
Forum Introduction: Claude syndrome was first described by French neurologist Claude in 1912, also known as red nucleus syndrome. The main symptoms are ipsilateral oculomotor nerve paralysis and contralateral ataxia. Oculomotor nerve paralysis may include pupil dilation and restricted eye movement, describing the anatomical localization, namely the red nucleus, oculomotor nerve bundle, and superior cerebellar peduncle. This syndrome is a special type of midbrain infarction that can easily delay treatment.
The patient, a 55-year-old female, was admitted on 2017-07-17 due to “double vision and unstable walking for 6 days, left eyelid drooping for 5 days.” Six days prior, the patient experienced double vision at rest without obvious cause, which became more pronounced when looking left, along with unstable walking, easily leaning to the right, requiring assistance, and reduced mobility in the right hand. There was no significant dizziness, rotational vision, limb numbness, twitching, or speech disorders, and bowel and bladder functions were normal. On the second day of onset, she visited a local county hospital, underwent a CT scan of the head and cardiac ultrasound, which showed no significant abnormalities. One day later, left eyelid drooping occurred, and the local hospital initially diagnosed it as “oculomotor nerve paralysis,” providing unspecified treatment, with no improvement in her condition, leading to her transfer to our hospital on the sixth day of onset. The patient had a 10-year history of hypertension, taking nifedipine tablets, 1 tablet/day, and a history of “stroke,” denying diabetes or heart disease history.
Admission examination: Blood pressure 122/76 mmHg, alert and articulate, cognitive function normal, left eyelid drooping, left pupil 4 mm, sluggish light reflex, right pupil 3 mm, sensitive light reflex, limited adduction, upward, and downward movement of the left eye, unrestricted movement of the left eye in all directions, normal muscle strength and tone in limbs, symmetrical bilateral limb and facial sensations, negative bilateral pathological signs; right-side finger-to-nose and heel-to-shin tests inaccurate, positive Romberg test; meningeal irritation signs negative. Auxiliary examination: triglycerides 3.36 mmol/L, homocysteine 16 mmol/L, other biochemical indices and blood routine basically normal. Neck vascular ultrasound showed: bilateral carotid intima thickening with plaque formation; head MRI + DWI + MRA (2017-07-15 Figure 1): (1) new cerebral infarction in the midbrain; residual changes of bleeding in bilateral basal ganglia, thalamus, and pons; (2) bilateral periventricular white matter demyelination changes; (3) brain MRA showed left middle cerebral artery M1 segment sclerosis and reduced distal branches; bilateral posterior cerebral arteries thin and signal reduced.
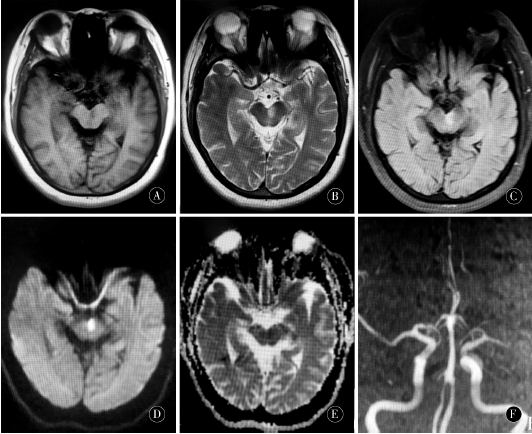 Figure 1A-C: Left midbrain medial long T1 long T2 highFLAIR abnormal signal; D: DWI shows high signal in the left midbrain; E:ADC shows low signal in the left midbrain; F: MRA shows left middle cerebral artery M1 segment sclerosis and reduced distal branches; bilateral posterior cerebral arteries thin and signal reduced (head MRI + DWI + MRA on the seventh day of onset)
After admission, treatment was given to inhibit platelet aggregation, stabilize plaques, improve circulation, eliminate oxygen free radicals, regulate blood pressure, and control blood lipids. After 10 days of treatment, the patient’s eye movement improved compared to before but had not returned to normal levels. The left eyelid drooping slightly improved, and the right-side ataxia improved, allowing her to eat and walk independently. After improvement, she was discharged.
