Cerebral cysticercosis is cerebral cysticercosis and is the most common brain parasitic disease. The incidence accounts for about 80% of cysticercosis. It occurs nationwide. Cerebral cysticercosis is also known as cysticercosis, which is caused by the larvae of the pork tapeworm parasitizing the brain. It is important to clarify that the disease caused by the adult pork tapeworm parasitizing the human intestine is called tapeworm disease. The larvae (cysticerci) of the pork tapeworm parasitize the human subcutaneous muscles, brain, eyes, etc., leading to cysticercosis. Cysticercosis and tapeworm disease are two different diseases, and the harm caused by cysticercosis is much greater than that of tapeworm disease. The parasite is mainly distributed in the Sanbei region and Yunnan-Guizhou region.
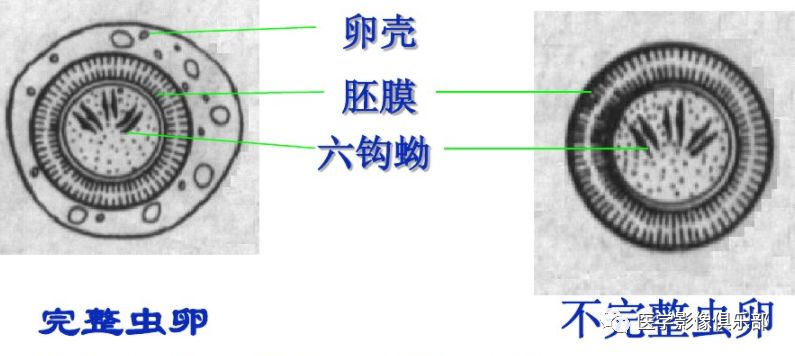
Transmission routes: Humans accidentally ingest the eggs of the pork tapeworm (with hookworm) or when a patient with pork tapeworm vomits, the eggs flow back into the stomach, and the six-hooked larvae exit in the duodenum and penetrate the intestinal wall, reaching the whole body through the bloodstream, evolving into cysticerci. The parts of the human body where cysticerci are found, in order of occurrence, are subcutaneous tissue, muscles, brain, eyes, heart, liver, lungs, and peritoneum.Cerebral cysticercosis is transmitted through fecal-oral contact from humans carrying the tapeworm, while tapeworm disease is transmitted by consuming infected pork.The transmission of cerebral cysticercosis is mostly human-to-human, rather than the commonly believed pig-to-human. With the frequent movement of people internationally, clinicians who encounter patients with epilepsy, especially those who have lived in developing countries, should consider the possibility that their epilepsy, headaches, and focal neurological deficits are caused by cerebral cysticercosis; and should assess the stage of the disease by identifying the imaging characteristics of cerebral cysticercosis.
Tapeworm disease:Tapeworm disease is caused by eating undercooked pork containing cysticerci. Once the scolex (the head of the parasite) is ingested, it attaches to the mucosal layer of the small intestine, producing several proglottids (segments) and developing into an adult. This is tapeworm disease. Eventually, segments containing eggs will detach from the body and be excreted with feces. Pigs become infected after eating feed contaminated with the feces of infected individuals. These ingested larvae are absorbed through the intestine and spread to the muscles of the pig, forming cysticerci, thus completing their life cycle.
Cysticercosis: The infection form of this disease is consistent between humans and pigs, both transmitted through fecal-oral contact with human carriers. Once ingested, the larvae lose their embryonic membranes under the action of gastric acid, becoming a cyst containing larvae, known as six-hooked larvae. They migrate through intestinal absorption and can often parasitize the brain, eyeballs, and muscles, forming cysts.
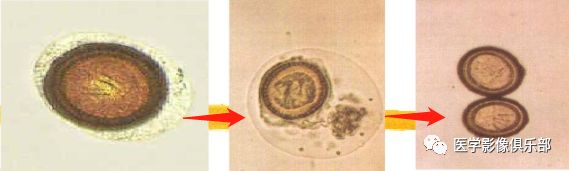
The above image shows the eggs losing their embryonic membranes under the action of gastric acid, forming cysts, with six-hooked larvae inside.
Clinical and Pathological Features
1.Pathology When cysticerci enter the brain, they form vesicles, which contain liquid and white scoleces. The dead body is enveloped by inflammatory cells, with the outer layer forming granulation tissue rich in blood vessels and collagen fibers. Later, the collagenous connective tissue repairs and turns into scar tissue, and the dead body calcifies. Based on the location of the lesions, it can be divided into:①Intracranial cysticercosis: Vesicles are mostly located in the cortex and basal ganglia, ranging from several to hundreds, with superficial ones protruding on the brain surface,5-10mm in size, but sometimes a single large cyst may form;②Ventricular cysticercosis: Vesicles are free or attached to the ependyma, with a diameter of 10-20mm, thin-walled vesicles may be accompanied by obstructive hydrocephalus, and the lesions in ventricular cysticercosis are generally slightly larger than those in parenchymal cysticercosis;③Subarachnoid cysticercosis: Vesicles are located in the subarachnoid space, commonly seen in the basal cistern, sometimes connected like grapes, which may be associated with meningeal adhesions or obstructing cerebrospinal fluid circulation pathways. Once the lesions invade the arachnoid, there are generally symptoms of hydrocephalus.
2.Clinical manifestations Include consciousness disorders, mental disorders, seizures, intracranial hypertension, hydrocephalus, etc. Physical examination may reveal subcutaneous nodules, mostly located on the head and trunk. The cysticercus complement fixation test may be positive.

