
Comparative Effectiveness Research (CER) is translated into Chinese as “比较效果研究”. At first glance, it seems cheerful. Comparing effects? Most clinical studies are about comparing effects; what makes it special? Let’s look at the definition provided by Amy Price et al. in their paper: it generates and synthesizes evidence for medical activities related to prevention, diagnosis, treatment, and monitoring of a problem by comparing benefits and risks. The purpose of CER is to help patients, clinicians, payers (insurance departments), and policymakers choose appropriate diagnostic and therapeutic measures to improve the level of healthcare services at both the population and individual levels.
CER aims to produce medical service reports/papers targeted at different populations, some for patients, some for doctors, and some for insurance departments, etc. What research designs are available for CER? Theoretically, there are no limitations on the research design forms for CER, which can include systematic reviews/Meta-analyses, cross-sectional studies, case-control studies, cohort studies, and RCTs, among others. The main feature of CER is that the outcome of its research is “comparative effectiveness”, providing practical guidance for reference, often involving large-scale clinical studies.

Outcome research is translated into Chinese as “实效研究”. So, what is outcome research? Stephanie J. Lee et al. state in their paper: from an extreme perspective, all outcomes are outcomes, which implies that all research is outcome research. This is certainly inappropriate. So how do we distinguish outcome research from clinical trials? The currently popular view is to look at whether the research observes effectiveness (effectiveness) or efficacy (efficacy); if it is effectiveness, it is outcome research, while if it is efficacy, it is a clinical trial. The term “effectiveness” refers to research conducted in clinical practice, involving a heterogeneous population, with observation metrics that are relatively long-term; whereas efficacy refers to research conducted under clinical trials, involving a homogeneous population, with observation metrics that are short-term indicators or biological markers, etc.
However, effectiveness and efficacy sometimes share commonalities, as shown in the following diagram: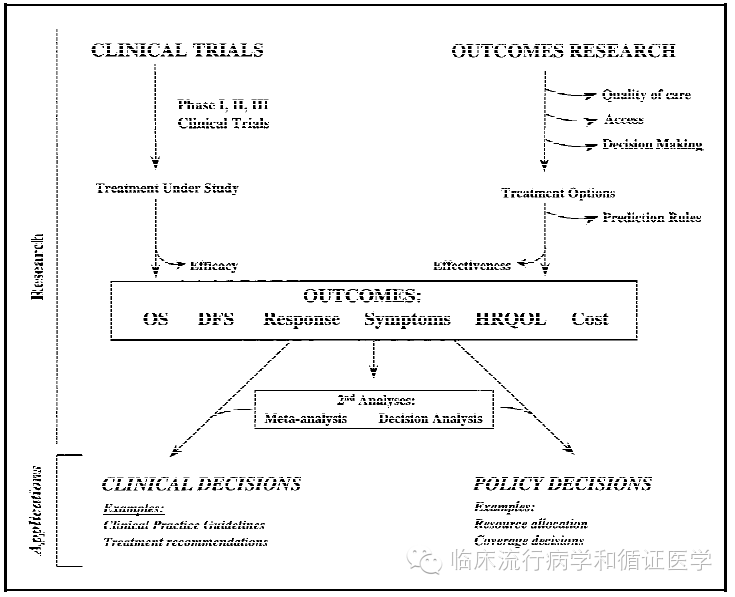
When the outcome metrics are overall survival (OS), if observed in a phase III drug clinical trial, it is efficacy; while in a community-based cohort study, it is effectiveness. Both outcome research and clinical trials can yield clinical and policy decisions. Stephanie J. Lee et al. also provide a relatively broad definition of outcome research: it refers to studies in clinical research focusing on health status, quality of life, and outcomes, while not focusing on efficacy in drug clinical trials and animal experiments. Thus, outcome research naturally includes all research forms except drug clinical trials and animal experiments.

Real-world research translates to “真实世界研究”. This research is conducted in the “real world”, meaning there are no strict limitations on the selection of research subjects and clinical drug treatments. Its research environment is closer to clinical reality, allowing its research results to be better applied in clinical practice. Real-world research includes not only pragmatic clinical research but also observational studies, such as cohort studies.
