
Xiaolei Zhang, Chenghuan Hu, Translated by Shuangping Zhao, Proofread
Abstract:
Neurocritical patients are at risk of secondary brain injury, which is caused by inflammation, ischemia, and edema resulting from primary injuries. Recognizing clinical deterioration due to secondary injury in comatose patients is often challenging. Multimodal monitoring (MMM) includes various tools to monitor brain metabolism, perfusion, and oxygenation, aiming to detect these changes to help adjust treatment before irreversible damage begins. These tools include intracranial pressure (ICP) monitors, transcranial Doppler (TCD), Hemedex (for measuring local cerebral blood flow using thermal perfusion probes), microdialysis catheters (for measuring brain metabolism), Licox (for measuring local brain tissue oxygen tension), and continuous electroencephalography. Although further research is needed to demonstrate their impact on improving clinical outcomes, their role in elucidating the black box of the comatose brain is undeniable. In this review, we further elaborate on commonly used MMM parameters, the tools used to measure these parameters, and the indicators for monitoring based on current consensus guidelines.
1. Introduction
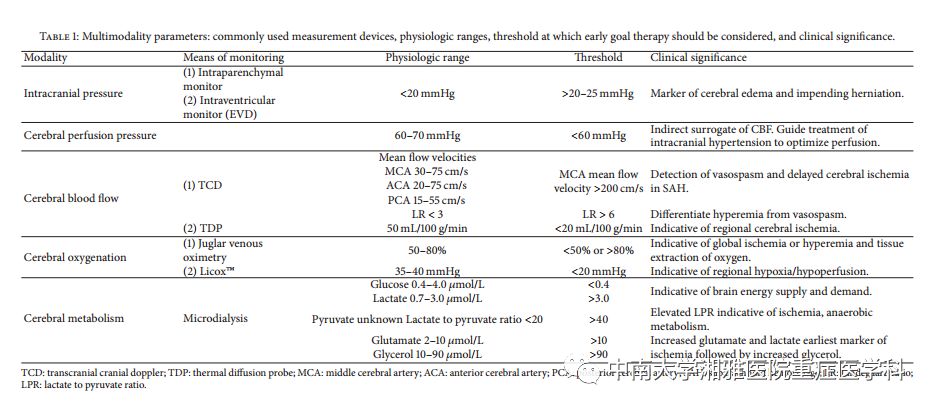
Acute brain injury (ABI) typically presents with varying degrees of altered mental status and very limited neurological examination. Unfortunately, these patients are at risk of further deterioration due to inflammation, edema, and local ischemia caused by primary injuries. This downstream damage is referred to as secondary brain injury (SBI) and is often missed in non-responsive and sedated neurocritical patients. Cutting-edge technologies now provide sophisticated tools that allow us to collect real-time integrated information about the pathophysiological processes of comatose patients, termed multimodal monitoring (MMM). The goal of MMM is to detect SBI early by monitoring changes in physiological parameters that reflect cell death and damage. These parameters include intracranial pressure (ICP), cerebral perfusion pressure (CPP), cerebral blood flow (CBF), brain tissue oxygenation, brain metabolism, and cortical electrical activity (see Table 1). Information obtained from these tools, if integrated into clinical decision-making and early goal-directed therapy, may help prevent SBI before irreversible damage occurs.
In this review, we further elaborate on commonly used MMM parameters, the tools used to measure them, and the indicators for monitoring based on current consensus guidelines.
