✦
Deep Learning Soup Group Literature Review Study Fifty-Seven
Predicting Neurological Outcomes in Cardiac Arrest Patients Using Artificial Neural Network Algorithms and Cumulative Patient Information
Deep Learning Soup Group
September 30, 2022
In 2021, Peder Andersson and colleagues from Skåne University Hospital in Lund, Sweden, utilized artificial neural networks to predict the neurological outcomes of patients who remained in a coma after cardiac arrest resuscitation. They also investigated the prognostic potential of biomarkers, patient background information, and factors related to intensive care monitoring and treatment. Their article titled “Predicting neurological outcome after out-of-hospital cardiac arrest with cumulative information; development and internal validation of an artificial neural network algorithm” was published in the journal Critical Care (IF: 19.333).
DOI:
https://doi.org/10.1186/s13054-021-03505-9
1. Research Background
In the field of intensive care, predicting whether patients who remain in a coma after cardiac arrest resuscitation can fully recover neurologically or suffer severe neurological damage is a critical area of research. However, this prognosis is influenced by many factors, necessitating robust and reliable methods for data analysis and prediction. Although existing multimodal clinical neurological examinations such as EEG, somatosensory evoked potentials, neuroimaging, and biomarkers can prognosticate neurological outcomes, this study posits that demographic and clinical variables also hold prognostic value, yet current methods have not utilized this information. Previous studies have demonstrated that certain biomarkers are closely related to brain injury, cardiac loss, and systemic inflammation; this study incorporates these biomarkers and categorizes them into clinically usable and research-grade biomarkers based on their measurement frequency in current clinical and laboratory practices.
With advancements in machine learning algorithms and increased computational power, diagnostic and prognostic capabilities in various medical fields, including intensive care medicine, have been enhanced. Many studies have confirmed that machine learning shows promising results in short-term and long-term prognoses for out-of-hospital cardiac arrest (OHCA) survivors. In a recently published study, an artificial neural network (ANN) machine learning algorithm outperformed logistic regression in predicting neurological outcomes based on patient admission information. Building on this research, this study hypothesizes that an ANN model based on cumulative information obtained in the first three days of intensive care can reliably predict neurological damage in OHCA patients.
2. Dataset
This study included 939 unconscious OHCA survivors, with the inclusion criteria being adults (≥18 years) who were in a coma (Glasgow Coma Scale ≤8). In subsequent data analysis, 7 patients who were lost to follow-up after 6 months or had excessive missing data were excluded. Additionally, the study materials consisted of patient information at three different time points: 24, 48, and 72 hours post-cardiac arrest. To restrict the prognosis to comatose patients, those who awoke or died at these time points were excluded, as shown in Figure 1. The outcomes were classified using the Cerebral Performance Category (CPC) scoring method, assessed by evaluators through face-to-face or telephone interviews during a 6-month follow-up. Good outcomes were defined as CPC 1-2, while poor outcomes were CPC 3-5. A total of 440 patients (47%) had good outcomes (CPC 1-2), and 492 patients (53%) had poor outcomes (CPC 3-5).
The variables studied included patient background information, pre-hospital and admission records, and data obtained at 24, 48, and 72 hours. During these three days, blood samples were taken daily to obtain patient biomarker information, which was categorized into clinically usable biomarkers and research-grade biomarkers. Three models (A, B, and C) were established each day, resulting in nine datasets. Model A: clinical variables only; Model B: added clinically usable biomarkers, such as neuron-specific enolase (NSE); Model C: added research-grade biomarkers, such as neurofilament light (NFL).
To ensure that the prognostic value of biomarkers was not diminished by technical issues, patients with missing values in the biomarkers for Models B and C were excluded, resulting in approximately a 30% reduction in the number of patients in each dataset.
3. Methods
Throughout the model development process, 80% of patients were randomly assigned to the training group, while 20% were assigned to the testing group. For each model, the following scheme was used for variable selection and imputation of missing values. Each variable had a maximum of 20% missing values. Binary variables had at least 2% unique events. The correlation between variables did not exceed 98%. The median or mode was used for imputation of missing values below the 20% threshold. The ANN model used to predict the neurological outcomes of OHCA survivors at 6 months consisted of an input layer, several hidden layers, and an output layer. During development, five-fold cross-validation and Bayesian optimization algorithms were used for hyperparameter tuning to find the best model under constraints. The model with the highest average AUROC in cross-validation was selected for further analysis.
