
MEDICOOL . Medical Library
// 1 Definition //
●Instability of the extensor tendon at the metacarpophalangeal (MCP) joint is divided into two categories: subluxation and dislocation.
●Subluxation refers to the lateral displacement of the extensor tendon beyond the midline while still maintaining contact with the condyle when the MCP joint is fully flexed.
●The definition of dislocation is when the extensor tendon is displaced into the groove between the metacarpal heads.
●Instability of the extensor tendon at the MCP joint often occurs in patients with underlying inflammatory conditions (i.e., rheumatoid arthritis).
●Injury to the sagittal band, particularly the radial sagittal band, can lead to instability of the extensor tendon. Although injuries to the ulnar sagittal band have also been reported, the vast majority of extensor tendon instability is caused by injuries to the radial sagittal band.
●In non-rheumatic patients, extensor tendon instability is relatively rare.
●Because the sagittal band covers or wraps around the MCP joint, it is sometimes referred to as the “barrier” ligament.
●Based on the degree of extensor tendon instability, sagittal band injuries are classified into Type I, II, and III.
●Traumatic extensor tendon subluxation at the level of the MCP joint is classified as a Type II injury, while complete dislocation is classified as a Type III injury. These injuries are commonly referred to as “boxer’s injuries.”
●Not all sagittal band injuries will lead to extensor tendon subluxation; clinical examination can help differentiate patients with extensor tendon instability.
●Factors affecting treatment include symptoms and the interval between injury and medical consultation.
// 2 Anatomy //
●The extensor structures at the level of the MCP joint include the extensor tendon sagittal bands and the palmar plate. The sagittal bands are part of a complex extensor support system that includes triangular ligaments between the lateral tendon bundles, transverse support ligaments, and oblique support ligaments at the proximal interphalangeal (PIP) level (Figure 1A).
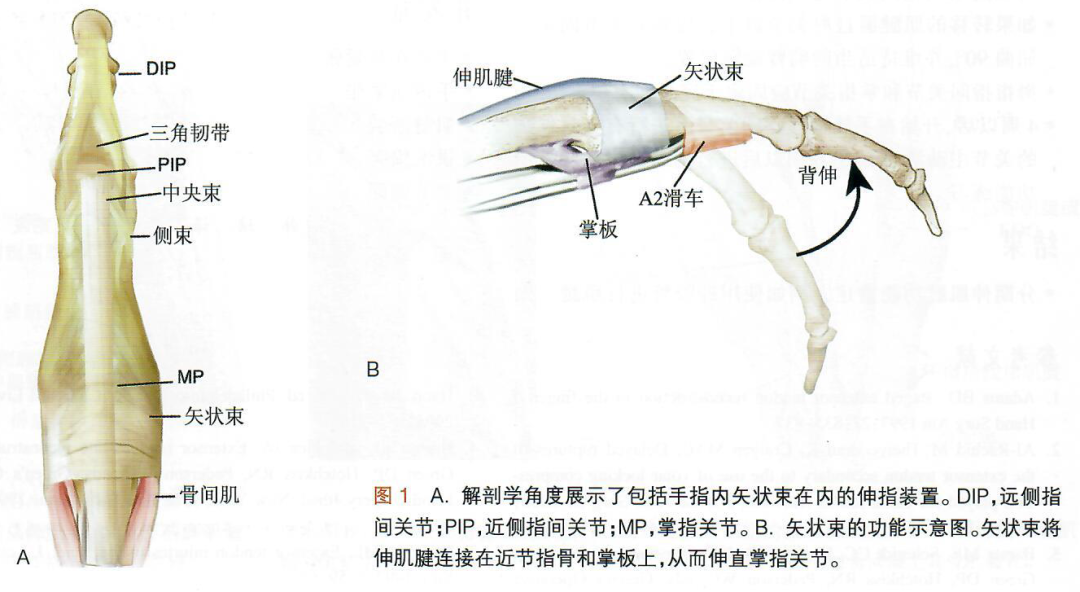
●The sagittal bands are dynamic structures that wrap around the extensor tendon, maintaining the tendon in the center of the joint during flexion of the MCP joint, preventing bowstring deformity during hyperextension, and controlling tendon displacement. The sagittal bands attach to the palmar plate covering the MCP joint (Figure 1B).
●At the MCP joint, the sagittal bands are the primary stabilizing structures of the extensor tendon, and their integrity is essential for normal tendon function.
●When the MCP is in a neutral extended position, the sagittal bands are perpendicular to the tendon.
●There are significant anatomical and physiological differences between the sagittal bands and the deep lateral collateral ligaments.
●The radial sagittal band is more elongated compared to the ulnar sagittal band.
●The sagittal bands are under the most tension during flexion of the wrist and MCP joints and when there is ulnar deviation.
●The lumbrical muscles achieve flexion of the MCP and extension of the interphalangeal (IP) joints through the lateral bands, originating from the flexor digitorum profundus (FDP) tendon, crossing to the radial side of the fingers, and inserting into the extensor tendon expansion.
●The interosseous ligaments are very strong, originating from the necks of adjacent metacarpals and inserting into the necks of nearby metacarpals, located on the dorsal side of the lumbrical tendons and the palmar side of the interosseous tendons.
// 3 Pathophysiology //
●Sagittal band injuries typically occur due to direct trauma while the MCP joint is in a flexed position.
●Sagittal band injuries can also occur due to indirect flexion forces or direct shear forces on the sagittal bands.