2. Intracranial Pressure (ICP) and Cerebral Perfusion Pressure (CPP)
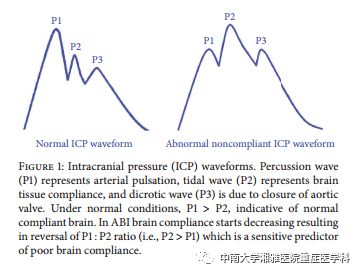
ICP and CPP are the most commonly monitored parameters in patients with acute brain injury. The brain parenchyma, cerebral blood volume, and cerebrospinal fluid represent normal intracranial components contained within an inelastic bony structure. The modified Monro-Kellie doctrine states that the total volume of the intracranial contents is constant, and an increase in one or both can offset a decrease in one or both. This principle can be viewed as a buffering effect when there is a slight increase in volume, with minimal changes in ICP. However, in acute brain injury (traumatic or vascular), a significant increase in volume, manifested as cerebral edema or hematoma, can elevate ICP, leading to reduced cerebral blood flow, ultimately resulting in ischemia and brain herniation. The normal ICP range in adults is between 7 and 15 mmHg. An ICP value exceeding 20 mmHg indicates intracranial hypertension. Besides absolute values, ICP waveforms should also be assessed as they provide important information on whether the probe is correctly placed and the state of brain compliance (Figure 1). There is sufficient evidence supporting continuous ICP > 20 mmHg, especially when treatment is difficult, leading to worse outcomes.
CPP is the difference between MAP and ICP. It represents the pressure gradient driving cerebral blood flow (CBF) and ensures the delivery of oxygen and metabolites. It is also considered an indicator of the brain’s autoregulation mechanism. Normal adult CPP > 50 mmHg. According to recent guidelines for traumatic brain injury, the recommended CPP for favorable outcomes is between 60 and 70 mmHg, with the patient’s autoregulation state being the most important factor determining the minimum CPP threshold. A grade III recommendation states that to prevent the risk of adult respiratory distress syndrome, excessive use of fluids and vasopressors should be avoided to maintain CPP above 70 mmHg. However, management based on target CPP rather than ICP has not shown better outcomes. In fact, it has been hypothesized that CPP values should be individualized based on the disease state and information collected through ICP, oxygenation, and metabolic monitoring. A recent retrospective cohort study analyzed the adherence to current guidelines and the trends in 2-week mortality in TBI patients. They found that as adherence to the guidelines improved, the 2-week post-injury mortality significantly decreased, especially in cases guided by both ICP and CPP monitoring.
The Brain Injury Foundation (third edition) and MMM consensus guidelines recommend ICP and CPP monitoring for all ABI patients with a Glasgow Coma Scale of 8 or less, and/or those at risk of elevated ICP based on clinical and/or imaging features. However, these recommendations were not implemented in the fourth edition of the Brain Injury Foundation guidelines as they stemmed from descriptive studies or studies that did not meet inclusion criteria. Current guidelines recommend using information from ICP monitoring to manage severe traumatic brain injury patients to reduce inpatient and 2-week post-injury mortality (IIB level).
Compared to external ventricular drainage (EVD), internal pressure sensors are easier to place and provide continuous monitoring, where the drainage system must be closed to measure ICP. Currently popular technologies include piezoelectric strain gauges (Codman micro-sensors and Raumedic Neurovent) and fiber optic (Integra Camino) sensors. These devices require insertion into the brain parenchyma 1.5 to 2 cm through a burr hole. The optimal position should be close to the injury area, especially in focal lesions, as interhemispheric differences exceed 10 mmHg in focal lesions with mass effect. Therefore, CT imaging is typically recommended after positioning. Notably, Codman and NeuroVent are MRI-compatible. Intraparenchymal monitors are more expensive; their measurements drift over time and cannot be recalibrated. Other less precise monitors include subarachnoid screws and epidural fiber catheters, which are rarely used in clinical practice.
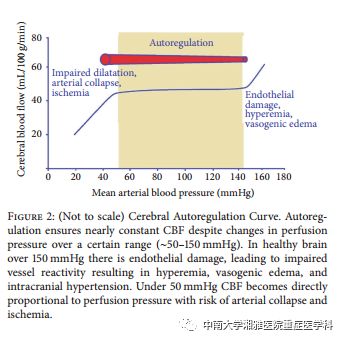
Autoregulation is another important aspect of cerebral perfusion monitoring. An uninjured brain can maintain relatively stable cerebral blood flow despite fluctuations in perfusion pressure by altering the caliber of cerebral vessels (Figure 2). In an injured brain, this autoregulation mechanism is disrupted, putting patients at risk of SBI due to ischemia caused by hypotension, whereas increased MAP can elevate ICP, leading to congestion. This adaptive feature of the cerebrovascular system can be quantified as static autoregulation, reflected by the concept of the pressure reactivity index (PRx). PRx measures the correlation between arterial blood pressure and ICP waves and reflects the brain’s autoregulation response to blood pressure changes. PRx is scaled as a correlation coefficient (from +1.0 to -1.0), with positive values indicating a linear correlation with MAP changes, reflecting impaired autoregulation status. A retrospective cohort study showed that patients with PRx values < 0.25 (20% vs. 69%) had lower mortality rates.
