
The complement system is a component of innate immunity. It plays an important role in defending against pathogenic infections, participating in immune regulation, and maintaining internal environmental stability; however, abnormal activation of the complement system can also cause self-damage, leading to diseases. The kidneys are one of the organs most easily affected.
From August 1 to 4, 2024, the Chinese Physician Association Nephrology Physician Branch (CNA) 2024 Academic Annual Conference was grandly held in Taiyuan. In the renal and cardiovascular theme session, Professor Fu Ping from West China Hospital of Sichuan University delivered an excellent report titled “Complement-Related Kidney Disease”. DXY has summarized its essentials for readers.
1. Overview of Complement-Related Kidney Disease (CMKD)
1. The Complement System and Its Components
Professor Fu Ping introduced that the complement system consists of more than 50 types of plasma proteins and membrane proteins, including complement inherent proteins, complement receptors, and complement regulatory proteins. Complement activation includes three pathways: the classical pathway, the lectin pathway, and the alternative pathway.
All pathways form C3 and C5 convertases, which then produce the main effectors of the complement system:
– Anaphylatoxins (C3a/C5a): play an inflammatory role
– Opsonins (e.g., C3b): facilitate opsonization and phagocytosis
– Membrane Attack Complex (C5b-9, i.e., MAC): exert lytic effects
2. Abnormal Activation of the Complement System Causes Self-Damage
Professor Fu Ping pointed out that under physiological conditions, the activation and regulation of the complement are in a balanced state, playing an important role in immune surveillance and maintaining self-immune homeostasis; however, under pathological conditions, an overactive complement system can attack self-cells and tissues, leading to various inflammatory responses and autoimmune diseases.
Deficiencies or dysfunctions in complement regulation can lead to excessive activation of the complement system, becoming a driving or exacerbating factor for various inflammatory or autoimmune diseases; while excessive suppression of the complement can prevent the body from responding to external infectious damage or foreign antigens.
Factors leading to complement system imbalance include genetic mutations, gene polymorphisms, genetic defects, gene expression levels, autoantibodies, environmental factors, etc.
3. Special Structure, Kidneys Are Easily “Injured”
Professor Fu Ping stated that, on one hand, glomerular basement membrane (GBM) does not express complement regulatory proteins, and the expression of complement regulatory proteins CD55 and CD59 in glomerular endothelial cells is relatively low, and damage to the glycocalyx on the surface of endothelial cells and GBM also leads to complement activation.
On the other hand, the kidneys have abundant blood flow, resulting in high local complement concentrations, and changes in local pH can also affect complement activation. This leads to the generation of key complement activation products that cause damage, such as inflammatory factors C3a and C5a, and the formation of the membrane attack complex MAC, resulting in kidney injury.
4. New Consensus Recently Released
Professor Fu Ping introduced that the 2024 Chinese Expert Consensus on the Diagnosis and Treatment of Complement-Related Kidney Disease has been published, which is systematic and comprehensive, covering CMKD classification, detection, vaccines, and the pathogenesis and targeted treatment evidence and recommendations for different CMKDs, providing normative references for the diagnosis and treatment of CMKD.
5. What Diseases Does CMKD Include?
Based on the different roles of complement in the pathogenic mechanism, it can be divided into kidney diseases directly mediated by abnormal activation of the complement system and kidney diseases involving the complement system.
– The former includes C3 glomerulopathy, atypical hemolytic uremic syndrome (aHUS), and immune complex-mediated membranoproliferative glomerulonephritis (IC-MPGN);
– The latter includes IgA nephropathy, anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), diabetic nephropathy, membranous nephropathy (MN), focal segmental glomerulosclerosis (FSGS), lupus nephritis, antiphospholipid syndrome, etc.
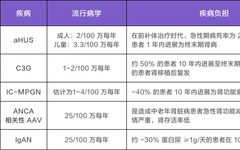
In common diseases like diabetic nephropathy and lupus nephritis, the involvement of complement in the pathogenic mechanism is still unclear; while several other CMKDs are relatively rare, often not widely recognized, and have acute conditions with poor prognosis. Professor Fu Ping introduced their epidemiology and disease burden as shown in Table 1.

