
Recent information regarding obesity:
-
Public Health Issue: The EU Defines Obesity as a Disease (2021) -
Clinical Practice: Obesity Management as a Primary Treatment Goal for Type 2 Diabetes with Obesity (2022) -
Guideline Consensus: Obesity and Weight Management for Diabetes Prevention and Treatment (2022 ADA Standards of Care) -
WE14 Notes: Obesity (2020) -
Guideline Consensus: 2020 Obesity: International Joint Consensus Statement to End Stigmatization
First Step (STEP)
Compiled by: Chen Kang
The unstoppable rise in obesity rates is a global issue, constituting one of the major public health challenges of the 21st century. Obesity and overweight lead to a range of comorbidities that affect the quality of life for millions of people. Weight gain and the desire to lose weight are the most common issues patients present to endocrinologists, and discussions often become difficult due to the lack of reliable weight loss programs. While dietary and lifestyle measures may be useful, maintaining success is challenging, and various known strategies only work for a small portion of people, clearly ineffective for many others with obesity. Weight loss surgeries have become increasingly sophisticated, safe, and effective, showcasing the health benefits of weight loss from another perspective. However, surgery is invasive, often incurs significant short-term costs, and given the severity of the obesity problem, it is difficult to promote on a large scale, especially now that obesity has become a public health issue faced globally. Until a few years ago, approved medications for weight loss had limited efficacy, with most affecting only a few percent of body weight and little evidence of lasting impact.
However, over the past few decades, the glucagon-like peptide-1 (GLP-1) system has been discovered and described, playing a physiological role in glucose homeostasis. Developing drugs that activate GLP-1 receptors (GLP-1R) is an important addition to diabetes therapeutics. An unexpected outcome of this work has been the demonstration that GLP-1 can reduce food intake and lead to weight loss. A series of reliable clinical trials now show that GLP-1 receptor agonists (GLP-1RA) can be specifically used to treat obesity, with effects significantly better than past medications, promising clinically meaningful weight loss effects for most individuals receiving treatment. This article focuses on this new application of GLP-1RA.
Scientific Basis for GLP-1 Weight Loss System
In the mid-1990s, the discovery of leptin and its receptor was a breakthrough in the convergence of metabolic and neuroscience fields, providing the most promising area for targeted weight loss treatment at that time. These compelling findings offered an easy entry point to link systemic metabolism with brain regulation, triggering a wave of research that led to the rapid definition and elucidation of key central nervous system (CNS) circuits controlling energy balance and nutritional homeostasis. As interest in leptin gradually waned, the role of the peptide produced in the gut—glucagon-like peptide-1 (GLP-1)—began to be described, and its ability to reduce food intake when utilized in the CNS of rodents was observed (Nature. 1996;379(6560):69-72). Looking back over the past 30 years, the scientific importance of leptin as a physiological mediator and catalyst of the neuroscience revolution is indisputable. However, leptin has never succeeded in becoming a predictor of weight loss in early preclinical studies. Instead, it is the GLP-1 system that, despite initially having lower persuasive and informative evidence regarding its actions in the central nervous system, subsequently produced meaningful drugs that may clinically impact weight and obesity.
The key components of the GLP-1 system are the gastrointestinal tract, central and peripheral nervous systems, and pancreatic islets (Mol Metab. 2019;30:72-130). The expression of the glucagon precursor gene is limited to specific intestinal enteroendocrine L-cells in the intestinal mucosa, a small group of hindbrain neurons, and the α-cells of the pancreatic islets; in each of these cell types, GLP-1 is cleaved from proglucagon. The expression of GLP-1 receptors (GLP-1R) is more widespread, but the main sites regulating food intake are the vagal afferent neurons as well as neurons in the hypothalamus and hindbrain (Mol Metab. 2022;57:101351). Recent preclinical studies support a model in which GLP-1 released from the gut mediates satiety via vagal nerve transmission (Cell Metab. 2021;33(7):1466-82 e7), while activation of hindbrain neurons has a parallel and independent effect on suppressing food intake (Nat Metab. 2021;3(2):258-273). However, unlike leptin receptors, the absence of GLP-1R does not cause obesity in mice (Endocrinology. 1998;139(7):3127-3132; Endocrinology. 2010;151(10):4678-4687), indicating that this system may not be essential for normal weight regulation. Although there are many sequence variants in the human GLP-1R gene, none are clearly associated with weight phenotypes (Cell. 2018;172(1-2):41-54.e19).
