Acid etching technology is widely used in dentistry (involvement in caries, restoration, orthodontics, etc.), and any content related to resin bonding often involves this concept. Since it is closely related to bonding, discussing acid etching inevitably leads to the mention of bonding technology.
First, let us understand the development history of acid etching adhesives:
|
Type of Etching |
Components |
Bonding Strength |
Clinical Products |
|
|
1st to 3rd Generation |
Total Etching |
Too many details to list individually. Specific content can be referenced in related literature. |
2-7 MPa, relatively low |
Currently mostly discontinued |
|
4th Generation |
Total Etching (Two components, mixed before use) (Multiple bottles and steps) (First mix with 35-37% phosphoric acid total etching agent to treat the tooth surface) |
35-37% phosphoric acid etching + primer (N-phenylglycine acid-glycerol methacrylate resin, etc., carrier is acetone or water) + adhesive (HEMA hydroxyethyl methacrylate or UDMA dimethacrylate, etc.) |
17-25 MPa |
3M: Scotchbond Ivoclar: Heliobond Kuraray: Clearfil Photo Bond Kerr: Optibond |
|
5th Generation |
Total Etching (Single bottle) (Requires mixing with 35-37% phosphoric acid total etching agent to treat the tooth surface) |
Primer and adhesive mixed into a single bottle adhesive |
20-25 MPa |
3M: Adper Single bond plus Ivoclar: Syntac Kuraray: Clearfil Liner Bond Kerr: Optibond Solo Heraeus: Gluma Comfort Bond Denstply: Prime & Bond Kerr: Optibond Solo |
|
6th Generation |
Self-Etching (Two bottles two-step method) (Stepwise application) |
Treatment agent is one bottle: (Self-etching agent + coupling agent) + adhesive in another bottle |
18-25 MPa |
Ivoclar: Adhese Kuraray: Clearfil SE Bond GC: Unifil Bond Kerr: Optibond Solo Plus SE |
|
Self-Etching (two bottles one-step method) (two components mixed and applied simultaneously) |
Component 1; Component 2: |
18-25 MPa |
Denstply: XENO Ⅲ 3M: Adper Prompt L-Rop |
|
|
7th Generation |
Self-Etching One-Step Method |
(Self-etching agent + coupling agent + adhesive) mixed into one bottle |
Heraeus: I-Bond GC: G-Bond Denstply: XENO Ⅳ |
In my clinical work, the commonly used adhesives are: 3M total etching Single bond system and Kuraray self-etching SE-Bond system.
Generally, for dead pulp teeth with extensive enamel and dentin defects, I often use the method of total etching of enamel and dentin: 37% phosphoric acid etching of enamel for 60 seconds + 3M Single bond + resin filling, mainly considering that the total etching effect on enamel is relatively more certain;
For vital pulp teeth, I usually use the method of 37% phosphoric acid etching of enamel for 30 seconds + self-etching of dentin (Kuraray SE-Bond) for 20 seconds + resin filling, mainly considering that self-etching has advantages over total etching in reducing postoperative sensitivity.
Next, we need to introduce two “well-known” professional terms: “Total Etching Bonding System” and “Self-Etching Bonding System“.
-
What is total etching? What is self-etching? How are they distinguished?
-
Are they aimed at enamel or dentin? Or both?
-
What are the criteria for choosing specific etching methods in clinical practice? Or in what situations are they applicable?
-
How to grasp the etching time? What details should be noted during bonding after etching?
-
How to control the moisture during dentin wet bonding? How to measure the thickness of the adhesive?
-
What theoretical support is behind all the clinical operation points?
Next, we will explain:
Total Etching Bonding System: The total etching theory was first proposed by Fusayama et al. in 1979, which involves using an etching agent to treat both enamel and dentin simultaneously, completely removing the contamination layer, and forming a demineralized layer of 3-5μm on the dentin surface. Then, a primer is applied to improve the wettability of the dentin surface, allowing the adhesive to penetrate into the demineralized collagen fiber network, forming an entangled mixed layer that serves as a transitional structure connecting the restorative resin and dentin. The mixed layer and the resin protrusions penetrating into the dentinal tubules provide retention, but the mixed layer plays the main role in retention.