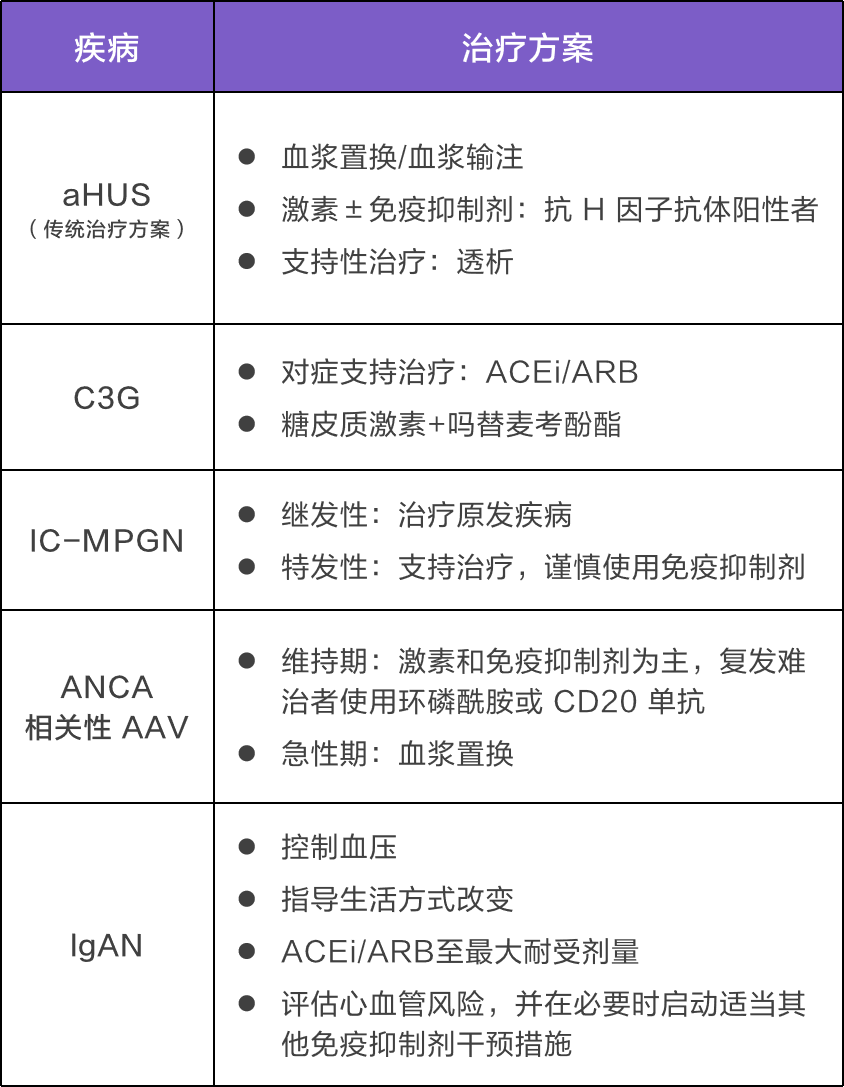
Meanwhile, the treatment needs for these relatively rare CMKDs are severely unmet, and previous treatments have mainly focused on non-specific treatments and symptomatic support (Table 2), with issues such as a lack of targeted treatment, insufficient remission rates, and significant long-term side effects.
