|
|
Gastric adenocarcinoma accounts for approximately 95% of gastric malignancies, predominantly occurring in individuals over 50 years of age. It exhibits low sensitivity to chemotherapy and radiotherapy, resulting in high incidence and mortality rates, with overall poor prognosis [1]. The disease typically presents no symptoms in its early stages; as it progresses, patients may experience gastric discomfort, dyspepsia, and non-specific abdominal pain, necessitating effective and accurate screening methods [2]. Clinically, the diagnosis and assessment of gastric adenocarcinoma primarily rely on imaging examinations and pathological biopsies, which provide some reference value, but there is a lack of research on the mechanisms of occurrence and progression of gastric adenocarcinoma. With the continuous advancement of serum testing technologies, it has been discovered that serum markers such as fatty acid binding protein 4 (FABP4), alpha-fetoprotein (AFP), and monocyte chemotactic protein-1 (MCP-1) show abnormal expression in malignant tumor patients, which can assist physicians in evaluating the patient’s condition [3]. This study analyzed 43 gastric adenocarcinoma patients and 40 healthy individuals, aiming to explore the changes in serum levels of FABP4, AFP, and MCP-1 in gastric adenocarcinoma patients and their clinical significance.
1 Materials and Methods
1.1 Inclusion and Exclusion Criteria
Inclusion criteria: ① Patients who meet the diagnostic criteria for gastric adenocarcinoma [4], confirmed by pathological biopsy; ② Patients who are conscious and have stable vital signs; ③ Patients who can cooperate with examinations. Exclusion criteria: ① Patients with other malignant tumors; ② Patients with other gastric diseases; ③ Patients with acute or chronic infections, severe endocrine diseases, autoimmune diseases, or hematological diseases; ④ Patients with liver or kidney dysfunction; ⑤ Patients who received radiotherapy or chemotherapy before the study commenced.
1.2 General Information
Forty-three gastric adenocarcinoma patients admitted to a certain hospital between August 2022 and July 2023 were selected as the observation group, including 25 males and 18 females; ages ranged from 38 to 79 years, with an average age of (60.35±7.11) years. An additional 40 healthy individuals who underwent physical examinations during the same period were selected as the control group, excluding those with severe organ dysfunction, mental disorders, or immune system diseases, including 23 males and 17 females; ages ranged from 40 to 78 years, with an average age of (59.63±7.23) years. There was no statistically significant difference in general information between the two groups (P>0.05), indicating comparability. This study was approved by the hospital’s medical ethics committee, and informed consent was obtained from the participants.
1.3 Methods
3 mL of venous blood was drawn from the subjects (on an empty stomach in the morning), centrifuged at 3500 r/min for 15 minutes with a centrifuge radius of 10 cm, and the supernatant was separated and stored at -80℃ until testing; serum levels of FABP4 (enzyme-linked immunosorbent assay), AFP (chemiluminescence method), and MCP-1 (enzyme-linked immunosorbent assay) were measured.
The TNM staging of gastric cancer was determined according to the American Joint Committee on Cancer (AJCC) guidelines, classified into stages I, II, III, and IV.
Medical records were reviewed, and information on patient age, gender, tumor diameter, TNM stage, differentiation degree, and tumor location was collected, and relevant data were organized and input into statistical software for analysis.
Quality control during the study period was strengthened, actively correcting problems and defects; all collected blood samples were sent to the hospital laboratory for testing within 1 hour, first tested by one group of personnel, then retested by another group, and the results were analyzed collectively. Once there was no disagreement, data entry began, using a double-entry method with two people independently entering data, followed by consistency checks to promptly address anomalies, ensuring data accuracy.
1.4 Statistical Methods
SPSS 25.0 statistical software was used for analysis. Measurement data were described using  t test was used for comparison, and count data were described using rates, analyzed using the χ2 test. Correlations were analyzed using Spearman correlation analysis, and influencing factors were analyzed using univariate and multivariate logistic regression analysis. The predictive value was assessed by plotting receiver operating characteristic curves (ROC), with P<0.05 indicating statistical significance.
t test was used for comparison, and count data were described using rates, analyzed using the χ2 test. Correlations were analyzed using Spearman correlation analysis, and influencing factors were analyzed using univariate and multivariate logistic regression analysis. The predictive value was assessed by plotting receiver operating characteristic curves (ROC), with P<0.05 indicating statistical significance.
