Introduction
The 27th Annual Congress of the Chinese Rheumatology Association (CRA) was successfully held in Wuhan, Hubei from August 8-10, 2024. On this occasion, the Rheumatology and Immunology Department of Yiyao Tong has closely followed the academic frontier and dedicatedly created the “New Knowledge in Rheumatology” medical column, aiming to provide professional and cutting-edge medical information to a wide range of doctors, to discuss the latest developments in the diagnosis and treatment of rheumatic and immune diseases, and to promote the development of this field.
During this conference, Professor Dai Lie, the head of the Rheumatology and Immunology Department at Sun Yat-sen University Sun Yat-sen Memorial Hospital, delivered an excellent lecture on “Diagnosis and Differential Diagnosis of Crystal Arthropathies.” Here, Yiyao Tong has organized some of the content for readers.
Common crystals that cause crystal arthritis include monosodium urate (MSU) crystals causing gout, calcium pyrophosphate (CPP) crystals causing pseudogout, and basic calcium phosphate (BCP) crystals causing calcific periarthritis. Additionally, cholesterol crystal arthritis and steroid crystal arthritis can also be observed clinically. Crystal analysis of the patient’s synovial fluid and synovial tissue can assist in clinical diagnosis.
Gout
-
Directly related to hyperuricemia caused by purine metabolism disorders and/or reduced uric acid excretion
-
The clinical pre-stage is asymptomatic hyperuricemia and/or MSU crystal deposition
-
The clinical stage manifests as recurrent acute arthritis, tophi, and chronic gouty arthritis
-
Usually presents as acute monoarthritis, commonly seen in the first metatarsophalangeal joint, midfoot, ankle, and knee joints
-
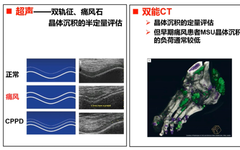
For patients suspected of gout attacks, evidence of crystal deposition needs to be sought, including synovial fluid analysis, ultrasound, and dual-energy CT

Q
In the diagnosis of gout, is synovial fluid crystal analysis necessary for symptomatic patients?
The 2023 EULAR imaging guidelines for the diagnosis and treatment of CiAs indicate that when characteristic manifestations of MSU deposition are identified on ultrasound (i.e., double contour sign or tophi) or DECT, gout can be diagnosed without synovial fluid analysis.
-
Although evidence of MSU deposition in synovial fluid or tissue analysis remains a diagnostic hallmark, it may not always be feasible due to unsuccessful joint aspiration or lack of facilities/expertise for analyzing joint fluid.
-
However, as a general rule, joint aspiration should always be attempted whenever feasible, especially to exclude other causes of acute arthritis, such as septic arthritis, regardless of whether there is previous evidence of gout (e.g., DECT positive and hyperuricemia).
-
Gout may coexist with septic arthritis or CPPD, which again requires synovial fluid to exclude/confirm differential diagnoses.
-
Imaging findings should be interpreted with care, considering that they are not completely specific (i.e., the double contour sign is a typical feature of gout but may be present in CPPD and asymptomatic hyperuricemia).
Calcium Pyrophosphate Crystal Deposition Disease (CPPD)
-
CPP crystal deposition (CPPD): refers to the presence of CPP crystals, which can be detected by microscopy or imaging
-
CPP can deposit in joint cartilage and synovium, ligaments, and surrounding tissues
-
The most common deposition sites for CPP are the knee and wrist joints, with other sites including the pubic symphysis, hip joint, and metacarpophalangeal joints
-
CPPD disease: indicates the presence of symptomatic arthritis
-
Chondrocalcinosis: refers to the radiological examination showing calcification of hyaline cartilage and/or fibrocartilage
-
This lesion is common in CPPD disease but is not an absolute specific lesion of CPPD, nor is it a common manifestation in affected patients.
-
During the progression of the disease, the manifestations of calcium pyrophosphate crystal deposition disease are diverse and heterogeneous.
-
Asymptomatic CPPD disease
-
Acute CPP crystal arthritis (pseudogout) – knee, wrist, shoulder, ankle
-
OA with CPPD, with or without superimposed acute attacks (pseudosecond OA) – knee, wrist, metacarpophalangeal, hip joints
-
Chronic CPP crystal inflammatory arthritis (pseudorheumatoid arthritis) – wrist, metacarpophalangeal, knee, and elbow joints, symmetrical
-
Severe joint degenerative lesions (pseudoneuropathic arthropathy)
-
Spinal involvement
1
Acute CPP Crystal Arthritis (Pseudogout)
➤ Exists in >25% of CPPD patients
➤ Commonly involves one or more large joints, with the knee and wrist being the most severely affected, and less commonly the MTP1
Over time, other joints may be affected
➤ Any joint may be involved, and polyarthritis may occur
➤ Typically presents as intermittent, acute, self-limiting, severe joint redness, swelling, and pain, with asymptomatic periods in between
➤ Patients often have systemic manifestations, including fever, leukocytosis, elevated ESR, and other acute-phase reactants
➤ It takes longer to reach peak intensity, and symptoms may persist for up to 120 days despite treatment
➤ Differential diagnosis: infection, trauma, hemorrhage, and other crystal-related diseases (such as gout), further synovial fluid analysis can assist in disease differentiation.