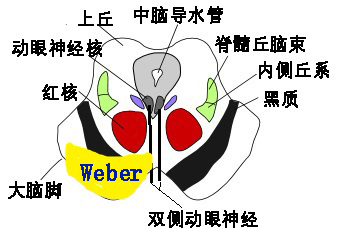
The oculomotor nerve nuclei located in the midbrain tegmentum are distributed rather scattered. The root fibers of these nuclei travel ventrally with parasympathetic fibers, some transversely passing through the red nucleus, ultimately forming the oculomotor nerve exiting the brainstem on both sides from the interpeduncular fossa. The afferent impulses of the red nucleus come from the cerebellar emboliform and dentate nuclei, and the cerebellar red nucleus bundle crosses within the superior cerebellar peduncle in the midbrain, participating in the regulation of body posture and assisting in the precise and smooth execution of voluntary movements. Near the level of the superior colliculus of the midbrain aqueduct, tumors, inflammation, and vascular lesions can cause ipsilateral oculomotor nerve fiber bundles and superior cerebellar peduncle efferent fibers to be affected, thus presenting a group of symptoms including ipsilateral oculomotor nerve paralysis and contralateral cerebellar ataxia.
This syndrome is rare, and since its first report, there have only been a few case reports both domestically and internationally, with differing opinions on the location of the responsible lesion. KREMER initially described Claude syndrome as involving the red nucleus. DHANJAL and others conducted pathological examinations on a case of Claude syndrome, showing pericentral midbrain infarction affecting part of the superior cerebellar peduncle and red nucleus, while MRI showed no lesions in the red nucleus, indicating that Claude syndrome does not necessarily involve the red nucleus. However, it should be noted that MRI findings may not fully correspond to the areas affected in neuropathology. SEO et al. studied 6 cases of Claude syndrome patients, and CHIN-SHIH et al. studied 1 case of Claude syndrome through imaging and pathological studies, finding that the anatomical localization of this syndrome primarily involves the superior cerebellar peduncle, with only mild involvement of the red nucleus aside from the oculomotor nerve bundle.
The midbrain paramedian artery is one of several branches of the posterior cerebral artery, supplying the midbrain paramedian area, including the medial side of the crus cerebri, red nucleus, substantia nigra, superior cerebellar peduncle, oculomotor nerve nucleus, and nerve roots. The midbrain paramedian artery is a small terminal artery, and these branches are easily obstructed by microatheromatous emboli or cardiogenic emboli, which can also cause hypoperfusion ischemic damage. The narrowing of the posterior cerebral artery is considered a potential factor for these patients. Routine vascular imaging such as head MRA and CTA often fails to detect this, while DSA can clearly identify the presence of this vessel but is an invasive examination and not a routine examination method, thus often relying on the ischemic area to infer vascular lesions.
The patient’s head MRA showed left middle cerebral artery M1 segment sclerosis and reduced distal branches; bilateral posterior cerebral arteries were thin and signal reduced. No abnormalities were found in the cardiac ultrasound, considering that the onset was related to midbrain supply artery atherosclerosis thrombosis or arterial stenosis caused by hypertension. Pure midbrain infarction accounts for 0.6% of ischemic strokes, and ataxia is the most common clinical manifestation of midbrain infarction, possibly due to the presence of abundant nerve fiber bundles connecting the cerebellum. Oculomotor nerve paralysis has been recognized as a clinical feature of midbrain infarction, but it occurs only in 35% of pure midbrain infarctions, and patients with concurrent pupil dilation are less likely to occur, indicating that only a small proportion involve all oculomotor nerve nuclei and nerve bundles. Therefore, sudden onset of oculomotor nerve paralysis and ataxia should be taken seriously for potential stroke. The patient suddenly developed left eyelid drooping, inability to adduct the left eye, and upward and downward gaze, with pupil dilation indicating complete oculomotor nerve paralysis, damage to the oculomotor nerve bundle, and simultaneous right-side ataxia, easily leaning to the right, indicating damage to the cerebellar connecting fibers, possibly affecting the cerebellar red nucleus bundle and red nucleus. On the seventh day of onset, the patient underwent head MRI + DWI + MRA, suggesting a new lesion in the left midbrain anterior medial region, with atherosclerotic basis in the carotid and cerebral arteries. Considering the patient was a middle-aged female with acute onset, a history of hypertension, and stroke, it can be clearly localized as midbrain infarction. This case did not present contralateral limb tremors, rigidity, or involuntary movements, thus differing from Benedict syndrome (red nucleus syndrome), representing a more typical Claude syndrome.