2 Results
2.1 Comparison of Serum Levels of FABP4, AFP, and MCP-1 Between the Two Groups
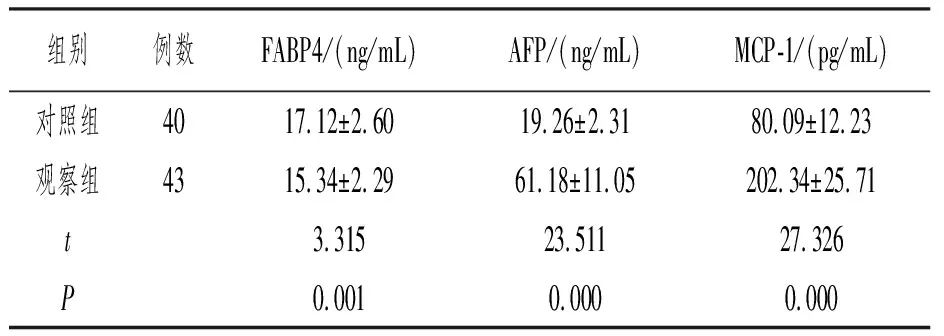
Compared to the control group, the observation group had lower FABP4 levels (P<0.05) and higher AFP and MCP-1 levels (P<0.05). See Table 1.
Table 1 Comparison of Serum Levels of FABP4, AFP, and MCP-1 Between the Two Groups 
2.2 Comparison of Serum Levels of FABP4, AFP, and MCP-1 in Patients with Different Tumor Diameters
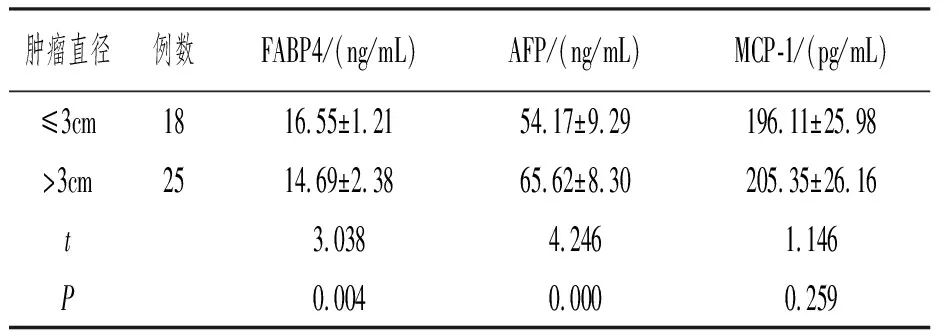
Compared to patients with tumor diameter ≤3 cm, those with tumor diameter >3 cm had lower FABP4 levels (P<0.05) and higher AFP levels (P<0.05); there was no statistically significant difference in MCP-1 levels among different tumor diameters (P>0.05). See Table 2.
Table 2 Comparison of Serum Levels of FABP4, AFP, and MCP-1 in Patients with Different Tumor Diameters 
2.3 Correlation Between FABP4, AFP, and MCP-1
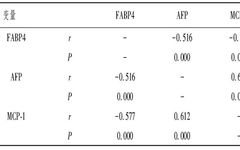
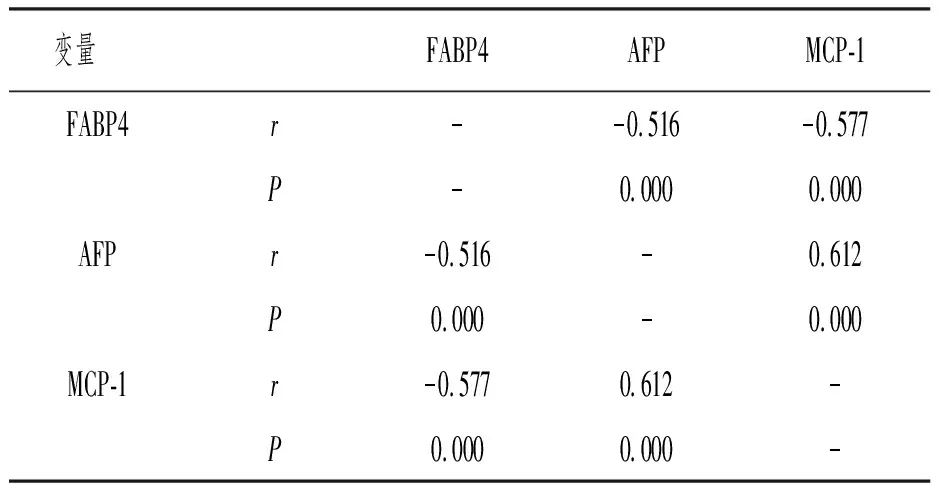
Spearman correlation analysis showed that FABP4 was negatively correlated with AFP, FABP4 was negatively correlated with MCP-1, and AFP was positively correlated with MCP-1 (P all <0.05). See Table 3.