3. Cerebral Blood Flow (CBF)
Cerebral blood flow can be monitored non-invasively using transcranial Doppler (TCD) by measuring the mean flow velocity of different cerebral volumes, allowing for a more comprehensive assessment. TCD is primarily used to detect vasospasm in subarachnoid hemorrhage (SAH), identifying patients at risk of delayed ischemia. It is also more reliable for assessing the anterior circulation, with an average MCA flow velocity > 200 cm/s having a high probability of predicting clinically significant vasospasm. However, increased velocity can reflect either vasospasm (i.e., reduced diameter) or congestion. The Lindegaard ratio (LR), which is the ratio of the highest flow velocity in the MCA to the highest flow velocity in the external ICA, helps distinguish between hyperperfusion and vasospasm, with LR values > 3 considered indicative of the difference between the two. The predictive capability of TCD is particularly suitable for difficult-to-sonicate vessels (ICA and ACA) and can be improved through transcranial color-coded duplex ultrasound. Limitations of TCD include operator-dependent variability and the inability to distinguish symptomatic from asymptomatic vasospasm, especially at velocities between 120 and 199 cm/s.
CBF can also be measured by directly inserting a thermal diffusion probe (TDP) into the brain parenchyma. Commercial systems include the Hemedex monitoring system, which is incompatible with MRI. It allows for regional CBF (rCBF) monitoring by assessing the thermal convection caused by tissue blood flow. The probe tip is inserted into the white matter of the brain, and its utility depends on proximity to the area of interest. TDP has been validated by CT, and CBF levels below 15 mL/100g/min have been determined as diagnostic thresholds for low perfusion. According to MMM consensus guidelines, TDP should be placed in the vascular territory of a ruptured aneurysm to monitor vasospasm. Quantifying rCBF with TDP is highly dependent on the patient’s core temperature and shows significant changes under hyperthermic conditions.
So far, there have been no published studies demonstrating improved outcomes guided solely by CBF monitoring, but it appears to be a promising tool when used in conjunction with other parameters.
4. Brain Tissue Oxygen Saturation
Maintaining adequate oxygenation is crucial for neurocritical patients. Brain oxygenation serves as a surrogate marker for CBF and, along with metabolic parameters, acts as a marker for tissues at risk of ischemia. The brain tissue oxygenation index (PbtO2) is a product of the difference in oxygen tension between cerebral arteries and veins.
PbtO2 serves as an adjunct to ICP monitoring to guide the management of CPP in ABI patients and adjust individual CPP thresholds. PbtO2 is an invasive means of monitoring local brain oxygen pressure by inserting a microcatheter into the white matter, located in areas of ischemic risk identified by CT or MRI perfusion studies. Two commercial probes are available for monitoring PbtO2: the Licox system (which provides additional ICP and brain temperature monitoring) and the NeuroVent PTO system (which measures carbon dioxide partial pressure and pH). Both methods can measure oxygen content in adjacent white matter safely and effectively, but they are not interchangeable, as significant differences in measured PbtO2 values have been observed when comparing the two devices. Using Licox, normal PbtO2 is reported to be 23-35 mmHg. Current MMM guidelines consider PbtO2 below 20 mmHg as a threshold for considering intervention.