After cutting dentin, the longitudinal section of dentin shows the presence of contamination layer plugs in the dentinal tubules (magnification 2000)
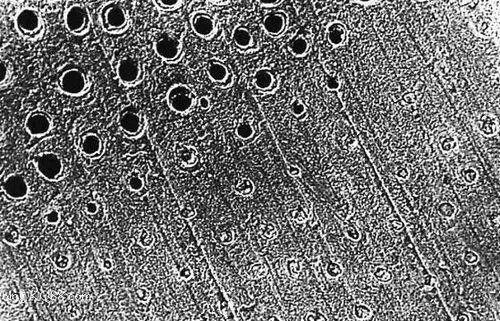
The upper part of the dentin in the image has been completely washed after being treated with 37% phosphoric acid etching for 15 seconds, showing that the contamination layer has been removed (magnification 1000)

Longitudinal section of dentin. The peritubular dentin has been removed, exposing the intertubular dentin collagen fibers (magnification 5000)
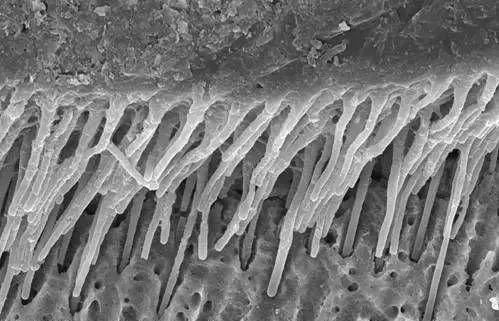
The image shows resin protrusions (magnification 1500)
Self-Etching Bonding System: This involves mixing acidic functional components and coupling agents together, allowing demineralization of the tooth surface and coupling to occur simultaneously, omitting the independent etching step. Specifically, the acidic functional components dissolve the minerals in the contamination layer and cause superficial demineralization of the underlying dentin, but they do not remove the contamination layer. During the formation of a hybrid layer with the resin monomers that penetrate the contamination layer, they also mix with the self-etching components in the dentinal tubules to form plugs, becoming part of the resin protrusions, thus achieving the purpose of bonding resin to dentin. Initially, this was limited to dentin bonding, but later it developed to function on both enamel and dentin.
The self-etching bonding system can be divided into the following two categories based on its components and clinical operation steps:
A. Single component: self-etching agent + coupling agent + adhesive combined into one
B. Two components: treatment agent (self-etching agent + coupling agent) + adhesive or self-etching agent + (coupling agent + adhesive)
The Kuraray SE-BOND from Japan is a two-component self-etching bonding system [treatment agent (etching agent + coupling agent) + adhesive]