2
OA With CPPD (Pseudosecond OA)
➤ Is a common chronic manifestation of calcium pyrophosphate crystal deposition disease
➤ A large portion of CPPD patients have degenerative arthritis
➤ Affects joints similar to OA
➤ Commonly involves the knee, wrist, MCP, hip, and shoulder joints, presenting as gradually onset pain and slowly progressive joint destructive inflammatory symptoms, with morning stiffness and synovitis being rare
Half of the patients will have superimposed acute arthritis attacks
➤ Differentiation from OA:
-
The affected joints are usually not the typical joints involved in pure OA patients
-
When occurring in the knee joint: primary OA is more common in the medial compartment, leading to varus deformity; OA with CPPD or elderly pseudosecond OA is more likely to affect the lateral compartment and lead to valgus deformity;
-
Significant degenerative joint lesions usually have calcification of cartilage as a preceding manifestation
3
Chronic CPP Crystal Inflammatory Arthritis (Pseudorheumatoid Arthritis)
➤ Manifestations are similar to RA: significant morning stiffness, fatigue, synovial thickening, localized edema, and restricted joint movement caused by active inflammation or flexion contracture
➤ Affects multiple joints – peripheral joints of the upper and lower limbs
-
Including wrist joints, metacarpophalangeal joints, knee joints, and elbow joints
➤ Symmetrical or nearly symmetrical distribution
➤ Arthritis can last for months, and the inflammation of the affected joints often varies in severity and is unrelated
-
Multiple inflammatory joints usually flare up independently
➤ These episodes are usually self-limiting, often lasting from days to weeks
➤ Differentiation from RA:
-
In RA patients, multiple joint inflammation often occurs simultaneously and resolves
-
Compared to RA, chronic CPP crystal inflammatory arthritis has radiological changes more similar to OA, but the clinical manifestations of the affected joints are more like RA
4
Severe Joint Degenerative Lesions (Pseudoneuropathic Arthropathy)
➤ The imaging characteristics may resemble neuropathic joint destruction
➤ However, true neuropathic joint destruction is characterized by loss of joint position sense, occasionally accompanied by loss of other sensations (such as pain and temperature sense)
5
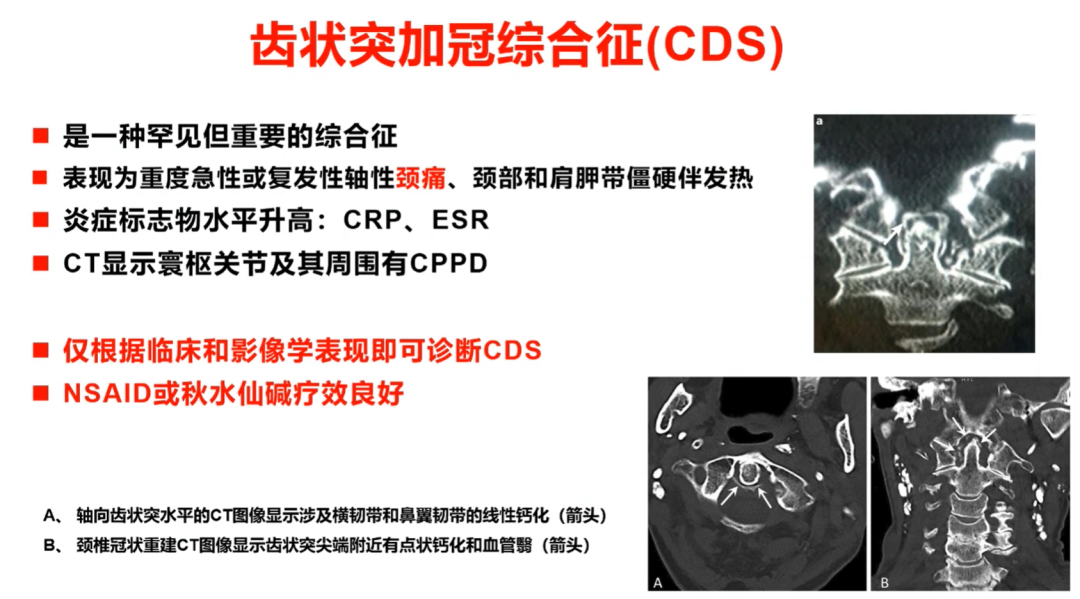
Spinal Involvement
➤ Clinical manifestations include spinal stiffness, sometimes leading to joint bony ankylosis, resembling spinal lesions of AS or DISH
-
This type of symptom is most common in familial CPPD disease
➤ Crystal deposition in the yellow ligament at the cervical level or lower posterior longitudinal ligament can lead to spinal cord compression syndrome or cause acute nerve compression symptoms or chronic spinal canal stenosis symptoms
-
The space-occupying effect caused by CPPD crystals and associated soft tissue accumulation must be differentiated from other calcified or ossifying space-occupying lesions