SjVO2 monitoring requires the retrograde insertion of a specialized fiber-optic catheter into the internal jugular vein, preferably into a prominent vein, to assess overall oxygenation. Under stable arterial hemoglobin saturation and concentration, SjVO2 reflects the difference between oxygen supply and demand in the brain. Normal levels range from 60-75%. SjVO2 levels below 50% indicate hypoxia. Multiple or continuous ( > 10 minutes) hypoxia is associated with poor prognosis in brain injury patients. SjVO2 levels exceeding 75% indicate congestion or tissue infarction. Blood is collected from the catheter to derive the venous oxygen content and calculate the arterial-venous oxygen content difference (AVDO2). AVDO2 > 9 mL/dL may indicate global ischemia, while AVDO2 < 4 mL/dL indicates congestion. The use of SjVO2 is limited by the need for frequent recalibration and catheter-related complications (including infection, elevated ICP, venous thrombosis, and pneumothorax). Secondly, localized small areas of ischemia may not cause any changes in SjVO2, as it reflects global brain oxygenation.
SjVO2 or PbtO2 monitoring is suitable for patients requiring hyperventilation to control ICP (Pco2 20-25) and those at risk of cerebral ischemia or hypoxia. PbtO2 can also serve as an adjunct to TCD for monitoring delayed cerebral ischemia in comatose SAH patients. In patients with TBI considered to be diffuse processes, it is recommended to place probes in the least injured areas. SAH probes should be preferentially placed in areas at the highest risk of vasospasm (the vascular territory of the ruptured aneurysm), while hemorrhagic probes should be placed near the site of bleeding. PBT O2 monitoring and directed therapy have been shown to improve long-term functional outcomes in patients with low-grade aneurysmal SAH. Current MMM guidelines recommend SjVO2 or PbtO2 monitoring to assist in ICP/CPP-directed therapy, identify refractory intracranial hypertension and treatment thresholds, help control delayed cerebral ischemia, and select patients for secondary treatment of persistent intracranial hypertension. The recent Guidelines for the Management of Traumatic Brain Injury (fourth edition) recommend using jugular bulb monitoring to assess the difference in venous and arterial oxygen content to help guide management decisions (level III). Furthermore, due to insufficient existing evidence to provide formal recommendations, the current recommendations have removed the brain tissue oxygen saturation threshold of less than 15 mmHg for treatment, as a recent retrospective cohort study of 629 patients showed no difference in mortality rates between TBI patients who received ICP and PbtO2 monitoring compared to those who only received ICP monitoring.
Near-infrared spectroscopy (NIRS) is an emerging non-invasive tool for measuring brain oxygenation. It calculates the concentration of chromophores (oxygenated hemoglobin, rSO2 in brain injury patients) based on the light attenuation between a light source and a receiver. A study of 94 randomly selected healthy adults showed an average cerebral oxygen saturation of 67.14±8.84% using near-infrared spectroscopy. However, to date, no studies have established threshold values for rSO2 to predict SBI. Another significant limitation of NIRS is the interference of scalp swelling and epidural/subdural hematomas (common in brain injury patients) on the signal, leading to unreliable measurements.
5. Brain Metabolism
Although monitoring brain tissue oxygen, CBF, and CPP provides essential physiological information, monitoring various substrates, metabolites, and neurotransmitters during acute brain injury can provide more insights into the pathophysiological processes of oxidative metabolism and ultimate mitochondrial dysfunction. This information, combined with data from ICP, CBF, and PbtO2 monitoring, assists in guiding treatment to reduce further brain injury.
Neuroimaging, particularly PET scans and magnetic resonance spectroscopy, provides information about glucose uptake and lactate levels, respectively. However, these imaging modalities provide static information, while brain metabolism is a dynamic process. Furthermore, most patients are critically ill and unable to be transported back and forth to obtain these images. The advent of cerebral microdialysis (CMD) has revolutionized the monitoring of brain metabolism. Through microdialysis, various substrates, neurotransmitters, and metabolites can be analyzed at the bedside every hour. Current MMM guidelines recommend cerebral microdialysis for patients at risk of ischemia, hypoxia, and energy failure or those with ischemia, hypoxia, and energy failure. They also recommend using CMD to assist in titrating drug therapies, such as systemic glucose control, transfusion, and therapeutic hypothermia. A single-center prospective study involving 165 patients explored the management of TBI patients using information obtained from CMD monitoring and found that patients who normalized glutamate within 120 hours of monitoring had reduced mortality rates and better outcomes at six months. However, the recent guidelines for traumatic brain injury have not found sufficient evidence to support any level of recommendation.