While there is still a prevailing view that GLP-1 released from the gastrointestinal tract stimulates insulin secretion via an endocrine mechanism, limited information indicates the influence of endogenous peptides on food intake. Experimental evidence from human studies using functional magnetic resonance imaging (fMRI) aligns with the activation of the CNS through circulating GLP-1 from exogenous or endogenous sources in a manner compatible with satiety (Diabetologia. 2015;58(12):2688-2698; Diabetes. 2014;63(12):4186-4196). Similar findings suggest that plasma GLP-1 has an enhanced effect on the CNS in individuals who have undergone weight loss surgery (Diabetes Care. 2017;40(11):1522-1529). Therefore, while more work is needed to confirm and deepen the understanding of the mechanisms, it can be demonstrated that GLP-1 is an endocrine component of human physiological satiety.
Although preclinical studies indicate that the physiological role of GLP-1 in regulating satiety is auxiliary rather than essential, pharmacological agonism of GLP-1R consistently reduces food intake and weight in both preclinical and human studies. Research volunteers treated with the GLP-1R agonist (GLP-1RA) exendin-4 (the first GLP-1 analog developed as a drug) consistently report decreased appetite, reduced food intake, and weight loss with prolonged use. Similar findings have been described in other GLP-1RA trials, where consistent weight loss was observed in subjects treated with exenatide, liraglutide, albiglutide, and dulaglutide. These drugs have much higher concentrations in circulation compared to endogenous GLP-1, and their effects may be mediated directly in the CNS. Based on preclinical research, GLP-1 receptors not only activate neurons in peripheral visceral organs accessible in circulation, such as the midbrain’s arcuate nucleus and the hindbrain’s area postrema, but can also reach the hypothalamic centers crucial for regulating food intake (J Clin Invest. 2014;124(10):4473-4488). Similar to studies with natural GLP-1, exendin-4 also alters specific neural activity on fMRI images in a manner indicative of satiety (Diabetes Care. 2016;39(10):1804-1810), with other GLP-1RAs also obtaining similar data. In summary, a compelling theory can be proposed that pharmacological GLP-1 receptors have a direct effect on the brain to suppress appetite and food intake.
Clinical research related to GLP-1R has advantages, which have pointed to the development and improvement of such drugs for the treatment of type 2 diabetes (Mol Metab. 2021;46:101102). However, the consistent effects of weight loss in diabetic patients included in clinical trials, combined with experimental evidence of the aforementioned mechanistic rationale, lay a solid foundation for advancing these drugs in trials specifically targeting weight loss in non-diabetic subjects. In recent years, results from these trials have been reported, bringing new hope to patients seeking weight loss and alleviation of the health burden of obesity.