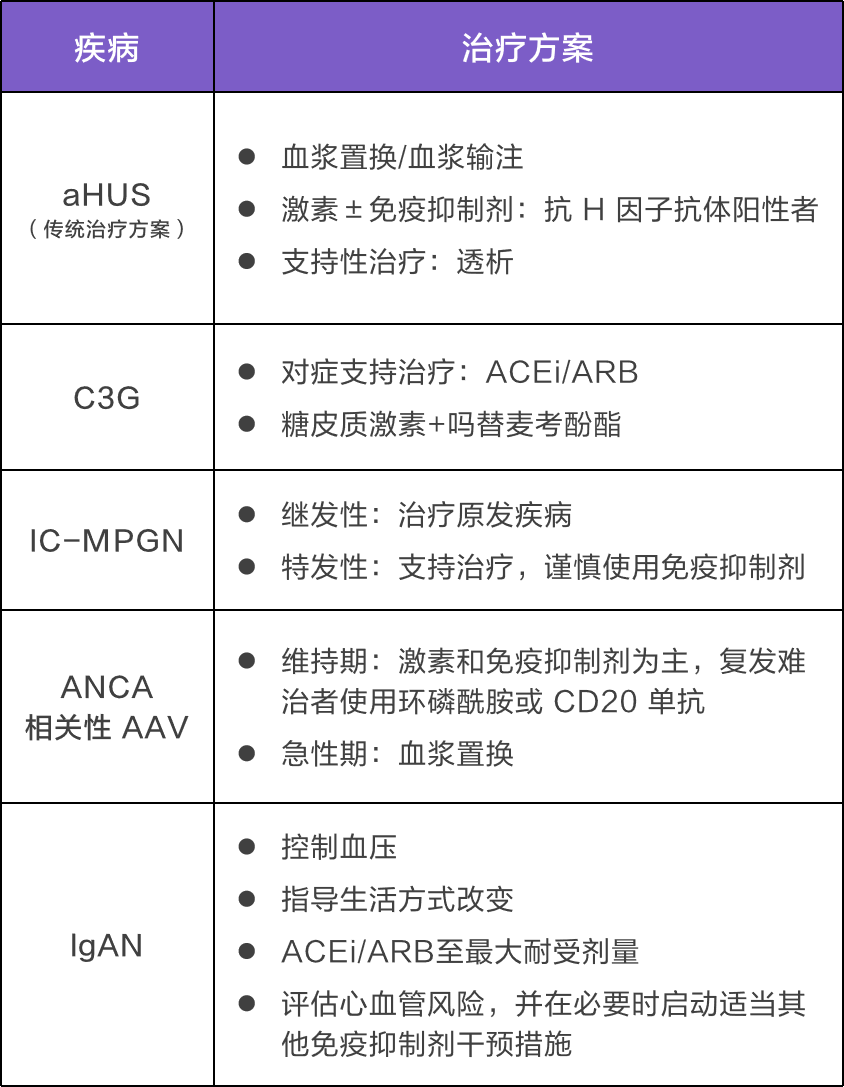
Note: ACEi – Angiotensin-converting enzyme inhibitors; ARB – Angiotensin receptor blockers
2. Pathogenic Mechanisms of Complement in CMKD
Professor Fu Ping introduced that in different complement-mediated kidney diseases, the pathways of complement abnormal activation vary. Overall, complement activation mainly proceeds through three pathways, which eventually converge into a common terminal pathway.
1. Diverse Mechanisms of Complement-Induced Kidney Disease
The mechanisms by which complement participates in glomerular diseases mainly include the following, with varying degrees and weights of complement involvement in different glomerular diseases:
– Deposition of complement components/activation products in the glomeruli: C3 glomerulopathy (C3G);
– Complement-mediated thrombotic microangiopathy (TMA): aHUS;
– Autoantibodies and immune complexes activating complement: IgAN, lupus nephritis, IC-MPGN, membranous nephropathy, anti-GBM antibody disease, cold agglutinin disease;
– Complement-mediated kidney inflammation: ANCA-associated vasculitis. In addition, complement activation, which is not limited to the glomeruli, may also lead to tubular and interstitial damage.
2. The Most Representative CMKD – aHUS
aHUS is the most representative CMKD, possibly caused by congenital/acquired abnormal regulation of the complement alternative pathway leading to uncontrolled abnormal activation of the complement alternative pathway (Figure 1).
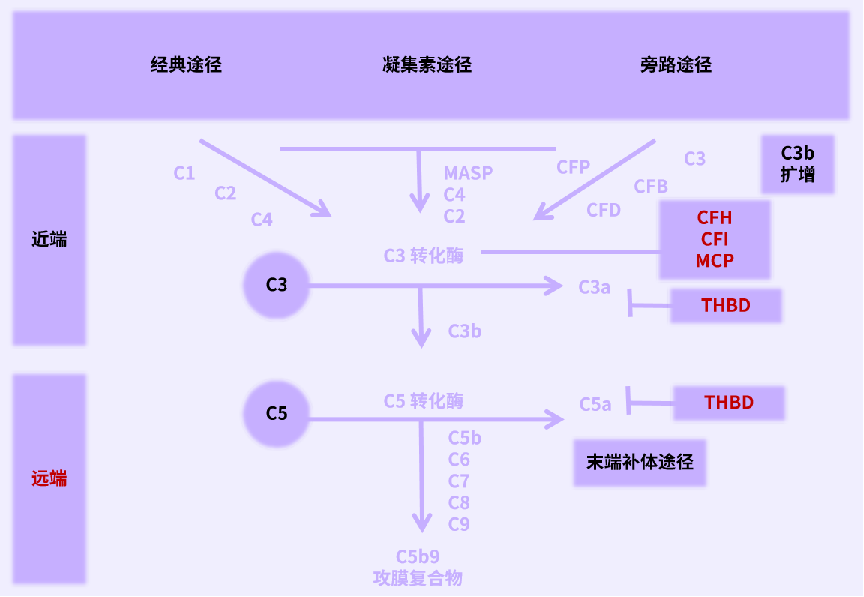
Figure 1 Pathogenesis of aHUS
Note: MCP – Membrane cofactor protein; THBD – Thrombomodulin; MASP – Serine protease
Professor Fu Ping stated that currently known genetic variations in complement are limited, and 30% to 50% of patients do not exhibit identifiable genetic variations, and TMA patients with unclear pathogenic mechanisms are also defined as aHUS.