The microdialysis catheter is 0.62 mm wide, lined with a semi-permeable membrane with a pore size typically of 20 kDa. The catheter is inserted into the subcortical white matter, perfused very slowly (0.1-2.0 µL/min) with saline or Ringer’s solution via a pump system. Molecules below the membrane cutoff size diffuse down their concentration gradient and equilibrate with the perfusion fluid. This fluid is collected in a vial and analyzed hourly by enzyme spectrophotometry or high-performance liquid chromatography.
Microdialysis in neurocritical care primarily focuses on glucose delivery and metabolism. Under normal conditions, i.e., aerobic conditions, glucose is metabolized to pyruvate and adenosine triphosphate. A reduction in glucose may be due to decreased perfusion, decreased systemic supply, or increased utilization. Conversely, elevated glucose may be due to congestion, increased systemic supply, or decreased metabolism. Under hypoxic conditions or mitochondrial dysfunction (common in ischemic injury), glucose is metabolized to lactate. In fact, lactate, pyruvate, and the lactate-to-pyruvate ratio (LPR) are considered markers of anaerobic metabolism and energy crisis, with LPR being the most reliable among the three. Glutamate is an excitatory neurotransmitter associated with ischemia, inflammation, and cell injury. Compared to other neurotransmitters, it is one of the earliest markers of vasospasm. Glycerol is a component of neuronal structure, and its elevated levels indicate that ischemia has developed into cell injury. Normal adult concentrations of glucose, lactate, and pyruvate while sedated are reported as 1.7±0.9 mmol/L, 2.9±0.9 mmol/L, and 166±47 μmol/L, respectively, with LPR > 40 considered a marker of metabolic distress in TBI. However, in acute brain injury patients, trends in these metabolite concentrations rather than absolute values, combined with other parameters, assist in guiding treatment strategies. For focal brain injury, the microdialysis catheter should be placed at the site of injury. For diffuse brain injury, the catheter should be placed in the right frontal region, while SAH probes should be placed in the watershed area near the ruptured aneurysm. Poor prognosis in severe TBI patients is associated with metabolic disturbances seen in CMD, particularly evidence of low glucose and LPR. In SAH patients with delayed cerebral ischemia, lactate and glutamate levels rise early, followed by glycerol. It has been reported that elevated LPR in SAH patients persists for 11 to 13 hours prior to delayed cerebral ischemia.
6. Electroencephalography
Electroencephalography provides information about brain electrical activity and is used to detect seizures. Most commonly, electrodes are placed on the scalp to record cortical activity. However, in some cases, electrodes can also be applied directly to the surface of the brain, which is more sensitive than scalp EEG for detecting seizures.
Neurocritical patients often experience non-convulsive seizures, which are subclinical. The prevalence of non-convulsive seizures in brain injury patients (including traumatic brain injury, subarachnoid hemorrhage, intracerebral hemorrhage, and hypoxic-ischemic encephalopathy) ranges from 4% to 30%, associated with secondary brain injury, which can be confirmed by elevated LPR and ICP. In comatose patients, continuous EEG monitoring for at least 48 hours is required to detect non-convulsive seizures with a sensitivity greater than 90%. Regardless of the cause, non-convulsive seizures are associated with increased morbidity and mortality.
Current MMM guidelines recommend EEG monitoring for all ABI patients and patients with altered consciousness of unknown origin, as well as for patients in a seizure state within 60 minutes of medication, during therapeutic hypothermia, and for 24 hours after rewarming. In addition to seizures, certain EEG patterns, such as widespread repetitive slow waves, are highly correlated with the occurrence of vasospasm in SAH, leading to the development of quantitative EEG (qEEG). qEEG is data obtained by processing raw EEG data for hours using a compressed spectral array. Variables such as the α/δ ratio, power, and α variability can be used to detect delayed cerebral ischemia in SAH.