Concept Validation Clinical Trials of GLP-1RA for Weight Loss in Non-Diabetic Populations
Exenatide is the commercial version of exendin-4, approved by the FDA in 2005 for the treatment of type 2 diabetes. Almost immediately, it was used off-label for weight loss in both diabetic and non-diabetic populations, often in conjunction with unvalidated dosing regimens. However, formal studies on GLP-1 RA for weight loss were not published until 2009 (Lancet. 2009; 374(9701): 1606-1616; Diabetes Care. 2010; 33(11): 2406-2408). Initial reports described a group of nearly 600 non-diabetic volunteers with a body mass index (BMI) of 30-40, who were randomly assigned to use orlistat or injectable placebo as a control vs. increasing doses of liraglutide. The two doses of liraglutide (2.4 and 3.0 mg) used in this trial were higher than the approved doses for diabetes treatment. During the 20-week active treatment period, the liraglutide-treated subjects experienced a dose-dependent weight loss greater than either control group. Additionally, gastrointestinal symptoms (nausea, vomiting, and diarrhea), which are hallmark side effects of GLP-1RA, were generally well tolerated, with frequency and severity comparable to those seen in trials of these drugs for diabetes; the incidence of nausea was dose-dependent but steadily decreased during the first 10 weeks of treatment. A second study randomly assigned 163 non-diabetic subjects with an average BMI of about 40 to receive exenatide or placebo (PBO) for 24 weeks, in the context of structured lifestyle intervention. In this study, the standard dose of exenatide resulted in a weight loss of 5.1 kg from baseline, compared to 1.6 kg with PBO, and this significant difference persisted for one month after treatment cessation. Notably, the weight loss in this relatively small study was on the higher side of the weight loss range observed in exenatide’s glycemic control trials in diabetic subjects. These two concept validation studies using liraglutide and exenatide laid the groundwork for longer trials that could better assess clinical efficacy.
The first large long-term study of GLP-1RA for weight loss was the Satiety and Clinical Adiposity-Liraglutide Evidence/SCALE trial, including SCALE Obesity and Prediabetes (N Engl J Med. 2015;373(1):11-22) and SCALE Diabetes (JAMA. 2015;314(7):687-699). The obesity and prediabetes trial was a multinational study designed to detect the efficacy of 3.0 mg liraglutide in non-diabetic patients with an average BMI of 38. After 56 weeks, patients in the liraglutide group lost an average of 8.4 kg compared to 2.8 kg in the PBO group. Almost all subjects in the liraglutide group (92%) lost weight, with the number of individuals losing 5% and 10% or more of their initial weight being three times that of the placebo-treated subjects. In the SCALE Diabetes trial, which included subjects with type 2 diabetes, liraglutide resulted in a weight loss of 6.4 kg compared to 2.2 kg in the placebo group, with 54% and 25% of subjects losing 5% or 10% of their initial weight, respectively. Adverse events in both trials (mainly gastrointestinal events) were similar to those observed in liraglutide’s glycemic control trials.
Semaglutide Clinical Trials
Semaglutide is the latest GLP-1RA drug approved in the US in 2017. Similar to liraglutide, semaglutide promotes the binding of fatty acyl side chains to albumin, thereby prolonging its residence time in circulation (Front Endocrinol (Lausanne). 2019;10:155). Due to differences in pharmacokinetics between the two drugs, semaglutide has a longer plasma half-life and is effective with once-weekly dosing. In fact, in clinical trials for glycemic control, semaglutide was shown to be more effective than liraglutide or dulaglutide in reducing hemoglobin A1c (HbA1c) and weight (Diabetes Care. 2016;39(9):1501-1509; Lancet Diabetes Endocrinol. 2018;6(4):275-286). Consequently, semaglutide was rapidly advanced into weight loss testing in non-diabetic subjects. The first of these studies compared multiple daily doses of semaglutide with 3.0 mg liraglutide in a population with a BMI > 30 kg/m2 (Lancet. 2018;392(10148):637-649). In this 52-week study, daily doses of semaglutide ranging from 0.05 to 0.4 mg resulted in a placebo-adjusted weight loss of 3.7%-11.5%, with effects at all doses except the lowest being greater than liraglutide (5.5%). Adverse events were similar to those described in many other GLP-1RA studies.
