Authors: You Shanshan, Xu Zhonghui, Jiang Yuxin
Affiliation: Department of Ultrasound Medicine, Peking Union Medical College Hospital
Corresponding Author: Jiang Yuxin
Source: Journal of Peking Union Medical College
2017,8(4-5):215-220
Rheumatoid arthritis (RA) is an autoimmune disease of unknown etiology, commonly found in middle-aged women, with an incidence rate of approximately 0.32% to 0.36% in China[1]. Its main manifestations include symmetric, persistent joint swelling and tenderness, morning stiffness lasting more than 1 hour, with the most commonly affected joints being the proximal interphalangeal joint (PIP), metacarpophalangeal joint (MCP), wrist, and elbow. The pathological changes in RA include synovial cell hyperplasia, infiltration of various inflammatory cells, vascular granulation, invasion of cartilage and subchondral bone tissue, ligaments, and tendons, leading to destruction of articular cartilage, bone, and joint capsule, ultimately resulting in joint deformity and loss of function[1].
Currently, the imaging examinations used for joints mainly include X-ray films, magnetic resonance imaging (MRI), and musculoskeletal ultrasound (MSUS). X-ray films were once the gold standard for diagnosing RA joint damage and were listed as one of the revised diagnostic criteria for RA by the American College of Rheumatology (ACR) in 1987[2]. The Sharp scoring for narrowing of the joint space and the Larsen score for bone erosion are used to grade RA by X-ray. Although the specificity is high, the sensitivity is poor. X-ray cannot provide clear diagnostic evidence for pathological changes such as synovial hyperplasia, active synovitis, and vascular granulation, making X-ray suitable for observing mid to late-stage lesions and follow-up examinations for confirmed patients, but it cannot make an early diagnosis of RA. MRI is highly sensitive in displaying early RA lesions and is one of the reliable methods for early diagnosis, accurately assessing the disease course, and monitoring efficacy; however, it is expensive, relatively time-consuming, and not suitable for some claustrophobic patients. MSUS has advantages such as being non-invasive, cost-effective, free of ionizing radiation, and easy to operate, playing an increasingly important role in the early diagnosis of RA, assessment of disease activity, monitoring drug efficacy, and treatment[3-4].
In 2013, the European League Against Rheumatism published 10 recommendations for the application of joint imaging examinations in RA clinical practice, strongly recommending the use of MSUS for detecting subclinical disease, monitoring treatment response, and predicting disease progression[5]. Traditional MSUS techniques include grey-scale ultrasound (GSUS) and color Doppler imaging (CDFI), while contrast-enhanced ultrasonography (CEUS) and ultrasound-guided interventional therapy are rapidly developing new technologies. This article reviews the applications and research progress of these techniques in RA.
Application Of Grey-Scale Ultrasound In Rheumatoid Arthritis
Diagnosing Synovitis
The basic lesion of RA is synovitis, and ultrasound can differentiate synovial hyperplasia from effusion.
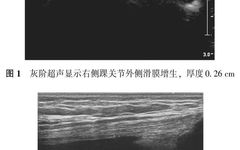
The ultrasound imaging definition of synovial hyperplasia by the Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) is an abnormal hypoechoic area within the joint (compared to subcutaneous fat, it can sometimes be isoechoic or hyperechoic), immovable and incompressible(Figure 1); the definition of synovial effusion is an abnormal hypoechoic area within the joint cavity (compared to subcutaneous fat, it can sometimes be isoechoic or hyperechoic), movable and compressible(Figure 2). The echo type of synovial hyperplasia varies greatly, from anechoic to hyperechoic, and the synovial morphology can range from mild synovial thickening to severe synovial hypertrophy with villi, deposits, and effusion. GSUS can be used to establish the diagnosis of RA, especially after ultrasound application, which can significantly improve diagnostic accuracy compared to traditional RA diagnostic methods such as clinical examination and X-ray examination[6].

The currently recognized semi-quantitative grading of synovial thickening by ultrasound is the grading methods proposed by Szkudlarek in 2003[7] and Dougados in 2010[8].
The grading standards proposed by Szkudlarek in 2003 are as follows:
Grade 0: No synovial thickening
Grade 1: Mild synovial thickening, not exceeding the line connecting the highest points of the bone surfaces
Grade 2: Synovial thickening exceeding the line connecting the highest points of the bone surfaces, but not exceeding the bone shaft
Grade 3: Synovial thickening exceeding the line connecting the highest points of the bone surfaces, and extending beyond one side of the bone shaft
In 2010, the Dougados grading method defined the grading levels as follows:
Grade 0: No synovial thickening
Grade 1: Mild synovial thickening
Grade 2: Moderate synovial thickening
Grade 3: Significant synovial thickening
However, the above grading systems also have flaws, including that certain normal small joints such as finger joints may also show grade 1-2 lesions, making it impossible to define normal values. There are differences between observers, and the degree of pressure applied by the probe may cause differences in results.