Therefore, the diagnosis of aHUS is a diagnosis of exclusion, and after confirming TMA, aHUS can be diagnosed by excluding thrombotic thrombocytopenic purpura (TTP) and Shiga toxin-producing Escherichia coli-associated hemolytic uremic syndrome (STEC-HUS). After considering the diagnosis of aHUS, further complement-related gene, complement levels, function, and anti-complement antibody testing can be conducted for prognostic evaluation and to guide long-term treatment plans.
3. Other CMKDs
C3G is a newly defined classification of kidney disease, diagnosed solely based on immunofluorescence results from kidney biopsy. It typically refers to a group of conditions caused by excessive activation of complement leading to deposition of C3 in the glomeruli, including dense deposit disease (DDD) and C3 glomerulonephritis (C3 GN).
About 25% of C3G cases involve mutations in complement genes, such as those encoding C3, complement factor H, complement factor I, MCP, CFHR5, etc. 80% of DDD and over 50% of C3 GN patients have C3 nephritis factors (C3NeF) in their serum.
C3G and aHUS are both associated with congenital/acquired complement abnormalities, but C3G and aHUS have different sites of complement activation.C3G complement activation occurs in the liquid phase; aHUS complement activation mainly occurs on the endothelial surface.
Moreover, IC-MPGN has similar congenital/acquired complement alternative pathway abnormalities as C3G, and both may represent complement-mediated glomerular diseases.
In the pathogenesis of ANCA-associated AAV, there is also activation of the complement alternative pathway, and C5a is a key pathogenic component, forming a vicious cycle with neutrophils, ANCA, C5a, and the complement system in the progression of AAV.
IgAN primarily involves activation of the alternative pathway of complement, followed by the lectin pathway, with various complement protein levels and genetic variations associated with its occurrence, development, and severity, including increased deposition of glomerular C3, C4d, MBL, CFHR5, etc., abnormal circulating complement, and complement genetic anomalies, making complement a key pathogenic mediator.
For antiphospholipid syndrome, excessive activation of complement is involved in its occurrence and development; lupus nephritis involves activation of all three complement pathways; in other kidney diseases involving complement (such as MN, FSGS, and anti-GBM disease), specific antigens within the kidneys serve as targets for immune responses, leading to deposition of immune complexes that activate complement, exacerbating inflammation and tissue damage.
Additionally, in diabetic nephropathy, hyperglycemia activates the complement lectin pathway or causes CD59 to lose its inhibitory function.