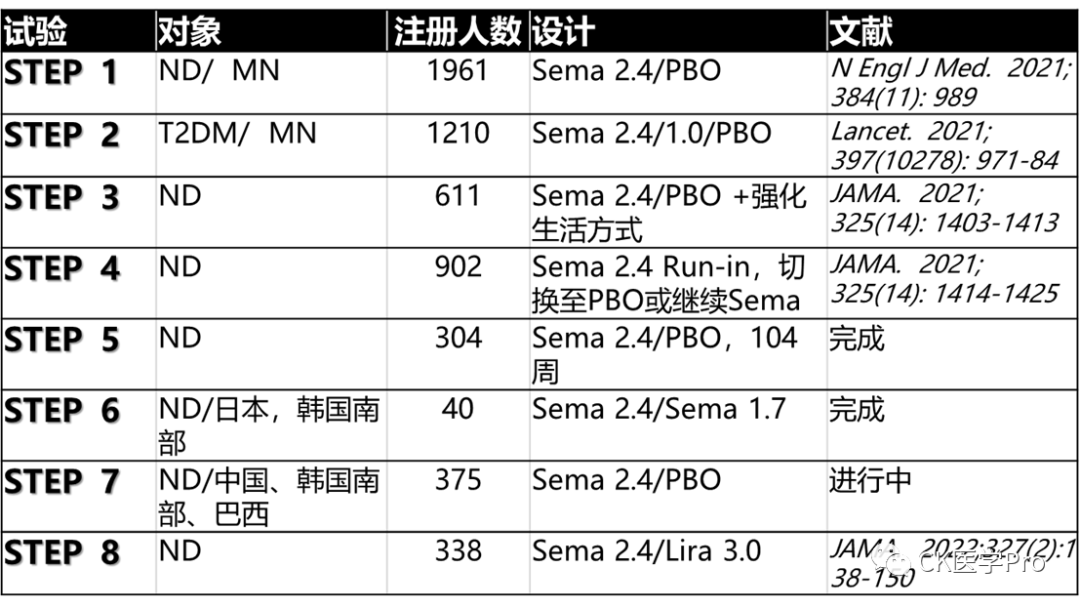
STEP (Semaglutide Treatment Effect in People with Obesity) is a series of phase 3 randomized clinical trials for semaglutide for weight loss, targeting populations with a BMI > 30. This project includes eight studies, each involving different subject groups or treatment regimens, all using subcutaneous semaglutide over 68 weeks. Except for STEP 3, all trials included similar lifestyle components, including 150 minutes of physical activity per week and a low-calorie diet (500 kcal/day), with the focus of the studies being on weight loss in non-diabetic adults; STEP 2 recruited participants with a BMI > 27 and type 2 diabetes. The primary outcomes of these studies followed standard outcome measures for weight loss trials, with the percentage of initial weight loss and the percentage of subjects losing 5% or 10% or more as key outcome indicators. Overall, the STEP trials published to date (Trials 1, 3, 4, and 8) have recruited over 3,700 non-diabetic subjects, with over 75% being female, a similar proportion of Caucasians, an average age of 46 years, and an initial weight of about 105 kg.
STEP 1 recruited over 1,900 adults, randomly assigned in a 2:1 ratio to receive either weekly 2.4 mg semaglutide or placebo (N Engl J Med. 2021;384(11):989). Although the inclusion criteria excluded a diabetes diagnosis, 43% of participants in STEP 1 had prediabetes, and over 75% had at least one comorbidity. The weight loss in the semaglutide group exceeded that observed in the SCALE trials, with an average change in weight of 14.9% compared to 2.4% in the placebo group. Over 80% of the semaglutide group lost at least 5% of their weight compared to 31% in the placebo group, with 70% losing 10% or more and 30% losing at least 20%. Gastrointestinal side effects were more common with semaglutide compared to placebo, but most were transient and resolved without permanently halting treatment or prompting patients to withdraw from the study. Cholelithiasis occurred in 2.6% of semaglutide-treated subjects and 1.2% of placebo subjects, with three semaglutide-treated subjects experiencing mild acute pancreatitis, two of which were associated with gallstones; all recovered during the trial. Based on these results, semaglutide appears to be the most effective weight loss medication among GLP-1s, with a placebo-adjusted average percentage weight loss approximately twice that reported for other drugs in this class. This inference was drawn from STEP 8, a direct trial comparing semaglutide and liraglutide, where average weight loss was 15% and 6.5%, respectively (JAMA. 2022;327(2):138-150). STEP 1 also provides the first evidence that drug intervention can lead to more than 10% weight loss in the majority of treated individuals.