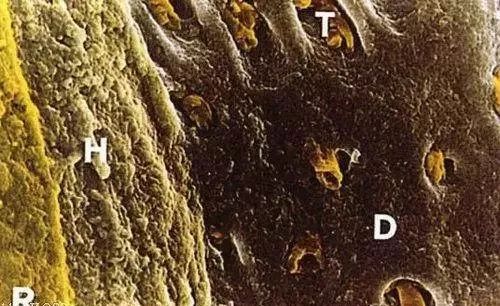
Composite resin interface replication model (magnification 2000). Note: T, resin protrusion; H, mixed layer; D, dentin; R, composite resin
Dentin section: resin enters dentinal tubules (magnification 2000)
From the descriptions of these two terms, it can be seen that both total etching bonding and self-etching bonding can work on both enamel and dentin (regarding the effectiveness, current academic research is flourishing, and it is up to us to discern which viewpoints are mainstream or more convincing), but it can be seen that the main difference between the two bonding systems lies in whether the contamination layer is removed.
Thus, the contamination layer plays a significant role in the bonding process. Additionally, we see the emergence of other important concepts, such as etching agents, acidic functional components, treatment agents, coupling agents, primers, adhesives, mixed layers, hybrid layers, resin protrusions, wettability… What are the specific definitions of these concepts? How are they related? Is there any overlap or confusion among them? Let us explain them one by one.
What is the contamination layer?
It is the layer produced on the surface when cutting or grinding dentin, composed of cut dentin collagen fibers, demineralized amorphous crystals, moisture, and some other substances.
What are the two types of etching agents?
What are their components?
A. Total etching agent: 35-37% phosphoric acid
B. Self-etching agent: Its functional components mainly include two types, one being unsaturated or polymerizable organic acids or acidic groups as functional components of methacrylate resin monomers; the other involves adding organic acids or inorganic acids, such as maleic acid, to non-acidic hydrophilic resin monomers. Compared to 37% phosphoric acid, it has weaker and gentler acidity.
What is the treatment agent commonly mentioned in self-etching bonding systems?
What is a coupling agent?
Are the coupling agent and primer the same substance?
What does primer mean?
Most manufacturers produce self-etching treatment agents that include self-etching agents and coupling agents, referred to as treatment agents to distinguish from total etching agents. Some manufacturers mix the coupling agent with the adhesive component into one bottle, while the treatment agent component is the etching agent, in which case referring to the etching agent is clearer.
A coupling agent is a substance with two different functional groups, where one part of the functional groups in its molecule can react with organic molecules, while the other part can react with the adsorbed water on the surface of inorganic materials to form a strong bond. The role of coupling agents in composite materials is to react with certain groups on the tooth surface and with the resin matrix, forming an interface layer between the tooth surface and the resin matrix that can transmit stress, thereby enhancing the bonding strength between tooth tissue and resin, improving the performance of the composite material, and preventing other media from penetrating the interface.
According to the chemical structure and composition of coupling agents, they can be divided into four categories: organic chromium complexes, silanes, titanates, and aluminum compounds. Coupling agents used in composite resin fillings are mostly titanates, with HEMA (hydroxyethyl methacrylate) being a representative. It can wet the dentin matrix to facilitate the penetration of bonding resin and can act as a co-solvent for some poorly soluble monomers. It can also penetrate deep into the hybrid layer to form chemical contact, generating hydrophilic hydroxyl groups that bond with exposed collagen fibers, while hydrophobic methacrylate can co-polymerize with the bonding resin. The solvents in coupling agents can be either water or organic solvents, with the main organic solvents currently being acetone and ethanol.
My understanding: the coupling agent acts like a “hand-in-hand” role, with one hand holding the hydrophilic collagen fibers of dentin and the other holding the hydrophobic adhesive. That is, guiding and connecting.
Regarding whether the primer and coupling agent are the same meaning, I have consulted several peers and have not reached a definitive answer. The information I have found is also mixed. My feeling is that the primer appeared before the self-etching bonding system became popular and mainly targeted enamel, so it seems more appropriate to refer to it as enamel bonding agent; however, later in clinical operations, most did not separate enamel bonding and dentin bonding, and its role is similar to that of the coupling agent mentioned in self-etching, thus for dentin bonding, the meaning of primer is similar to that of coupling agent.
However, there are some clinicians who often confuse it with treatment agents, which I think is related to the translation of the English word “primer”. In English-Chinese dictionaries, primer can be translated as primer, treatment agent, bottom coat, etc. In fact, most treatment agents are mixed components of self-etching agents and coupling agents. In the current stage where self-etching is prevalent, the term primer is rarely mentioned.
What is wettability?
The tendency of a liquid to spread on a solid surface is called the wettability of the liquid to the solid, and wetting is a necessary condition for bonding.
What are the histopathological definitions of mixed layer and hybrid layer?
Mixed Layer: Dentin treated with total etching agent (after removal of contamination layer) allows the adhesive to penetrate into the demineralized collagen fiber network, forming a mixed layer.
Hybrid Layer: Dentin treated with self-etching treatment agent, where the unremoved contamination layer and the resin monomers penetrating into the demineralized dentin beneath the contamination layer form a hybrid layer.
To fully understand these concepts, we must revisit the histological structure of enamel and dentin:
Enamel
Physical and Chemical Composition: 96-97% inorganic matter (hydroxyapatite), 3% organic matter and water
Histological Structure: Enamel prisms
Dentin
Physical and Chemical Composition: 70% inorganic matter (hydroxyapatite), 20% organic matter (mainly collagen), 10% water
Histological Structure: Dentin tubules (with odontoblast processes and tissue fluid within the tubules), intercellular matrix (peritubular dentin, intertubular dentin, and interglobular dentin)
The following images show three cases of vital pulp deep caries (already lined), proposed for direct resin restoration. Clinically, there are generally three operational methods. I wonder which one you prefer? What is the reason?
Simultaneous total etching of enamel and dentin: (This method has been questioned due to postoperative sensitivity, but in recent years, with the development and application of indirect pulp capping agents and lining materials, as well as trust in the effectiveness of total etching, some doctors still support this method.)