David Price et al. point out: it is proposed in contrast to traditional or classic RCTs, emphasizing the external validity of research, i.e., the generalizability of research results in clinical practice, which is similar to pragmatic clinical trials. In addition, it includes various observational studies, such as cohort studies.
Below, I will summarize the differences between classic RCTs and pragmatic RCTs: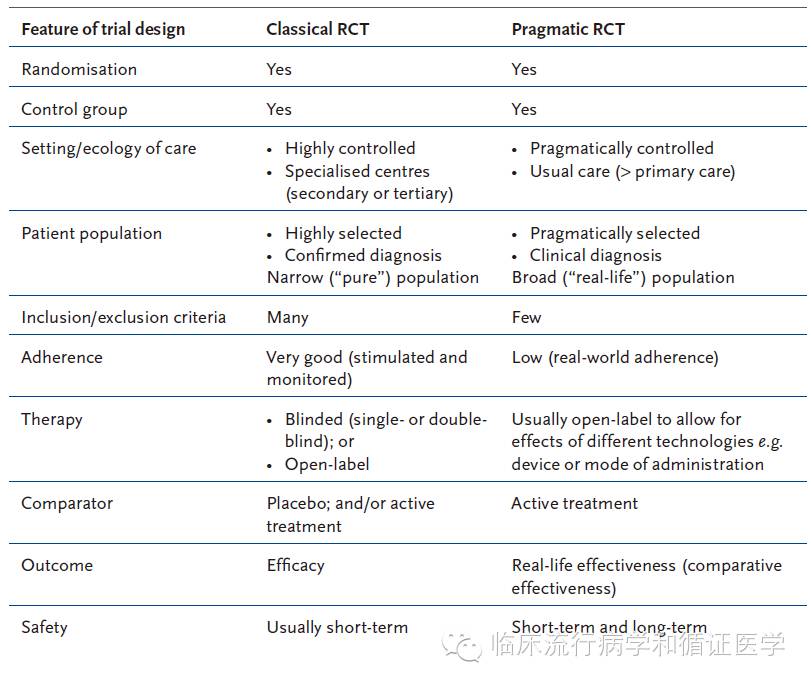 After understanding the concepts and characteristics of Comparative Effectiveness Research, Outcome Research, and Real-world Research, I would like to summarize: (1) These three types of research are proposed in specific environments, each with its distinct characteristics; (2) The relationships between these three types of research are quite chaotic, with no strict distinctions; (3) These three types of research encompass various common research design types, such as cross-sectional, case-control, or cohort studies, and their naming is also research, which differs in meaning from study in English; (4) What is the value of their proposal? I feel their value exists more at the policy level, with limited impact on advancing the evolution of clinical research types; (5) The above summary only represents personal views.
After understanding the concepts and characteristics of Comparative Effectiveness Research, Outcome Research, and Real-world Research, I would like to summarize: (1) These three types of research are proposed in specific environments, each with its distinct characteristics; (2) The relationships between these three types of research are quite chaotic, with no strict distinctions; (3) These three types of research encompass various common research design types, such as cross-sectional, case-control, or cohort studies, and their naming is also research, which differs in meaning from study in English; (4) What is the value of their proposal? I feel their value exists more at the policy level, with limited impact on advancing the evolution of clinical research types; (5) The above summary only represents personal views.
References:
[1]. A,P., C. P and B. R, comparative effectiveness research collaboration and precision medicine. Ann Neurosci, 2015. 22(3): p. 127-9.
[2]. Lee, S.J., C.C. Earle and J.C.Weeks, Outcomes research in oncology: history, conceptual framework, and trends in the literature. J Natl Cancer Inst, 2000. 92(3): p. 195-204.
[3]. Knottnerus, J.A. and P.Tugwell, Real world research. Journal of Clinical Epidemiology, 2010. 63(10): p. 1051-1052.
[4]. Price,D., et al., Real-world research and its importance in respiratory medicine. Breathe (Sheff), 2015. 11(1): p. 26-38.
Source: Clinical Epidemiology and Evidence-based Medicine