After the model development was completed, the SHAP (SHapley Additive exPlanations) algorithm was applied to all models. The SHAP plots obtained provide a visual representation of which variables influenced the predictions for individual samples and the relative contribution of each variable.
The ROC curve was used to evaluate the predictive models, and the AUROC for all models was calculated based on the testing set. To assess the prognostic capability of the models, confusion matrices for all testing sets were computed. The P-value for each variable was calculated, with P < 0.05 indicating that the variable was significant.
4. Results and Conclusion
After excluding 6 patients due to missing outcomes and 1 patient due to missing values, a total of 932 patients were included in this study. As described in the methods section, three datasets were created each day according to the categories of biomarkers, with Table 1 showing the number of patients and variables for each dataset. The nine models constructed from days 1 to 3 demonstrated good to excellent prognostic performance in predicting neurological outcomes at 6 months, as shown in Figure 2. Using clinical variables (Model A), the AUROC remained below 90% during the first three days of intensive care. With the addition of clinically usable biomarkers (Model B), the AUROC increased from 82% to 94% (P < 0.01). For the research-grade biomarker model (Model C), the prognostic performance remained strong from day 1 to day 3, with an AUROC of approximately 95%, as shown in Table 1 and Figure 2.
By applying the SHAP algorithm to our models, the predictive models can be interpreted. As shown in Figure 3, the age of 77 years increased the risk of poor prognosis, while low levels of biomarkers (NFL, NSE) reduced the risk of poor prognosis. When constructing the three models using the patient information from the second day, age and the dose of epinephrine during resuscitation were the two most important clinical variables. The significant role of epinephrine dosage may be related to the initial cardiac rhythm. After adding biomarkers to the model, the top ten important variables were primarily biomarkers, as shown in Figure 4. Notably, age remained an important variable across all three models, likely due to age being a risk factor in itself.
In this exploratory retrospective study, ANN demonstrated very good accuracy in predicting neurological outcomes in comatose patients after OHCA by utilizing clinical variables and biomarkers from the first three days of intensive care. It validated that research-grade biomarkers like NFL have the strongest predictive capabilities for neurological outcomes. Over time, the value of clinical variables in predicting neurological outcomes becomes negligible compared to that of biomarker variables.
Glossary