Simultaneous self-etching of enamel and dentin (this method is adopted by most clinicians, mainly for its simplicity and convenience)
Full etching of enamel followed by self-etching of dentin (currently, this treatment method is widely recognized and advocated)

What is dentin wet bonding?
Resin filling can be said to be a treatment project that every dentist performs daily, but the long-term effects of the filled teeth are often unknown (such as marginal sealing, filling strength, incidence of secondary caries, etc.).
The loss of cases, incomplete data, etc., are important reasons why we cannot draw efficacy evaluations, but another important reason I believe is the inability to compare or the difficulty of comparison, that is, the inclusion criteria for cases cannot be consistent. The diagnoses are the same, but the treatment operations cannot be consistent, meaning that the operational details cannot be standardized, especially in controlling moisture and thickness.
Indeed: dentin wet bonding can be said to be “easy to say but hard to do”. The theory of dentin wet bonding was proposed by Kanca in 1992, mainly stating that:
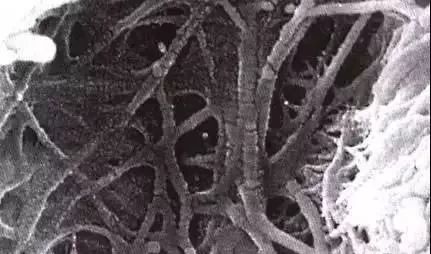
Moisture helps maintain the expanded state of the dentin collagen fiber network, opening the micropores, which is conducive to the penetration of resin. Scanning electron microscopy shows that excessively dry dentin surfaces will show shrinkage and collapse of the collagen fiber network, which is not conducive to the penetration of adhesive resin monomers, thus failing to achieve mechanical retention. Therefore, the amount of moisture retained is crucial; excessive wetness or dryness can lead to a decrease in bonding strength.
Expanded state
Shrinkage and collapse state
Thus, “dentin wet bonding” mainly refers to the total etching technique that removes the contamination layer, fully exposing the collagen fiber network, and relies on the adhesive penetrating into the collagen fiber network and working together with the resin protrusions embedded in the dentinal tubules to achieve retention.
Self-etching, due to its use of a milder etching agent, does not directly remove the contamination layer but modifies it, and the coupling and demineralization occur simultaneously, achieving bonding through the formed hybrid layer and resin protrusions. In other words, self-etching does not fully expose the collagen fiber network, so there is no need to maintain the expanded state of the dentin collagen fiber network, and thus “wet bonding” is not applicable.
Moreover, because of this, self-etching has reduced operational dependencies compared to total etching, simplifying clinical operation steps, which is also an important reason why self-etching bonding systems have been widely used in recent years.
“Wet bonding” is specific to total etching, does this mean that self-etching can ignore the importance of the moisture state of the dentin surface treated with the treatment agent?
Generally, before using the treatment agent, the amount needed should be considered based on the area of the cavity surface, with the aim of ensuring that the surface after active application is genuinely “treated” rather than just “skimming the surface” or “overly aggressive”. Because although self-etching does not require special “wet bonding”, it does not mean that the quantity of the treatment agent has no impact on bonding strength; it just means that it does not affect the expansion and shrinkage of the collagen fiber network.
What kind of moisture is considered appropriate moisture?
What methods can help us control moisture during clinical operations?
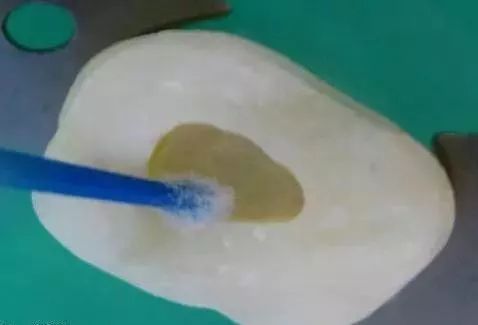
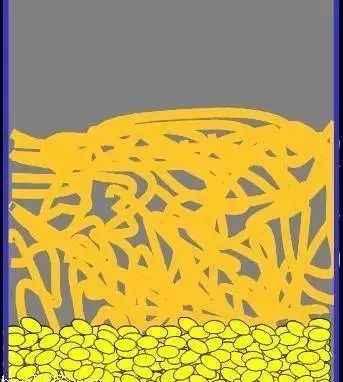
How to define appropriate “moisture”? Perhaps the following image will help us to understand it vividly:

My understanding of “appropriate moisture” is: moist but not flowing, wet but not soaked.
Below are some images from a recent case of resin filling after root canal treatment lining, showing total etching and wet bonding operational processes:


Specific operational process:
1. Enamel and dentin are first etched with 37% phosphoric acid for 60 seconds, then thoroughly rinsed with plenty of water, and a suitably sized and tensioned cotton ball is placed in the cavity (avoiding covering the enamel edge as much as possible). The filling instrument is then pressed lightly in the center of the cotton ball, and finally, an air gun (oil-free compressed air) is used to gradually blow air around the cotton ball (along the enamel edge) until the demineralized enamel edge turns slightly chalky, then the cotton ball is removed, and the dentin part is checked to see if it has reached the state of “appropriate moisture” (moist but not flowing, wet but not soaked).
2. Finally, a bonding stick dipped in adhesive (which must contain a coupling agent, such as 3M Single Bond) is used to apply to all areas of the cavity (note to control the thickness of the adhesive, as the thickness of the adhesive affects not only the bonding strength but also the marginal sealing, etc.).
In my opinion, “appropriate thickness” can still be understood as “moist but not flowing, wet but not soaked”; it should neither be “puddled” nor “dry”. Finally, resin layering and polishing are performed.
The following images are still derived from the book “Recent Advances in Dental Restoration Science”, which will help us understand dentin wet bonding after total etching:
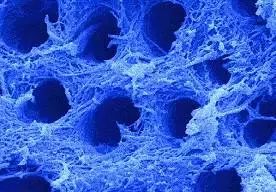
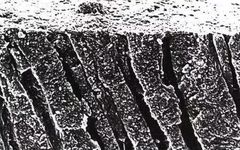
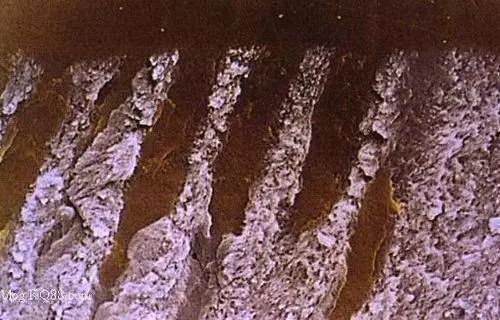
The image shows the dentin after total etching, with the intertubular dentin collagen fiber network fully exposed.
Magnified collagen fiber network (magnification 2000)
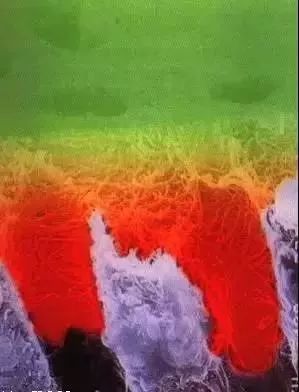
The following are some model images:

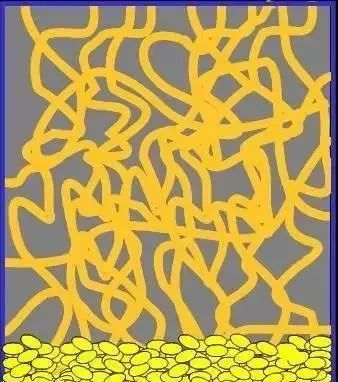
The image shows the dentin layer after etching, where the contamination layer has been removed, and both peritubular and intertubular dentin are demineralized, with collagen fibers exposed and rich in moisture. This dentin has high hydrophilicity and is very sensitive to dehydration. The blue color represents the moisture content of the calcium tissue structure.

The image shows the dentin layer after applying the primer. The hydrophilic resin (primer) has replaced the water in the collagen fiber network. The solvent of the primer can be organic (ethanol or acetone) or inorganic (water). Applying a water-solvent primer is a relatively slow process, while organic solvents replace water quickly (due to convection). After the evaporation of organic solvents, the resin surrounds the collagen fibers and hardens them, changing the dentin surface from hydrophilic to hydrophobic. The red color represents the area covered by the primer. (The above text is derived from the original text. Here, I believe the primer can be understood as a coupling agent. Before the emergence of fifth-generation adhesives, coupling agents were packaged separately and were often referred to as primers. Currently, the commonly used 3M Single Bond mixes the coupling agent with the adhesive into one bottle.)
 The image shows the dentin layer after applying the adhesive. The hydrophobic bonding resin penetrates into the dentinal tubules and fills the intertubular dentin. If the resin penetration is incomplete, areas of unfilled demineralized dentin will appear, lacking bonding resin protrusions. This defect can lead to poor dentin sealing and rapid degradation of the bonding interface.
The image shows the dentin layer after applying the adhesive. The hydrophobic bonding resin penetrates into the dentinal tubules and fills the intertubular dentin. If the resin penetration is incomplete, areas of unfilled demineralized dentin will appear, lacking bonding resin protrusions. This defect can lead to poor dentin sealing and rapid degradation of the bonding interface.

The image shows the dentin layer after polymerization of the bonding resin. The polymerized resin has completely penetrated the demineralized dentin, providing effective protection for the pulp-dentin complex.
“Etching and bonding” may seem like a routine operation in clinical practice, but achieving detailed “standardization and precision” is not an easy task, and fully understanding the profound theoretical support behind it requires a long journey…
• END • This article is sourced from the internet, copyright belongs to the original author. If there are any violations or infringements, please contact us, and our platform will respond promptly.
Previous Recommendations
1. 10,000 boxes of latex gloves for free! Dental Day clinic benefits, children’s toothpaste for 1 yuan, electric toothbrush for 9.9 yuan! 2. 35 dental projects not allowed in dental clinics? — Re-discussing the Shenzhen porcelain veneer penalty incident3.Another case of a 5-year-old girl “sealed eyes” entering ICU, which turned out to be caused by “teeth”.
Today’s Benefits Recommendation

Click Read the original text to discover more exciting content.