Diagnosing Bone Erosion
Bone erosion is a hallmark of pathological changes in RA, characterized by a destructive process of discontinuity of the bone cortex and associated mineral loss. De Flaviis[9] first applied MSUS to detect bone erosion in RA lesions in 1988. The classification standards for bone erosion vary widely among different studies, and OMERACT points out that bone defects must be seen in two mutually perpendicular planes to be diagnosed, defining those less than 2 mm in diameter as small bone erosions and those greater than 2 mm as large bone erosions[10]. Several studies have shown that MSUS can detect more bone erosions in the hands, feet, and shoulder joints compared to X-rays[11-12]. This is because MSUS can display the joint contour in three-dimensional space, while X-ray images are a two-dimensional display of the superimposed density of all structures along the path of the X-ray, thus many important details may be obscured. A comparative study of MSUS and X-ray in 100 RA patients showed that in the early stages of the disease, MSUS could detect bone erosions 6.5 times more than X-ray, and it has advantages when bone erosions are too small to be detected by X-ray; in the late stages of disease, the difference is 3.4 times[13]. Similarly, Weidekamm[14] found that in RA populations with other diseases, MSUS could detect bone erosions twice as much as X-ray. In RA, bone erosions within the joint tend to occur at specific locations, most commonly on the radial side of the second and third metacarpophalangeal joints and the fifth metatarsophalangeal joint, with the proximal interphalangeal joint most commonly affected medially and laterally. However, scholars like Zayat[15] believe that bone erosions detected by ultrasound are not highly specific for diagnosing RA, but the second and fifth metacarpophalangeal joints, the fifth metatarsophalangeal joint, and the distal ulnar joint are more specific for predicting RA.
Diagnosing Tendonitis and Tenosynovitis
In the inflammatory process of RA, inflammation and damage often affect the surrounding joints, particularly tendon damage can lead to significant functional impairment in RA patients[16]. It is often manifested as thickening of the tendon or tendon sheath visible in two mutually perpendicular planes, with reduced or uneven echo, and power Doppler ultrasound (PDUS) can detect Doppler signals. In 2014, the OMERACT MSUS group proposed a semi-quantitative scoring system for tendon damage in RA patients: Grade 0: Normal tendon; Grade 1: Partial tendon injury visible in both perpendicular planes; Grade 2: Complete tendon rupture visible in both perpendicular planes[17]. Janta et al.18 evaluated 72 RA patients’ four tendons (bilateral ulnar wrist extensors and bilateral tibialis posterior tendons) using GSUS, finding that the overall score was the sum of each tendon damage score, and that the tendon damage score was positively correlated with the RA disease course, with a high correlation with radiographic structural damage.
Application Of Doppler Ultrasound In Rheumatoid Arthritis Lesions
Diagnosing Synovitis
Doppler ultrasound includes CDFI and PDUS. PDUS detects blood flow signals mainly depending on the relative quantity of red blood cells with the same sampling flow speed, unaffected by factors such as the angle of ultrasound incidence, and can show blood flow even if the average speed of perfusion is zero. Since the blood vessels of proliferative synovium are mostly small vessels with low flow velocity, PDUS can detect blood flow signals in proliferative synovium more sensitively than CDFI(Figure 3).