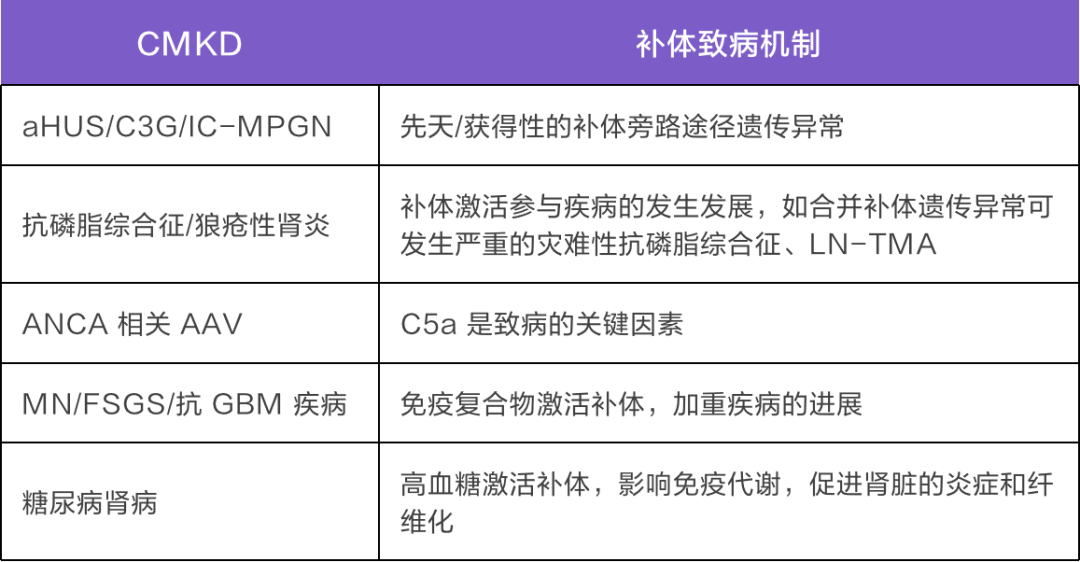
Professor Fu Ping concluded that the complement system is involved in the occurrence and development of various kidney diseases, and in different CMKDs, the pathogenic mechanisms of complement vary (Table 3). As the role of complement in kidney disease pathogenesis is uncovered, targeted complement therapy offers new possibilities for CMKD.
3. Application of Targeted Complement Therapy in CMKD
Currently, there are three drugs approved internationally for the treatment of CMKD, namely eculizumab, ravulizumab, and avacopan. Eculizumab has been approved in China for the treatment of adults and children with aHUS, while ravulizumab is approved abroad for aHUS treatment, and the small molecule C5aR inhibitor avacopan is approved abroad for AAV.
Professor Fu Ping introduced that in CMKD, targeted complement therapy has first achieved success in aHUS, currently C5 inhibitors are the first-line treatment for aHUS. Time is “kidney” life; consensus in China indicates that for adults with aHUS, eculizumab should be initiated as early as possible, with treatment lasting at least 6 to 12 months.
In the C08-002 study, for adult/teen aHUS patients, eculizumab showed rapid efficacy within 1 week, with a significant increase in platelet count by day 7 compared to baseline (P = 0.03), and within 2 years, 76% of patients showed sustained improvement in renal function; a real-world study in Japan indicated that after 1 month of eculizumab treatment, 57.1% of aHUS patients had improved serum creatinine (SCr decreased by ≥25%).
Notably, in studies where eculizumab treatment was initiated early (C10-003/C10-004/C08-002), approximately 80% to 83% of patients could discontinue dialysis after 26 weeks of treatment; in contrast, in the C08-003 study, no patients could discontinue dialysis when treatment was delayed; indicating that earlier initiation yields greater benefits. Additionally, a 2019 study suggested that long-term use of eculizumab for TMA reduces the risk of recurrence by 93%.
Of course, there are other complement inhibitors targeting the terminal complement pathway that are worth looking forward to, and Professor Fu Ping summarized them for us (Table 4).

Note: Drug clinical development stages based on the research status published on Clinical trial.gov, access date 2024-2-23
4. Summary and Outlook
At the end of the lecture, Professor Fu Ping summarized that traditional treatment methods for complement-mediated kidney diseases mainly focus on non-specific treatments, with limited therapeutic options, and targeted complement therapy offers new ideas and hopes for complement-mediated kidney diseases.
Currently, the application and research status of complement inhibitors in complement-related kidney diseases include: (1) aHUS: Complement C5 inhibitors are the first-line treatment choice, which should be initiated immediately upon diagnosis to rapidly and sustainably improve hematological abnormalities and renal function in aHUS patients; (2) ANCA-associated AAV: The main pathogenic factor is C5a, and there are already approved C5aR inhibitors abroad; (3) C3G/IC-MPGN/LN/IgAN/MN: Various complement inhibitors targeting different sites are under investigation.
Overall, the pathological roles of complement in different CMKDs vary, necessitating in-depth exploration of complement-related pathogenic mechanisms and selection of suitable targets for complement inhibitory therapy.
Compiled by | Kong Qing
Reviewed by | Professor Fu Ping
Submission | [email protected]
Cover Image | Zcool Hailuo