
The active examination can assess the patient’s ability to move around the axis of motion, reflecting their ability under normal conditions, as well as their ability in the presence of pain, degenerative joint disease, muscle hypertonicity, sprains, or strains. Static structural or postural examinations will provide clues about movement patterns.
The normal range of motion depends on the patient’s body type and the diseases causing their dysfunction. Therefore, the mobility of each category of patients is different. Considering factors such as the different muscle types and elasticity of patients with different body types, doctors can gain a better understanding of the overall functional impairment state presented by the patient.
During the examination, the doctor can allow the patient to perform active movements or keep the patient in a relaxed state without muscle contractions, moving the patient around various axes in the anatomical area (passive movement).
After taking the medical history, if no contraindications (severe trauma, loss of consciousness, etc.) are found, it is best to start with the “active movement” examination. This is because during active movement examination, the patient will voluntarily stop or refuse further activity when symptoms worsen. In contrast to active movement, passive movement examination will significantly increase the range of motion. Through these two methods of examination, the doctor can clearly understand the condition of the joint’s range of motion (such as severity, fractures, dislocations, somatization symptoms, symptom exaggeration, etc.).
MCP or PIP/DIP Joint Flexion
1. The patient sits; forearm in pronation; upper limb supported on the treatment table; wrist and hand in a neutral position.
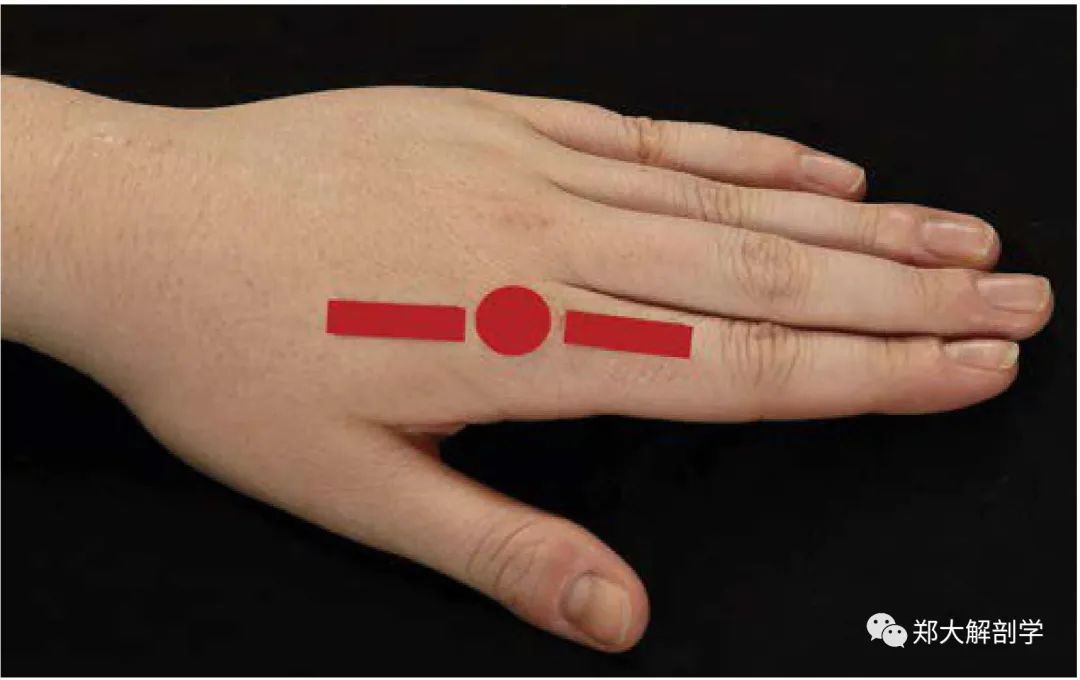
Measure the starting position of MCP flexion. The red line and dots indicate the alignment markers of the goniometer (the dorsal midline of the metacarpal, the dorsal side of the MCP joint, the dorsal midline of the proximal phalanx).
2. Keep the metacarpal stable.
3. Instruct the patient to perform the required movement, checking the flexion of the MCP joint through the achievable ROM.
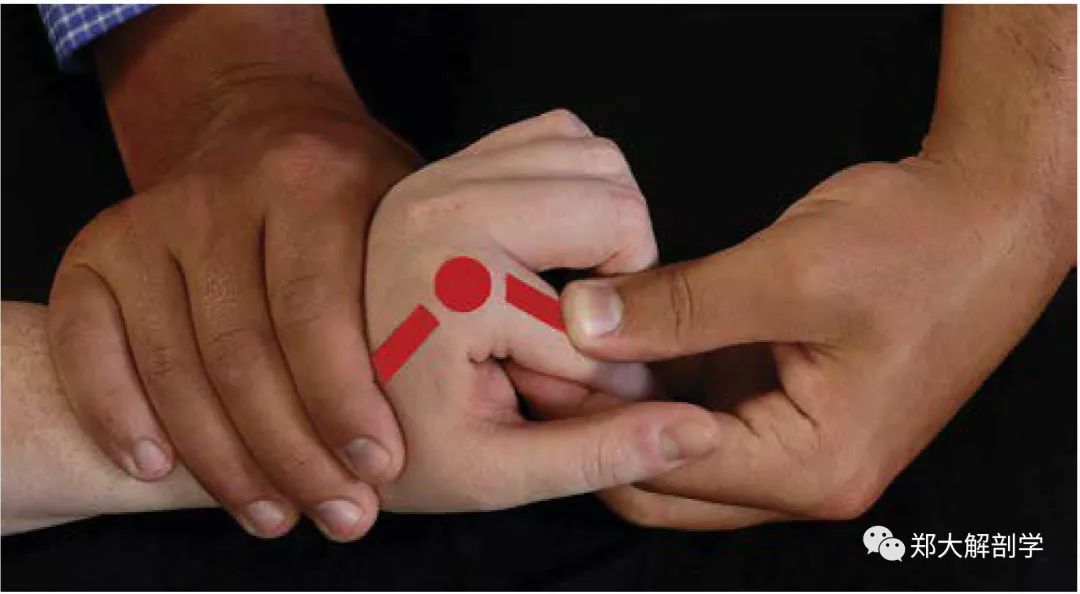
The MCP flexion ROM ends, showing the appropriate hand placement to stabilize the metacarpal and flex the MCP joint. The red line and dots indicate the alignment markers of the goniometer (the dorsal midline of the metacarpal, the dorsal side of the MCP joint, the dorsal midline of the proximal phalanx).
4. After completion, return the limb to the starting position.
Normal ROM: MCP = 80°~100°
[Course Guide] Pain Physical Examination and Anatomical Analysis
This series of courses has a total of 30 lectures.
Original price 99, limited-time group price 29.9, limited-time group leader free
Supports permanent re-listening.
Get more exciting content (scan the code).
Consultation phone: 13027515195 (same number as WeChat)