Table 3 Correlation Between FABP4, AFP, and MCP-1
2.4 Univariate Analysis of Gastric Adenocarcinoma Progression
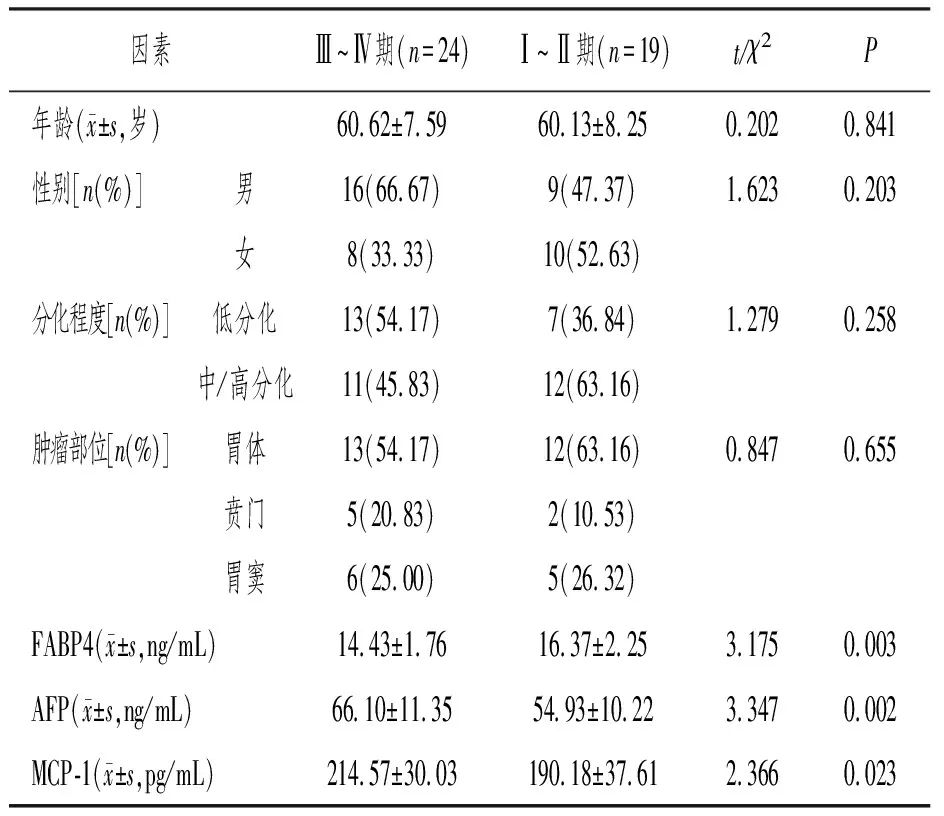
In the comparison of age, gender, differentiation degree, and tumor location between stages I–II and III–IV, there was no statistically significant difference (P>0.05); compared with the stage I–II group, the stage III–IV group had lower FABP4 levels (P<0.05) and higher AFP and MCP-1 levels (P<0.05). See Table 4.
Table 4 Univariate Analysis of Gastric Adenocarcinoma Progression
2.5 Multivariate Logistic Regression Analysis of Gastric Adenocarcinoma Progression
Factors with statistical differences from univariate analysis were used as independent variables, and the progression degree was used as the dependent variable for assignment, as shown in Table 5. A multivariate logistic regression model was established, finding that AFP (OR=2.165) and MCP-1 (OR=1.832) were independent risk factors affecting gastric adenocarcinoma progression (P<0.05), while FABP4 (OR=0.729) was a protective factor (P<0.05). See Table 6.
