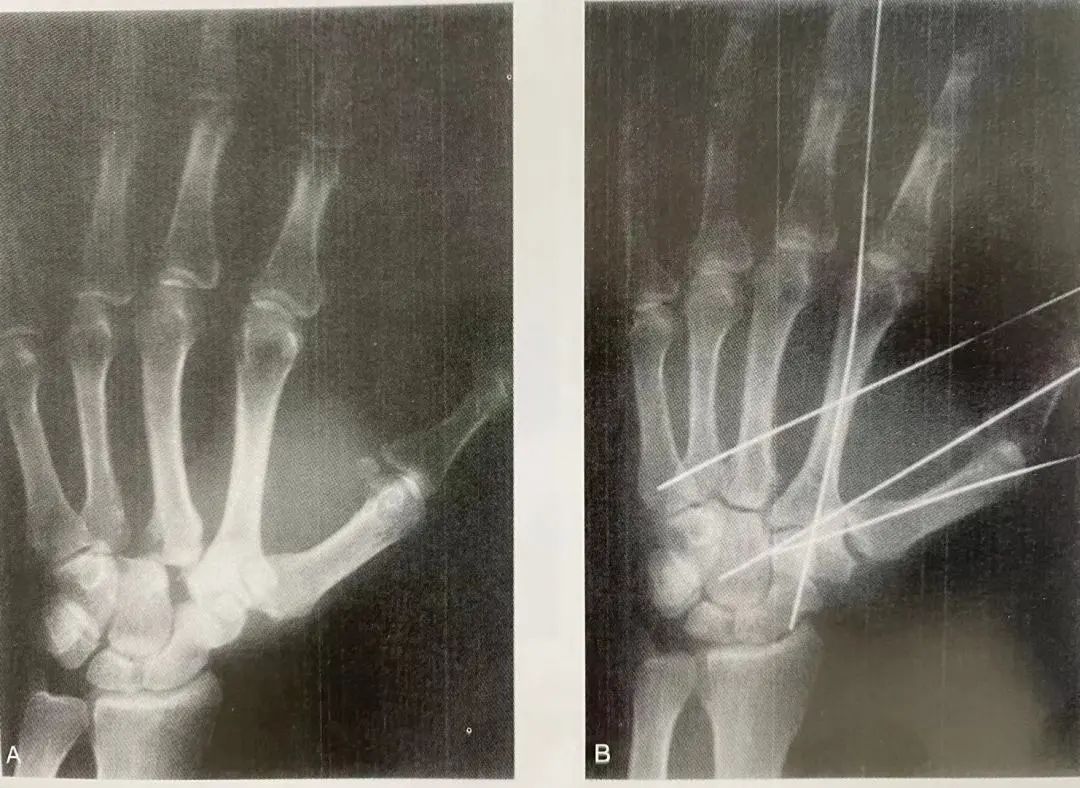
Figure 24-13 A. X-ray shows dislocation of the second and third carpometacarpal joints at the injury site; B. Post-reduction X-ray shows the dislocation reduced and fixed with Kirschner wires.
2. Treatment
Closed reduction is generally easier under longitudinal traction, but simple casting cannot maintain the reduction. In addition to casting, percutaneous Kirschner wire fixation is often necessary. Re-dislocation or incomplete reduction often occurs in the second and fifth carpometacarpal joints, resulting from the pull of the radial extensor and ulnar extensor tendons on the metacarpals. Because these injuries are associated with instability and significant swelling, casting after closed reduction often leads to recurrence.
3. Complications
Include re-dislocation, pain, weakness, and arthritis. Traumatic arthritis of the CMC joint can be effectively treated with arthrodesis.
Source: “Essentials of Trauma Orthopedics”, represents the author’s personal view, does not represent the official position of Bone Today. Hope everyone can make rational judgments and apply them purposefully.