●Other mechanisms include displacement of the finger due to trauma, which usually occurs when the MCP joint is in an extended position.
●In open injuries, the sagittal bands are often torn.
●Sometimes, tearing of the combined tendons can also lead to extensor tendon subluxation.
●Typical extensor tendon subluxation involves at least 50% rupture of the proximal sagittal band. When the MCP joint is flexed, the extensor tendon no longer remains centered in the joint but subluxates ulnarly.
●Studies have shown that finger sagittal band injuries correlate with the diameter of the sagittal band cross-section, the extent of the distal attachment, and the length of the sagittal band. Typically, the middle finger sustains the most injuries.
●Research indicates that traumatic subluxation occurs in patients with superficial and deep tears surrounding the extensor tendon sagittal bands.
●When underlying inflammatory conditions flare up, the sagittal bands begin to atrophy and thin, resulting in the extensor tendon displacing into the groove between the metacarpal heads. This non-traumatic extensor tendon dislocation often deviates ulnarly.
// 4 Natural Course //
●In typical patients, symptoms from acute injuries will subside within three weeks with appropriate treatment, although pain may persist for up to nine months before completely resolving.
●If swelling discomfort and subluxation of the sagittal band are ignored, symptoms will progressively worsen over time. The extensor tendon may become passively fixed in the groove between the metacarpal heads, leading to loss of extension and abduction function. These patients may require surgical intervention to alleviate symptoms.
// 5 History and Physical Examination //
●This article discusses traumatic subluxation. The treatment plan for inflammatory subluxation differs and is not included in this article.
●The key to treatment is understanding the environment surrounding the injury. This information will help identify the risk of infection in open wounds (e.g., clean lacerations, bites) or potential systemic diseases that may contribute to closed injuries caused by low-energy trauma.
●Shortly after trauma, soft tissue swelling may make it difficult to identify the alignment of the tendons over the MCP joint.
●Initial symptoms and signs of traumatic sagittal band injuries and subsequent extensor tendon instability include:
●Localized pain
●Associated swelling of the MCP joint
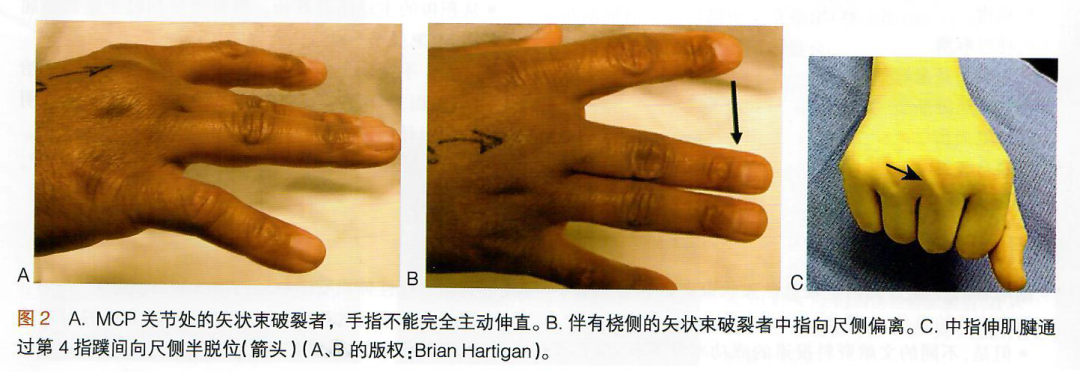
●Limited range of motion (Figure 2A)
●Limitation of extension at the MCP joint or lateral deviation during extension, or both (Figure 2B)
●Weakness in extending the MCP joint
●Painful snapping of the upper tendon may occur during active flexion of the MCP joint (Figure 2C)
●Ulnar deviation deformity and early or late difficulty in adduction of the affected finger (abduction difficulty in the index finger).
●Patients with chronic tendon instability often exhibit pain during flexion of the MCP joint, accompanied by local tenderness and swelling of the damaged sagittal band, such as during gripping actions.
●When the MCP joint is passively placed in an extended position, extension can be actively maintained. However, attempting to extend the MCP joint from a flexed position or flex the MCP joint from a fully extended position is often very difficult.
●Methods to examine extensor tendon instability at the MCP joint include:
●Assessing the range of motion of the sagittal band throughout the MP.
●Evaluating swelling, open wounds, etc. to determine the site of the lesion.
●Palpating the MCP joint and the groove between the metacarpal heads.
– Sagittal band injuries will present with superficial tenderness. In contrast, pain associated with collateral ligament injuries is often deep, located in the groove between the metacarpal heads.
●Performing tendon instability tests.
●Instructing the patient to flex the MCP and wrist joints, the position that places maximum ulnar deviation stress on the extensor tendon at the MCP joint. This will help determine the degree of instability.
●Pain provocation tests: In the extended position of the distal and proximal IP joints and the flexed position of the MCP joint, instruct the patient to extend the MCP joint against resistance as much as possible.
To be continued in the next issue…
The original text is excerpted from “Wiesel’s Orthopedic Surgery (Volume 3)”
Editor-in-Chief: Sam W. Wiesel (USA); Chief Translator: Zhang Changqing
////////////////////////////////////
Want to connect with more orthopedic experts?
Want to learn more professional insights?
Long press and scan the QR code below to add Orthopedic
Doctor WeChat Group group owner – Xiaoku
Please be sure to note: Orthopedic Doctor
The Elite Orthopedic Doctors Group 1 welcomes your joining