The patient visited a local county hospital on the second day, underwent head MRI but not DWI, and no significant lesions were found. The primary care hospital made an unclear diagnosis, leading to treatment delays. Isolated oculomotor nerve paralysis with pupil dilation is most commonly caused by diabetes or microvascular disease leading to ischemia of cranial nerves. Most oculomotor nerve paralysis is peripheral damage. For patients with risk factors for stroke such as hypertension, diabetes, and stroke history, if sudden unilateral oculomotor nerve paralysis occurs, it is essential to carefully check for other neurological signs, such as concurrent contralateral cerebellar ataxia, and consider midbrain infarction and the possibility of Claude syndrome. Timely completion of head MRI examination, especially DWI, is crucial for early diagnosis and treatment, enabling the best recovery for the patient.
Figure 1A-C: Left midbrain medial long T1 long T2 highFLAIR abnormal signal; D: DWI shows high signal in the left midbrain; E:ADC shows low signal in the left midbrain; F: MRA shows left middle cerebral artery M1 segment sclerosis and reduced distal branches; bilateral posterior cerebral arteries thin and signal reduced (head MRI + DWI + MRA on the seventh day of onset)
After admission, treatment was given to inhibit platelet aggregation, stabilize plaques, improve circulation, eliminate oxygen free radicals, regulate blood pressure, and control blood lipids. After 10 days of treatment, the patient’s eye movement improved compared to before but had not returned to normal levels. The left eyelid drooping slightly improved, and the right-side ataxia improved, allowing her to eat and walk independently. After improvement, she was discharged.
The oculomotor nerve nuclei located in the midbrain tegmentum are distributed rather scattered. The root fibers of these nuclei travel ventrally with parasympathetic fibers, some transversely passing through the red nucleus, ultimately forming the oculomotor nerve exiting the brainstem on both sides from the interpeduncular fossa. The afferent impulses of the red nucleus come from the cerebellar emboliform and dentate nuclei, and the cerebellar red nucleus bundle crosses within the superior cerebellar peduncle in the midbrain, participating in the regulation of body posture and assisting in the precise and smooth execution of voluntary movements. Near the level of the superior colliculus of the midbrain aqueduct, tumors, inflammation, and vascular lesions can cause ipsilateral oculomotor nerve fiber bundles and superior cerebellar peduncle efferent fibers to be affected, thus presenting a group of symptoms including ipsilateral oculomotor nerve paralysis and contralateral cerebellar ataxia.
This syndrome is rare, and since its first report, there have only been a few case reports both domestically and internationally, with differing opinions on the location of the responsible lesion. KREMER initially described Claude syndrome as involving the red nucleus. DHANJAL and others conducted pathological examinations on a case of Claude syndrome, showing pericentral midbrain infarction affecting part of the superior cerebellar peduncle and red nucleus, while MRI showed no lesions in the red nucleus, indicating that Claude syndrome does not necessarily involve the red nucleus. However, it should be noted that MRI findings may not fully correspond to the areas affected in neuropathology. SEO et al. studied 6 cases of Claude syndrome patients, and CHIN-SHIH et al. studied 1 case of Claude syndrome through imaging and pathological studies, finding that the anatomical localization of this syndrome primarily involves the superior cerebellar peduncle, with only mild involvement of the red nucleus aside from the oculomotor nerve bundle.
The midbrain paramedian artery is one of several branches of the posterior cerebral artery, supplying the midbrain paramedian area, including the medial side of the crus cerebri, red nucleus, substantia nigra, superior cerebellar peduncle, oculomotor nerve nucleus, and nerve roots. The midbrain paramedian artery is a small terminal artery, and these branches are easily obstructed by microatheromatous emboli or cardiogenic emboli, which can also cause hypoperfusion ischemic damage. The narrowing of the posterior cerebral artery is considered a potential factor for these patients. Routine vascular imaging such as head MRA and CTA often fails to detect this, while DSA can clearly identify the presence of this vessel but is an invasive examination and not a routine examination method, thus often relying on the ischemic area to infer vascular lesions.