Despite the widespread application of routine scalp EEG, it has its limitations, especially in the intensive care unit. Low signal-to-noise ratio, low spatial resolution, poor electrode-skin contact, and electrical interference from devices are factors affecting the interpretation of scalp EEG. In some cases, waveforms are suspicious but cannot diagnose the initial event. Given these limitations, the concept of intracortical depth electrodes has been introduced. Small-scale studies have shown that intracortical depth electrodes can detect seizures and cortical diffuse low-function states that scalp EEG cannot see. The placement of depth electrodes has safety issues similar to other invasive monitoring devices but can potentially be used to identify early changes in brain activity indicative of SBI. They are inserted through dedicated burr holes or EVD with 6 or 8 depth contact electrodes distributed across gray and white matter. The detection rate of seizures is much higher than that of seizures detected by surface EEG, and this technique completely eliminates baseline muscle artifacts. However, larger studies are needed to evaluate the full potential of depth electrodes and assess treatment outcomes based on this monitoring.
7. Integration of MMM Information and Conclusion
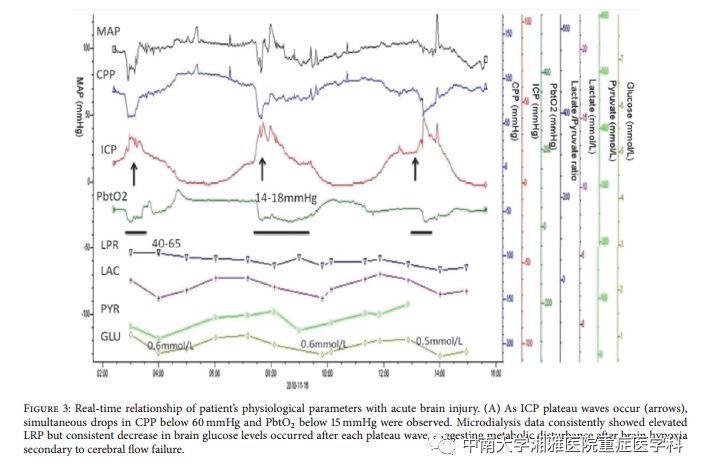
With advancements in technology and informatics, data collection is no longer an issue. The purpose of multimodal neuro-monitoring is not to add new tracking variables for intensivists but to integrate information from multiple modalities to create a patient-specific “injury profile,” which will help guide the development of optimal treatment plans. Figure 3 illustrates an example of how to integrate information from various modalities to determine optimal patient-specific thresholds, describing real-time monitoring of patient physiological parameters and the impact of elevated ICP on CPP and PbtO2, ultimately leading to regional hypoxia reflected by the degree of decline in brain glucose levels.
Given the complexity of the data and the need for overall interpretation of these parameters, a collection system (including MMM, vital signs, cEEG, and temperature, all parameters fully integrated) is crucial. Currently, there is only one commercial system called CNS Monitor (Moberg Research) that allows for monitoring a single patient at any given time. Further development of integrated systems with optimal signal-to-noise ratios, making sophisticated event detection algorithms a necessary component of a complete integrated approach.
Nevertheless, MMM has become a reality widely used in neurocritical care units around the world. Although various studies have demonstrated the physiological feasibility of monitoring various neurological parameters, there are still no publicly available randomized trial data to support the notion that any single variable can improve clinical outcomes. Steiner et al. analyzed the relationship between MAP and ICP to determine the optimal CPP for 114 patients with brain injury and demonstrated that patients whose mean CPP approached their “optimal” CPP target were more likely to achieve favorable outcomes.
Ideally, studies using multimodal bedside monitoring will help determine patient-specific physiological thresholds, enabling neurologists to optimize patients’ physiological functions and minimize secondary neurological damage. With the continuous development of bioinformatics, further improvements to systems that provide physicians with real-time, accurate individual physiological status information are just a matter of time.