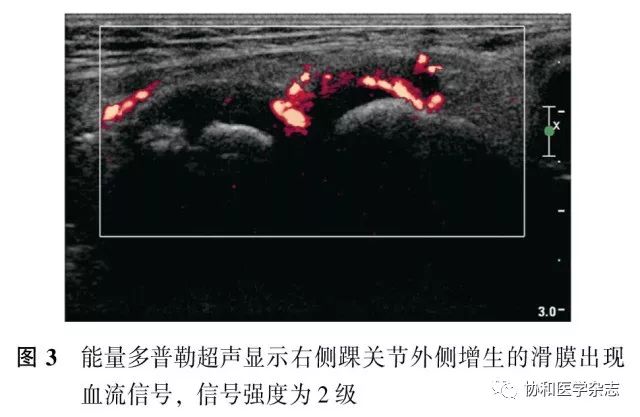
PDUS can semi-quantitatively grade the richness of blood flow signals, providing a more accurate assessment of joint inflammation and structural changes. However, there is currently no unified grading standard internationally. Newman et al.20 proposed a four-grade classification of synovitis based on PDUS signal intensity in 1996: Grade 0: No color blood flow signal; Grade 1: Single flow or mild blood flow signal; Grade 2: Multiple blood flow signals or moderate blood flow; Grade 3: Merged blood flow signals covering the entire synovium or strong blood flow signal. Schueller-Weidekamm21 proposed a four-grade classification of PDUS signals in 2009: Grade 0: Normal, i.e., no blood flow signal; Grade 1: Mild synovitis, i.e., punctate blood flow signal; Grade 2: Moderate synovitis, i.e., multiple punctate or merged blood flow; Grade 3: Severe synovitis, i.e., multiple merged blood flow covering more than half of the synovium. Kamishima et al.22 proposed a four-grade classification of PDUS signals in 2010: Grade 0: No blood flow signal; Grade 1: Punctate blood flow signal; Grade 2: Blood flow signal covering less than 1/3 of the joint cavity; Grade 3: Blood flow signal covering 1/3 to 2/3 of the joint cavity; Grade 4: Blood flow signal covering more than 2/3 of the joint cavity.
Some researchers have used computer-assisted measurements of color pixels and Doppler curve resistance index to analyze synovial blood vessels, and to quantitatively measure color pixels, the operator needs to define the region of interest related to the size of the joint cavity. Snekhalatha et al.23 used computer software to extract the color score algorithm of the wrist and MCP joints of RA patients, finding that the color score of the MCP3 joint was significantly elevated, indicating rich blood flow signals in that area, suggesting the presence of RA inflammation activity, and that the color score algorithm was significantly correlated with standard parameters such as health-related quality of life scores, 28-joint Disease Activity Score (DAS28), and erythrocyte sedimentation rate, thus this method can be used for quantitative diagnosis and evaluation of RA patients’ wrist and MCP joints.
Monitoring Disease Activity And Drug Efficacy
Kawashiri et al.24 believe that patients with synovitis showing blood flow signals on PDUS are more likely to develop bone erosions than those without blood flow signals, and that PDUS blood flow signal measurements are not correlated with clinical serum markers. Minowa et al.25 compared RA patients who were serum positive and negative using GSUS and PDUS and found that ultrasound was more helpful in diagnosing the former. Mian et al.26 found that RA patients with intermittent fibromyalgia may have higher disease activity scores, depression, and limb dysfunction scores, but both GSUS and PDUS showed characteristics of mild synovitis, suggesting that the recognition and management strategies for such patients may need to be adjusted. Naredo et al.27 found that in RA patients in persistent remission, PDUS could detect blood flow signals that could predict the failure of biological agent therapy. Domestic scholars such as Li Qiang et al.28 divided 48 RA patients into remission and non-remission groups according to different clinical remission standards and conducted ultrasound examinations on them, finding that there was no significant improvement in ultrasound disease activity between the two groups, with 79% of patients in the remission group still exhibiting GSUS or PDUS activity, thus a comprehensive assessment of disease activity status using clinical physical examinations and imaging indices such as ultrasound can help achieve true strict control and slow disease progression.
Predicting Disease Relapse
Janta et al.29 conducted ultrasound evaluations on 47 RA patients treated with methotrexate at the start of treatment and after 6 months and found that GSUS synovial thickening in the wrist joint, MCP, and PDUS blood flow signals in the wrist joint, ankle joint, MCP, and metatarsophalangeal joints were predictors of unstable remission. Sreerangaiah et al.30 evaluated 85 RA patients with a disease course of less than 3 months using PDUS and X-ray, finding that 3D power Doppler volume and 2D Doppler scores were ultrasound predictors of structural damage, and quantitative evaluation of vascular PDUS could benefit serum-positive early RA patients. Zufferey et al.31 showed that ultrasound-detected synovitis could not only predict RA progression but also predict the progression of inflammatory arthropathy associated with polyarthralgia and anti-citrullinated protein antibody negativity.
Application Of Contrast-Enhanced Ultrasound In Rheumatoid Arthritis Lesions
Although CDFI and PDUS can display synovial blood vessels, they cannot show small capillaries with low flow rates. Microvascular imaging in RA requires more sensitive vascular imaging techniques. Ultrasound contrast agents are suspensions containing microbubbles, typically with diameters less than 8 μm, which can distribute throughout the capillary networks of various organs in the body and serve as blood pool tracers, rarely leaking into synovial effusions, thus providing a more accurate reflection of vascular changes in the target tissue[32]. They can display the microvascular structure of solid tissues and calculate local concentrations over time, allowing for quantitative analysis of synovial vasculature.