➤ Odontoid process plus crown syndrome (CDS)
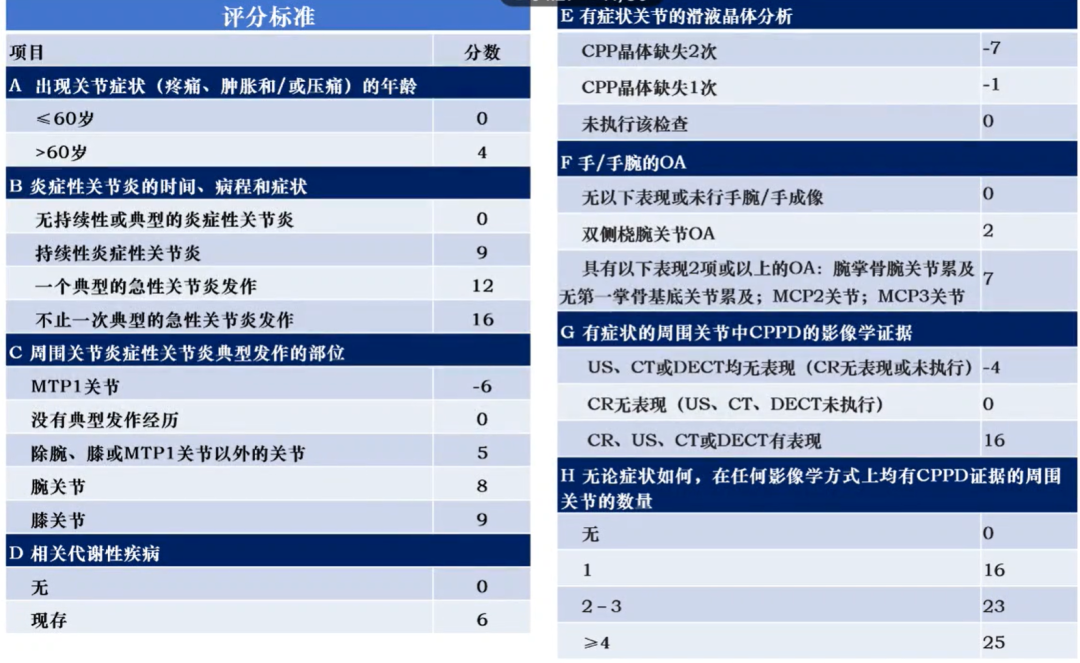
CPPD Scoring Criteria
BCP Crystal Arthritis
-
BCP crystalline-related arthritis (pseudopseudogout) and calcific periarthritis
-
Milwaukee Shoulder Syndrome (MSS)
1
OA With BCP Crystals (Pseudopseudogout)
➤ BCP crystals are a common manifestation of advanced large joint OA, indicating rapid progression to end-stage disease
-
The incidence of BCP crystal deposition in OA tissues is high
-
BCP crystals are found in up to 100% of end-stage hip and knee joint replacements, while CPPD crystals are only found in 18%
-
In knee joint replacements for OA, synovial fluid analysis shows BCP crystals in 47%, while CDDP only in 21%
-
CPP crystals often coexist with BCP crystals, and BCP-related arthritis typically progresses over months or years
➤ Routine laboratory tests: mostly normal
➤ Imaging: plain X-ray shows typical changes of severe OA
➤ Imaging examination is necessary for the diagnostic assessment of BCPD
➤ Routine radiological examination or ultrasound is recommended as the preferred imaging modality
-
Diagnosis based solely on clinical manifestations is difficult; BCP crystal analysis is very challenging, and the diagnosis of BCPD clearly relies on imaging diagnosis
-
CR or ultrasound may assist in the diagnosis of BCPD and may provide information about joint or periarticular involvement
-
The choice of technique mainly depends on availability
-
Ultrasound allows for more precise localization of BCP deposits, both in and around joint structures
-
CR usually provides comprehensive information about the joint as a whole
➤ Common sites: shoulder joint
2
Milwaukee Shoulder Syndrome
➤ Commonly seen in elderly women, non-inflammatory, shoulder-dominant, with significant non-inflammatory effusion, highly destructive, loss of function, with the dominant side being more severely affected in BCP crystalline-related OA-like arthritis
➤ Risk factors: history of shoulder joint trauma, history of overwork, advanced age
➤ Examination may reveal significant cold effusion in the glenohumeral joint, crepitus, and joint instability
➤ Synovial fluid analysis:
-
Non-inflammatory, white blood cell count <1000/mm3
-
BCP crystals strongly stained with alizarin red S, while CPP crystals are weakly stained
➤ Routine laboratory tests: mostly normal, inflammatory markers not elevated
➤ Significant glenohumeral joint degeneration and soft tissue calcification
-
Rotator cuff injury presents as “high riding” humeral head, with common erosion of the coracoid and acromion, and humeral neck may also show erosion, with extensive destruction of joint cartilage, thus rarely showing chondrocalcinosis
-
MRI: may show the extent of associated tendon and ligament damage
-
Ultrasound: may show tissue damage and presence of significant joint effusion
Information Source: Dai Lie. Diagnosis and Differential Diagnosis of Crystal Arthritis. 2024 CRA. August 9, 2024.