The patient’s head MRA showed left middle cerebral artery M1 segment sclerosis and reduced distal branches; bilateral posterior cerebral arteries were thin and signal reduced. No abnormalities were found in the cardiac ultrasound, considering that the onset was related to midbrain supply artery atherosclerosis thrombosis or arterial stenosis caused by hypertension. Pure midbrain infarction accounts for 0.6% of ischemic strokes, and ataxia is the most common clinical manifestation of midbrain infarction, possibly due to the presence of abundant nerve fiber bundles connecting the cerebellum. Oculomotor nerve paralysis has been recognized as a clinical feature of midbrain infarction, but it occurs only in 35% of pure midbrain infarctions, and patients with concurrent pupil dilation are less likely to occur, indicating that only a small proportion involve all oculomotor nerve nuclei and nerve bundles. Therefore, sudden onset of oculomotor nerve paralysis and ataxia should be taken seriously for potential stroke. The patient suddenly developed left eyelid drooping, inability to adduct the left eye, and upward and downward gaze, with pupil dilation indicating complete oculomotor nerve paralysis, damage to the oculomotor nerve bundle, and simultaneous right-side ataxia, easily leaning to the right, indicating damage to the cerebellar connecting fibers, possibly affecting the cerebellar red nucleus bundle and red nucleus. On the seventh day of onset, the patient underwent head MRI + DWI + MRA, suggesting a new lesion in the left midbrain anterior medial region, with atherosclerotic basis in the carotid and cerebral arteries. Considering the patient was a middle-aged female with acute onset, a history of hypertension, and stroke, it can be clearly localized as midbrain infarction. This case did not present contralateral limb tremors, rigidity, or involuntary movements, thus differing from Benedict syndrome (red nucleus syndrome), representing a more typical Claude syndrome.
The patient visited a local county hospital on the second day, underwent head MRI but not DWI, and no significant lesions were found. The primary care hospital made an unclear diagnosis, leading to treatment delays. Isolated oculomotor nerve paralysis with pupil dilation is most commonly caused by diabetes or microvascular disease leading to ischemia of cranial nerves. Most oculomotor nerve paralysis is peripheral damage. For patients with risk factors for stroke such as hypertension, diabetes, and stroke history, if sudden unilateral oculomotor nerve paralysis occurs, it is essential to carefully check for other neurological signs, such as concurrent contralateral cerebellar ataxia, and consider midbrain infarction and the possibility of Claude syndrome. Timely completion of head MRI examination, especially DWI, is crucial for early diagnosis and treatment, enabling the best recovery for the patient.
Source: Peng Xiaoxue, Bao Sujuan, Ma Xiaojun, Ge Zhaoming. A Case of Claude Syndrome and Literature Review [J]. Chinese Journal of Practical Neurology, 2018, 21(07):799-801.
More exciting readings
-
Year-End Review | 2023 Top Ten Scientific Research Advances in Parkinson’s Disease
-
Paradoxical Embolism
-
A Kaleidoscope of Neurological Diseases!
-
2023 Top Ten Scientific Research Advances in Sleep Medicine
-
Fast Walking or Slow Jogging | Individualized Scientific Exercise Prescription for Hypertension
-
Spinal Neurosarcoidosis
-
Lucid Dreaming | From Phenomenology to Cognitive Neuroscience
-
Precision Copper Removal and Individualized Treatment for Wilson’s Disease
-
Adolescent Depression Related to Sleep Deprivation
-
Psychological Talk | Lack of Security in Romantic Relationships
Latest Neuroscience Information Sharing Platform
Neurological Difficulties & Rare Disease Consultation Platform

This public account aims to disseminate cutting-edge information in neuroscience and explore clinical difficulties & rare diseases for public learning purposes! Original works are welcome for submission. Reproduced content and images are intended to convey more scientific information. If you do not wish to be reproduced, please contact us for deletion. Submission and contact email: [email protected]