In 2003, the International Arthritis Contrast Ultrasound Study Group (IACUS) conducted a multicenter study using GSUS, PDUS, and CEUS to evaluate synovial thickening in 113 RA patients, showing that MSUS and PDMSUS could identify 60.1% of active and inactive synovial thickening, while CEUS could distinguish 97.3% of active synovial thickening from inactive synovial thickening, significantly improving diagnostic efficacy[33]. Klauser et al.34 evaluated the vascularity of tendon synovitis in the wrist joints of 26 patients using PDUS and CEUS, showing that CEUS detected more vessels around and within tendons than PDUS, making CEUS more sensitive; however, there was no correlation between synovial thickening and the degree of vascular formation. Klauser et al.35 in 2011 compared subjective grading of CEUS and PDUS with computer-assisted objective quantitative scoring of CEUS in 37 patients’ joint synovial vasculature, finding that computer-assisted CEUS correlated with subjective CEUS grading, and that the intensity ratio of contrast signals correlated with subjective grading of PDUS and CEUS, with no correlation between clinical disease activity and neoangiogenesis or synovial thickening.
Interventional Diagnosis And Treatment Of Rheumatoid Arthritis Under Ultrasound Guidance
Interventional treatments guided by MSUS include fluid aspiration, intra-articular and peri-articular injection therapy, and synovial biopsy.
Fluid aspiration can relieve intra-articular pressure and alleviate pain, and the aspirated fluid can be used for further study. During ultrasound-guided aspiration, the needle tip position can be monitored in real-time to determine whether the puncture is successful and whether there is residual fluid, and it can detect very small amounts of fluid in the joint cavity; a small amount of saline can be injected into the joint cavity before re-aspiration for analysis[36].
Ultrasound-guided local corticosteroid injection is a relatively simple and cost-effective treatment method that can serve as an alternative or adjunctive treatment for several rheumatic diseases[37]. The purpose of corticosteroid injection is to reduce inflammatory responses. Babaei-Ghazani et al.[38] injected fluocinolone acetonide into a resistant cyst around the shoulder and elbow joints of a 26-year-old RA patient, resulting in significant relief of shoulder pain and hand numbness, with complete absorption of the cyst after 12 months.
AmmitzbØll-Danielsen et al.[39] randomly divided 55 RA patients with tendonitis into two groups using a double-blind method, with Group A receiving intramuscular injection of betamethasone and ultrasound-guided intra-articular injection of saline, while Group B received intramuscular injection of saline and ultrasound-guided intra-articular injection of betamethasone. Follow-ups at 4 and 12 weeks found that Group B performed better than Group A.
Synovial biopsy can enhance the understanding of the pathogenesis of RA, help discover potential targeted therapeutic drugs, and evaluate responses to antirheumatic drug therapy. Currently, there are three methods for synovial biopsy: blind needle biopsy, ultrasound-guided biopsy, and arthroscopic biopsy. Kelly et al.[40] performed ultrasound-guided synovial biopsy on 57 cases of early arthritis involving the knee, elbow, wrist, MCP, and PIP joints, with the obtained synovial tissue used for immunohistochemistry and RNA extraction, showing that ultrasound-guided synovial biopsy is a safe and well-tolerated method, with high GSUS scores for synovitis being predictive of high-quality or quantity of synovial tissue and RNA.
As MSUS continues to be widely and deeply researched globally, it will play an increasingly important role in the early diagnosis of RA, monitoring disease progression, predicting disease relapse, and guiding the determination of clinical treatment plans, as well as in ultrasound-guided local treatment injections in joint cavities.
References Omitted
Author Introduction:

–
You Shanshan
–
Master of Medicine, Associate Chief Physician of the Department of Ultrasound Medicine, Peking Union Medical College Hospital. With over ten years of clinical experience, proficient in ultrasound diagnostic techniques for common and difficult diseases in abdominal, obstetric, vascular, and superficial organs. One of the first medical talents in the “team-based” assistance program for Tibet, awarded the “Special Contribution Award for Assistance to Tibet” by Peking Union Medical College Hospital, and appointed as a lifelong visiting professor by the People’s Hospital of Tibet Autonomous Region. Author of 10 Chinese papers and 1 English paper as the first author.


Journal of Peking Union Medical College
Welcome to the official website
Follow the cover solicitation
Click for submission information
Official Website (Submission System)
http://mjpumch.cbpt.cnki.net
Magazine Subscription
Postal code for nationwide distribution: 2-719
Contact Us
Peking Union Medical College Hospital, No. 1 Shuai Fu Yuan, Beijing
Phone: 010-69154261/4262

Click “Read the original text” to download the literature for free