STEP 2 randomized over 1,500 T2DM subjects to receive weekly injections of semaglutide 2.4 mg, semaglutide 1.0 mg, or placebo for 68 weeks (Lancet. 2021;397(10278):971-84). The average weight change in the three treatment groups was significantly different, with -9.6% for 2.4 mg semaglutide, -7% for 1.0 mg semaglutide, and -3.4% for placebo, with the side effect profile in this cohort being similar to that observed with semaglutide in STEP 1. Notably, the higher dose of semaglutide resulted in about 2.5% more weight loss compared to the lower dose, but the blood glucose reduction was comparable. Additionally, the average weight loss in diabetic patients was lower than that observed in non-diabetic subjects (approximately 10% vs. 15%), consistent with results observed in the SCALE trials, where non-diabetic groups lost 8% and diabetic cohorts lost 5.4% of their weight (JAMA. 2015;314(7):687-699; Lancet. 2021;397(10278):971-84). Although both trials targeting T2DM subjects had older cohorts with a higher male percentage and differed in drug usage, this trend regarding the degree of weight impact from GLP-1RA seems consistent and warrants further testing.
STEP 3 randomized 611 non-diabetic subjects to receive either semaglutide 2.4 mg or placebo as an adjunct to intensive behavioral therapy, incorporating structured diets (JAMA. 2021;325(14):1403-1413). In the first eight weeks of the study, all subjects were provided with a low-calorie meal replacement diet and received intensive behavioral therapy throughout the 68-week protocol. Participants were also required to engage in 100 minutes of physical activity weekly, increasing by 25 minutes every four weeks to a maximum of 200 minutes per week. By week 68, the estimated average weight change for semaglutide was -16.0%, compared to -5.7% for placebo, a difference of 10.3%. Similar to other STEP trials, most (75.3%) of the subjects using semaglutide lost at least 10% of their weight. The placebo group also had a relatively high rate of weight loss, with 27.0% losing at least 10% of their initial weight, demonstrating the strength of lifestyle interventions. However, the 16% weight change induced by semaglutide in STEP 3 did not significantly differ from the results seen in STEP 1, raising the question of how much the intensified lifestyle changes contribute to the enhanced effects of potent medications.
STEP 4 aimed to test the effects of discontinuing semaglutide after a course of weight loss treatment to assess the impact on weight maintenance (JAMA. 2021;325(14):1414-1425). A total of 803 subjects received 2.4 mg of semaglutide for 20 weeks and lost about 10% of their initial weight. Of these, 535 subjects were then randomly assigned to continue semaglutide, while 286 subjects received placebo for the following 48 weeks. During the 20-week run-in period, subjects showed reductions in waist circumference, BMI, blood pressure, and HbA1c levels, with improvements in lipid levels associated with weight loss. After random assignment, the average weight further decreased by -7.9% in the semaglutide cohort, while those switched to placebo regained more than half of their initial weight loss. In the withdrawal group, improvements in obesity-related comorbidities (such as blood pressure) also reversed. In the continuous treatment cohort of STEP 4, the average weight loss over 68 weeks exceeded 17%, with 40% of treated subjects initially losing more than 20%, the largest weight loss observed in the STEP program. However, the results of this trial indicate that the beneficial effects of semaglutide on weight seem to require ongoing treatment.