1. Cerebral Performance Category (CPC): The CPC classifies neurological outcomes as follows: CPC 1, good performance; CPC 2, moderate disability; CPC 3, severe disability; CPC 4, coma or persistent vegetative state; CPC 5, brain death or death. CPC scores are further categorized into good (CPC 1 or 2) and poor (CPC 3, 4, or 5).
2. SHAP (SHapley Additive exPlanations): A unified method for interpreting any machine learning model output, utilizing classical Shapley values from game theory and their related extensions to link optimal credit allocation with local interpretability.
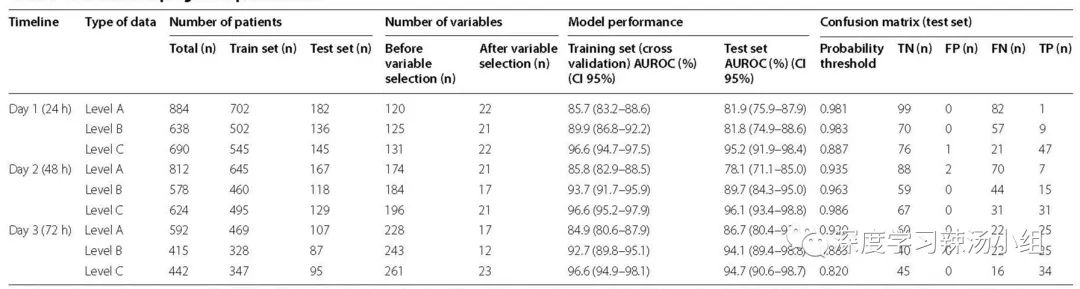
Table 1: Overview and Prognostic Performance
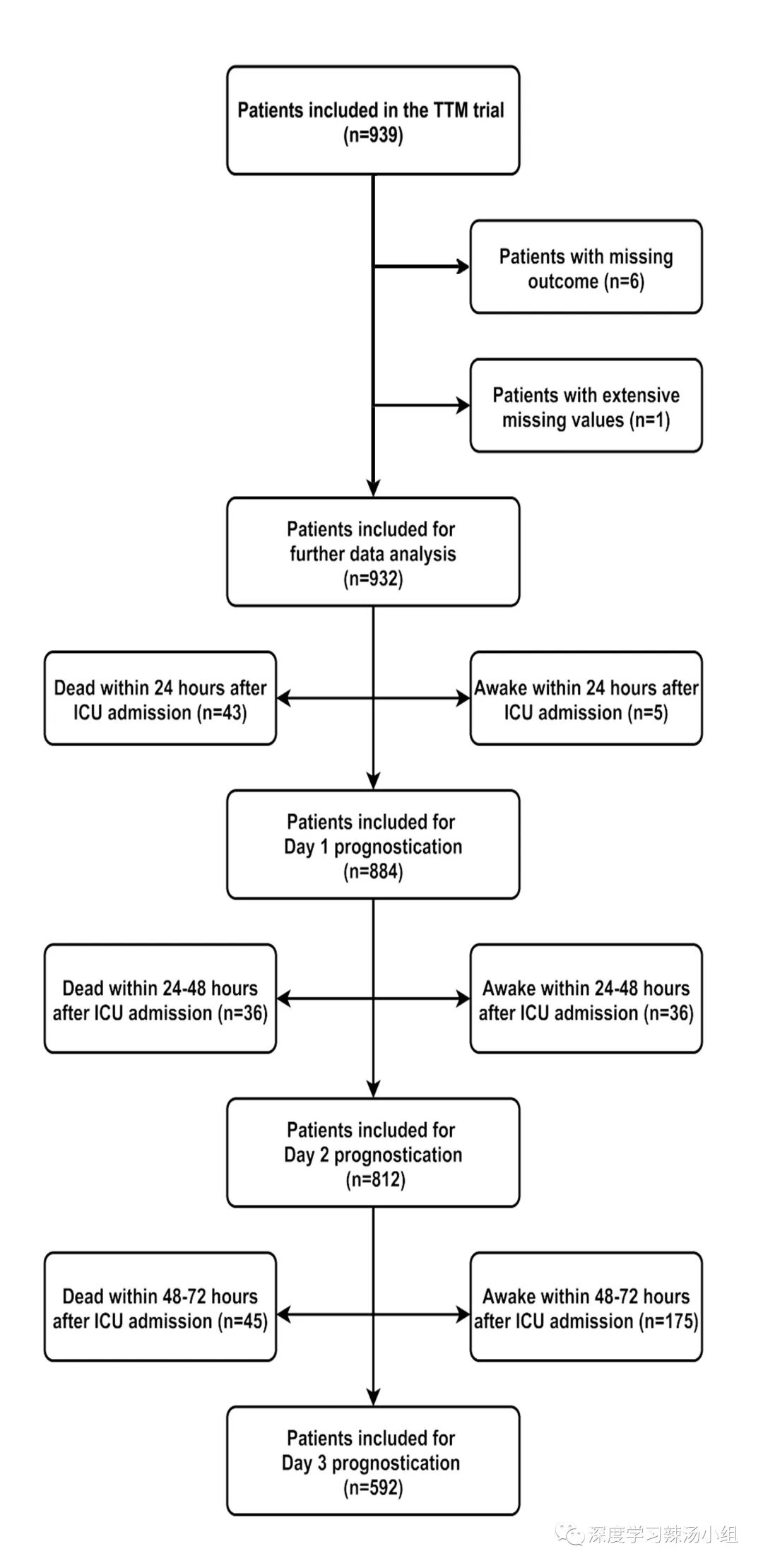
Figure 1: Flowchart of the Study Population on Days 1, 2, and 3 Post-Admission
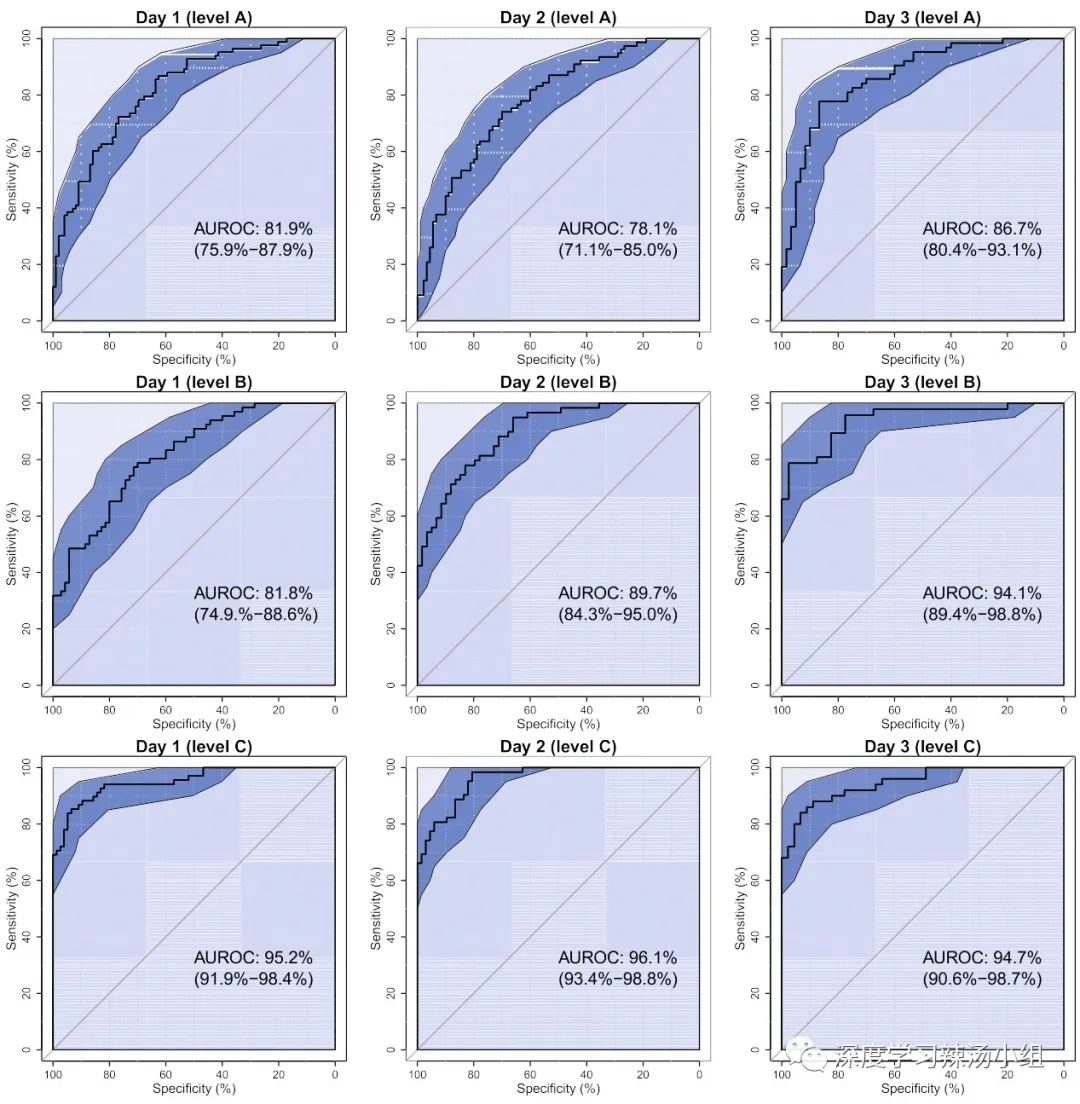
Figure 2: ROC Curves, AUROC, and 95% Confidence Intervals for Nine Models

Figure 3: Influence of Features on Predictions for a Sample

Figure 4: SHAP Variable Importance for the Three Models Based on Patient Information from the Previous 48 Hours
Pepper soup transformed by: Geng Shi
//
The Deep Learning Soup AI Group consists of a group of AI enthusiasts from Xuzhou Medical University and its affiliated hospital. We welcome everyone to communicate and learn with us!

Scan to Follow Us
Welcome to join us!
Member WeChat ID:cy2011mcu
Please note when adding friends:
Your Unit-Department-Name-Research Direction