Table 5 Variable Assignment Table
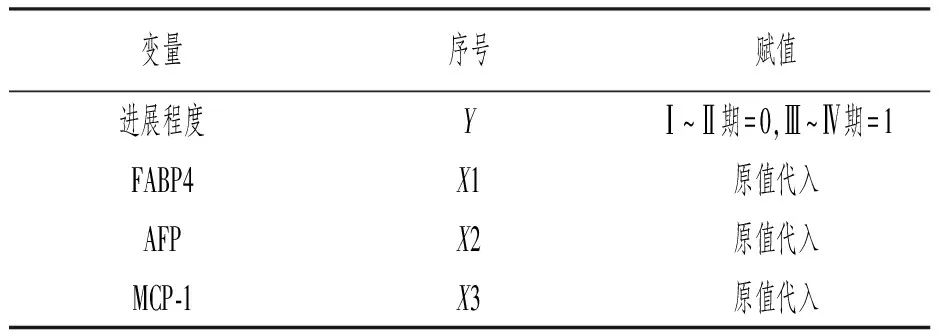
Table 6 Multivariate Logistic Regression Analysis of Gastric Adenocarcinoma Progression

2.6 Predictive Value of Serum Levels of FABP4, AFP, and MCP-1 for Gastric Adenocarcinoma Progression
ROC curve analysis showed that the area under the curve (AUC) for predicting gastric adenocarcinoma progression using FABP4, AFP, MCP-1, FABP4+AFP, FABP4+MCP-1, AFP+MCP-1, and combined detection were 0.739, 0.774, 0.711, 0.828, 0.860, 0.846, and 0.965, respectively. See Table 7, Figure 1.
Table 7 Predictive Value of Serum Levels of FABP4, AFP, and MCP-1 for Gastric Adenocarcinoma Progression
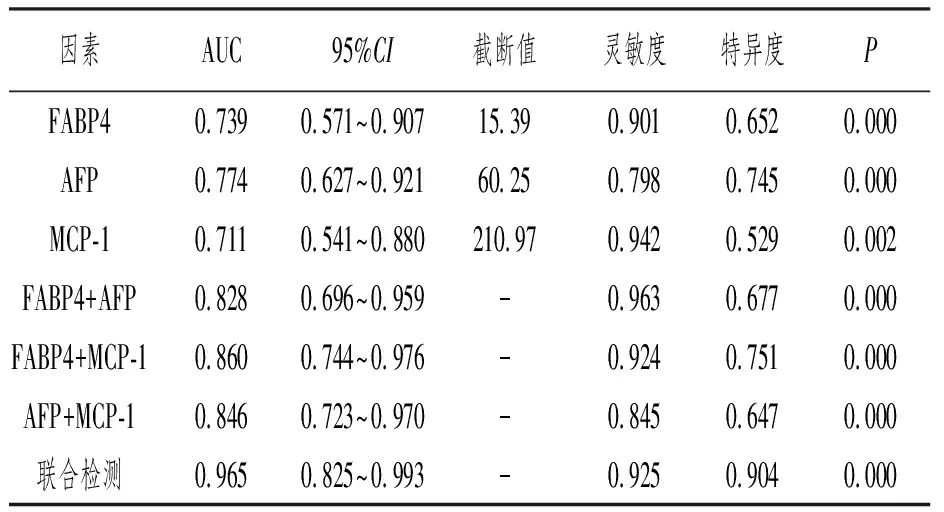
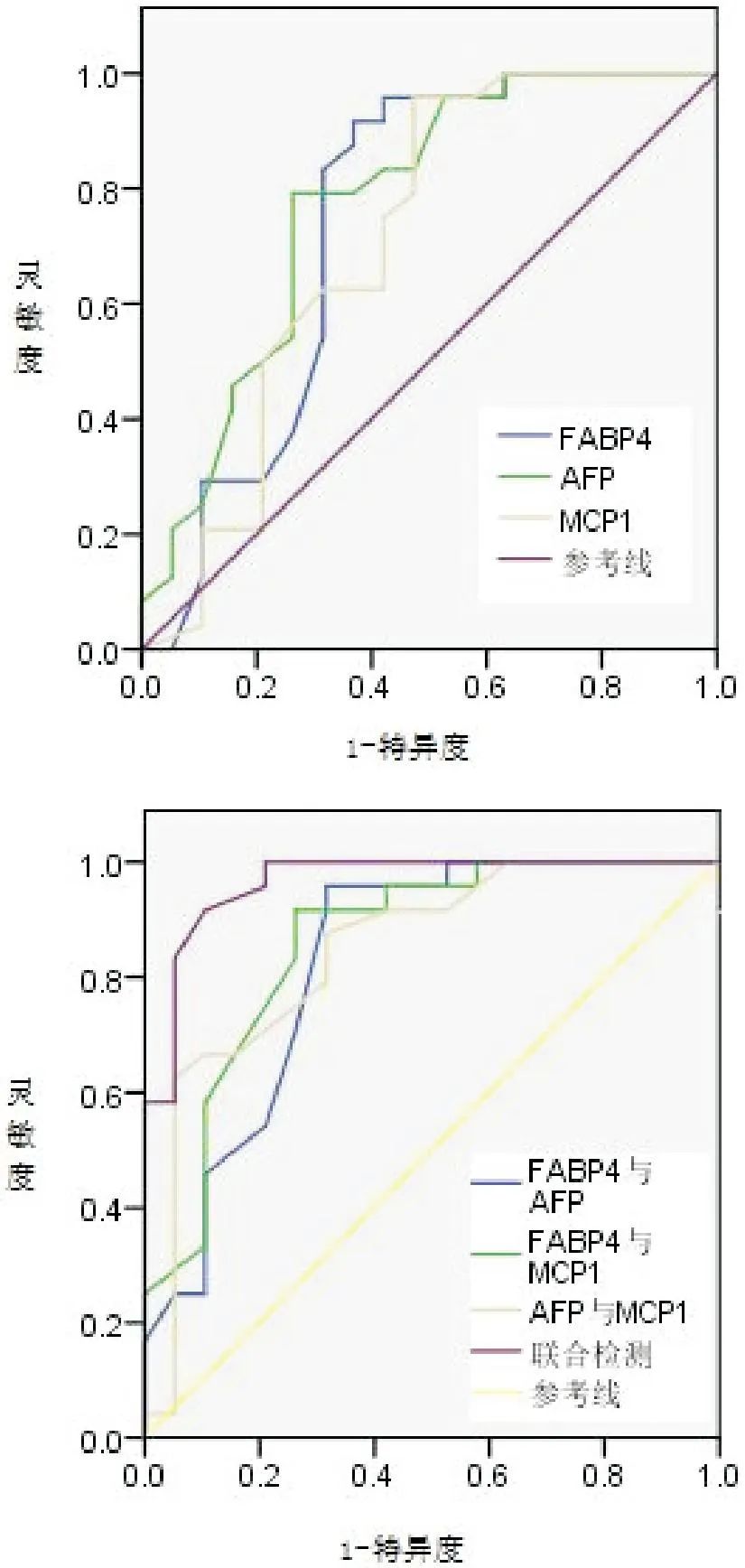
Figure 1 ROC Curve for Predicting Gastric Adenocarcinoma Progression Based on Serum Levels of FABP4, AFP, and MCP-1
3 Discussion
Gastric adenocarcinoma arises from the malignant transformation of gastric gland cells, which can grow in the gastric wall and invade adjacent tissues and organs, easily entering the lymphatic system and causing lymph node metastasis, even leading to distant metastasis, further shortening the patient’s survival [5]. Due to the lack of specific symptoms in the early stages of the disease, most patients are diagnosed at advanced stages, missing the optimal timing for surgical treatment and having a poor prognosis. Early diagnosis and targeted treatment measures are beneficial for controlling the progression of the disease [6].
FABP4 is a lipid chaperone protein that regulates the uptake and transport of fatty acids, influences systemic glucose metabolism, and facilitates communication between energy storage systems and organs in response to life-threatening situations [7]. This substance can regulate cell adhesion molecule 3 (CADM3), enhancing intercellular adhesion ability and inhibiting cancer cell shedding and metastasis. AFP, as a single-chain glycoprotein, has functions such as transport, immune suppression, and bidirectional regulation of growth factors, and is considered associated with primary tumors, showing high expression in various tumors [8]. MCP-1 belongs to the CC chemokine family and can influence the body’s inflammatory response and tumor immunity, inducing the secretion of matrix metalloproteinases, promoting the destruction and remodeling of the extracellular matrix, creating conditions for cancer cell metastasis [9].