Overall, the STEP trials provide the best evidence of the potential for medical weight loss to date. The effects of semaglutide on weight loss significantly exceed those of other currently available agents, with benefits for clinically significant obesity-related factors such as blood pressure, lipids, and blood glucose. During the 68-week study period, the impact of semaglutide on weight loss did not diminish, and longer trials are needed to determine the ultimate course of weight loss. It remains unclear from STEP 4 whether individuals receiving shorter treatment courses will regain their initial weight over time, but experiences from other weight loss interventions suggest that this is indeed the case. A summary of completed and ongoing STEP trials is provided in Table 1. In recent years, oral forms of semaglutide have been extensively studied in T2DM subjects, with weight loss effects observed when corrected for exposure to circulating drugs (Cell Rep Med. 2021;2(9):100387).
Dosage units for semaglutide and liraglutide are in milligrams (mg).
GLP-1RA and Weight Loss in Special Populations
Childhood and adolescent obesity is one of the major pediatric healthcare issues, with the pervasive environmental influences promoting positive energy balance having more limited impacts compared to dietary and other lifestyle measures. In a recent trial, 250 adolescents with a BMI > 30 were randomly assigned to receive liraglutide or placebo for 56 weeks (N Engl J Med. 2020;382(22):2117-2128). While only 80% of the liraglutide group was able to titrate to the maximum dose of 3 mg, significant weight loss was achieved through active treatment (approximately 6% placebo-adjusted). About 40% of subjects in the liraglutide group reduced their initial BMI by over 5%, compared to 19% in the placebo control group. These results are consistent with liraglutide’s trial results in adults, suggesting that young people respond similarly to GLP-1. Effective treatment of obesity in young people could have a disproportionately positive impact on public health, as they are more susceptible to the health consequences of weight gain.
Despite the improvements in a range of metabolic parameters in T2DM and/or obesity patients following weight loss surgery, about half of the treated patients do not achieve diabetes remission or a BMI < 30 within 5 years (Diabetes Care. 2016;39(6):861-877). Furthermore, 21%-43% of patients who achieved remission after gastric bypass surgery experience recurrence within 3-9 years (Obes Surg. 2015;25(1):143-158). To meet the needs of these patients, evaluations of GLP-1RA treatment have been conducted in patients who have undergone gastric bypass or sleeve gastrectomy. In the GRAVITAS trial, 80 patients with persistent diabetes after weight loss surgery were randomly assigned to receive 1.8 mg liraglutide or placebo for 26 weeks (Lancet Diabetes Endocrinol. 2019;7(7):549-559). Compared to placebo, liraglutide treatment reduced HbA1c by 1.22%. Additionally, subjects receiving liraglutide lost approximately 5 kg more than the control group (Lancet Diabetes Endocrinol. 2019;7(7):549-559). These findings are somewhat surprising, as GLP-1 levels in individuals who have undergone weight loss surgery are 10-20 times higher than in normal individuals. In fact, a common explanation for the metabolic benefits of gastric bypass and sleeve gastrectomy is the increased signaling through the GLP-1R system. However, plasma concentrations of GLP-1RA exceed the circulating levels of natural GLP-1 by at least 100 times, and the clinical response to GLP-1RA is proportional to drug exposure (Cell Rep Med. 2021;2(9):100387). Furthermore, the elevation of GLP-1 concentrations following weight loss surgery is transient and occurs only postprandially; long-acting GLP-1RA leads to sustained exposure of GLP-1R to stimulation.
Hints, Issues, and Future Directions
The completion of most STEP trials demonstrates the potential of GLP-1RA as a weight management strategy and has implications for the physiology, pharmacology, and clinical applications of GLP-1RA. From a physiological perspective, the GLP-1R signaling system appears to have considerable excess capacity. The concentrations of endogenous GLP-1 seem to act at the bottom of an exposure-response curve that has yet to be defined for maximum weight loss limits. This raises the possibility that continued refinement of GLP-1 receptor antagonists (especially modifications that can reduce common gastrointestinal side effects) will allow for further dose increases, potentially leading to even greater efficacy. From a pharmacological perspective, the application of GLP-1RA for weight loss is now the most common form of CNS-endocrinology treatment, with pharmacological ligands primarily targeting the brain. Pharmacokinetics may also contribute to the weight loss effects of these drugs, with longer and more stable exposure times resulting in better outcomes. However, it is strange that, even considering the similarities in molecular size and receptor binding portions of these drugs and the comparable concentrations achieved in circulation, liraglutide is less effective than semaglutide (Cell Rep Med. 2021;2(9):100387; Pediatr Obes. 2021;16(10):e12799). Understanding whether structural nuances affect access to key brain regions or interactions with GLP-1R will help advance the continued development of GLP-1RA and other incretin-based drugs.
From a clinical perspective, the development of GLP-1RA weight loss medications, particularly the effect sizes observed in the STEP trials, provides urgently needed first-line hope for patients and their providers. The effects of semaglutide treatment over two years (average weight loss of 10%-20%) represent a significant advancement in pharmacotherapy for obesity. The efficacy of drugs in clinical trials often reflects their optimal performance; thus, it will be vital to assess the effectiveness of semaglutide and related drugs in broader clinical practice. Additionally, the subjects in the STEP project were primarily white and female, and it remains to be seen how these results translate to more diverse populations. Given the sustained weight loss observed over 68-104 weeks in STEP 4, it is important to understand how longer treatment durations will affect outcomes. Other GLP-1 receptor antagonists that have been treated for more than one year have shown some degree of weight regain, which is also a trend observed in patients who have undergone weight loss surgery. Finally, all GLP-1RAs are expensive, and short-term costs will pose a barrier to widespread use; costs have been shown to be a factor in the non-use of such medications (Diabetes Care. 2009;32(12):2143-2148). In this regard, understanding the factors influencing efficacy and different patient characteristics and behaviors will help better allocate healthcare resources.
In addition to demonstrating the direct clinical benefits of semaglutide, the STEP trials exemplify the potency of GLP-1R agonists for weight loss. This provides new momentum for an already vibrant field of drug research. It seems that longer-acting formulations can be developed to enhance convenience and adherence. Moreover, recent studies on the structure and function of GLP-1R and other G protein-coupled receptors indicate that modifications to ligand-receptor interactions can shift downstream signaling and relative toxicity balance. Combination therapies are also in development. Co-injecting insulin agonists with semaglutide has resulted in a 17% weight loss over 20 weeks compared to using 2.4 mg semaglutide alone (Lancet. 2021;397(10286):1736-1748). Advances in peptide chemistry have led to the development of multi-receptor agonists, which may have enhanced metabolic efficacy. For example, dual GLP-1R/glucose-dependent insulinotropic polypeptide (GIP) receptor agonist tirzepatide has demonstrated weight loss effects approximately twice that of using 1.0 mg semaglutide (N Engl J Med. 2021;385(6):503-515). Other dual agonists activating both GLP-1R and glucagon receptors (GcgR), or tri-agonists signaling through GLP-1R/GIPR/GcgR, have shown promise in preclinical research and are currently being studied in humans. These valuable results suggest that leveraging the activity of GLP-1R may just be the beginning of scalable, meaningful, and durable obesity treatments. In this sense, the STEP series of studies may just be the first step.
Chen Kang 2022-12-02
Endocrine Metabolic Disease @CK Medicine
Endocrine Metabolic Disease Knowledge Framework @CK Medicine
Endocrine Metabolic Disease Graded Diagnosis and Treatment @CK Medicine
 , but if you are not an endocrinology specialist and are still so interested in this content that you reached this part of the PS, and even want to join the group, then just follow the steps in the PS, welcome!
, but if you are not an endocrinology specialist and are still so interested in this content that you reached this part of the PS, and even want to join the group, then just follow the steps in the PS, welcome!