Liu Li et al. [10] suggested that FABP4 exhibits low expression in the serum of patients and is closely related to poor prognosis, making it a novel diagnostic target and biomarker for gastric adenocarcinoma. Kong Junfeng et al. [11] pointed out in their study that serum AFP has high diagnostic value for gastric cancer, with serum AFP levels in gastric cancer patients being higher than those in non-gastric cancer patients. In this study, the observation group had lower FABP4 levels compared to the control group, and higher AFP and MCP-1 levels; patients with tumor diameter >3 cm had lower FABP4 levels and higher AFP levels compared to those with tumor diameter ≤3 cm. Considering the reasons, FABP4 can affect the adhesion, proliferation, and invasion of gastric adenocarcinoma cells and influence the occurrence and development of gastric adenocarcinoma through lipid metabolism and bile acid binding regulation, making it a potential diagnostic target; serum AFP levels are significantly elevated due to abnormal proliferation of gastric mucosal gland cells [12]; MCP-1 can induce inflammatory responses, stimulating gastric gland cells and leading to cellular carcinogenesis. In the results of this study, Spearman correlation analysis showed that FABP4 was negatively correlated with AFP (r=-0.516), FABP4 was negatively correlated with MCP-1 (r=-0.577), and AFP was positively correlated with MCP-1 (r=0.612). FABP4 can influence the metabolism and functioning of triglycerides, induce apoptosis in gastric adenocarcinoma cells, and slow down the tumor growth and progression rate in patients, with FABP4 significantly downregulated in gastric adenocarcinoma patients; high expression of AFP can regulate cell proliferation and metabolism, inhibiting the body’s immune response to gastric adenocarcinoma cells; if AFP is highly expressed, the proliferation capacity of cancer cells in the patient is strong, and the malignancy degree is high; MCP-1 can stimulate tumor neovascularization through various pathways, creating favorable conditions for the growth and proliferation of gastric adenocarcinoma cells, promoting disease progression in patients.
In this study, FABP4, AFP, and MCP-1 can predict the progression of gastric adenocarcinoma. ① FABP4 (OR=0.729): High expression of FABP4 can promote intercellular adhesion of gastric adenocarcinoma cells, preventing them from detaching from the primary lesions, thus inhibiting their migration and invasion, thereby suppressing the progression of gastric adenocarcinoma [13]. ② AFP (OR=2.165): Luo Dongming et al. [14] indicated in their study that serum AFP can be used to predict lymph node metastasis in gastric cancer patients; compared to patients without metastasis, those with lymph node metastasis have significantly elevated serum AFP levels. High expression of AFP enhances the invasion ability of gastric adenocarcinoma cells to lymphatic endothelial cells and leads to abnormal differentiation and maturation of gastric gland cells, facilitating the spread and metastasis of gastric adenocarcinoma cells. ③ MCP-1 (OR=1.832): MCP-1 can induce the infiltration of monocytes and macrophages into tumors and surrounding tissues, upregulating the expression of vascular endothelial growth factor, promoting tumor angiogenesis, and accelerating the growth, invasion, and metastasis of gastric adenocarcinoma cells [15]. Additionally, ROC curve analysis showed that the AUC for predicting gastric adenocarcinoma progression using FABP4, AFP, MCP-1, FABP4+AFP, FABP4+MCP-1, AFP+MCP-1, and combined detection were 0.739, 0.774, 0.711, 0.828, 0.860, 0.846, and 0.965, respectively, suggesting that these indicators can be used to predict gastric adenocarcinoma progression, with combined detection having higher predictive value, assisting in screening high-risk patients for timely intervention.
In summary, serum levels of AFP and MCP-1 are elevated in gastric adenocarcinoma patients, while FABP4 levels are decreased, and these levels are closely related to tumor diameter and TNM stage. Combined detection can be used to predict the progression of gastric adenocarcinoma, providing high value.