The above image shows the adult pork tapeworm, with the thinnest part at the end being the scolex, the thicker part being the strobila, and the neck between the head and strobila mainly serves a reproductive function. The strobila is flat, white or off-white, segmented, narrow at the front and wider at the back. This organism lacks a digestive system and relies solely on the absorption of nutrients through its body wall.
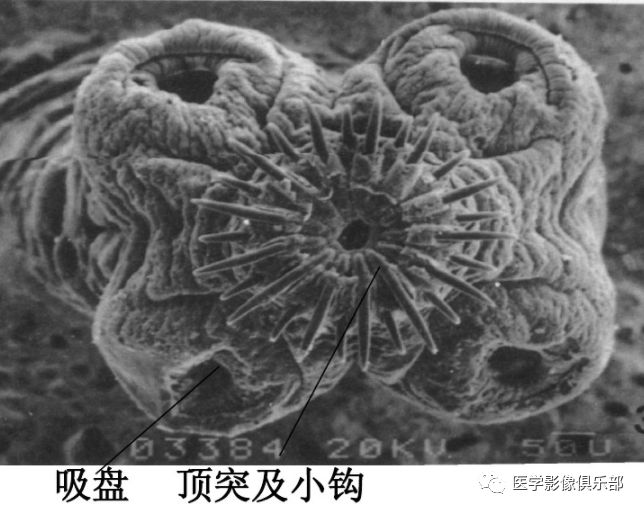
The above image shows the scolex of the pork tapeworm, which typically has four suckers that can securely attach to the inner wall of the digestive tract.
Imaging Findings
1. CT Findings
(1)Parenchymal Type(Five Subtypes)
1)Acute Encephalitis Type: Widespread low density in the supratentorial hemisphere, mostly located in the white matter, and may also be scattered in the cortex. Generalized brain swelling, narrow sulci, and small ventricles. No enhancement on contrast scans.
2)Multiple Small Cystic Type: On plain scans, multiple scattered round or oval low-density shadows are seen in the supratentorial hemisphere, often at the gray-white matter junction, with diameters of 5-10mm. Small nodular high-density shadows representing cysticercus scoleces may be seen inside. Generally, no enhancement on contrast scans, with mild surrounding edema.
3)Single Large Cystic Type: A single giant cysticercus or multiple cysticerci fused together. It appears as a round, oval, or lobulated low-density lesion in the brain, with a density of cerebrospinal fluid inside, clear boundaries, and no solid nodules. The large cyst itself shows no enhancement, but may have mild ring enhancement due to fibrous tissue proliferation.
4)Multiple Nodules or Ring Enhancement Type: On plain scans, multiple irregular low-density shadows are scattered. On enhanced scans, low-density shadows show nodular or ring enhancement, with diameters of 3-5mm.
5)Multiple Calcification Type: Multiple calcifications in the brain parenchyma, round or oval, with diameters of 2-5mm. Sometimes only a piece of calcification is seen, with no edema surrounding the calcification, and no enhancement on contrast scans.
(2)Ventricular Type: Most commonly seen in the fourth ventricle, followed by the third ventricle, and the lateral ventricle is rare. Because the density of the cysticercus vesicle is similar to that of cerebrospinal fluid, the cyst wall is thin, CT is difficult to display the vesicle, only indirect signs can be seen, such as abnormal morphology of the ventricle or localized asymmetric enlargement of the ventricle, displacement of the choroid plexus, and obstructive hydrocephalus. Some vesicles may have a density higher than that of cerebrospinal fluid, and the cyst wall may show ring enhancement or calcification.
(3)Meningeal Type: On plain scans:①Lateral fissure and suprasellar cistern cystic enlargement, with mild occupying effect;②Enlargement and deformation of the subarachnoid space; ③Symmetrical enlargement of the ventricles. On enhanced scans, sometimes the cyst wall enhancement or nodular enhancement can be seen, and meningeal enhancement is also observed.
(4)Mixed Type: The above two or more types of manifestations exist simultaneously.
2.MRI Parenchymal Cysticercosis MRI is more characteristic, mostly round cystic lesions,2-8mm in size, with eccentric wall nodular shadows,representing cysticercus scoleces.During the survival phase of the cysticercus, edema is mild. On enhanced scans, the cyst wall may enhance or not enhance.When the cysticercus dies,the scolex shows unclear,with increased surrounding edema,significant occupying effect,and increased thickness of the enhancement ring. At this time, the “white target sign” can be seen, where T2WI cyst fluid and surrounding edema show high signal, while the cyst wall and the unclear scolex inside show low signal, the low signal is caused by the gradual fibrosis, organization, and calcification of the cysticercus, with reduced water content and decreased hydrogen proton density. The “black target sign” refers to T1WI where the scolex inside the cyst shows high signal, with more bound water, and the hydrogen protons in the bound water have a motion frequency close to the Lamor frequency, while the rest show low signal.
Cysticerci located in the ventricles, cisterns, and sulci are round,2~8mm in size, showing longT1 and longT2 signals, often with the scolex not visible. The adjacent brain tissue may have smooth pressure marks. Some may present as large cystic lesions, lobulated, with septa, occasionally with the scolex located at the edge.DWI cyst fluid shows low or slightly low signal, while the scolex shows high signal due to more bound water. Meningeal cysticercosis shows multiple small cysts in the sulci, many of which are formed by the adhesion of cysticercus in the sulci to the meninges.
Stages of Parenchymal Cysticercosis
The central nervous system is infected by cysticerci, forming cerebral cysticercosis. When the brain parenchyma is involved, the disease can be divided into four independent stages:Vesicular Stage, Gelatinous Stage, Nodular Granuloma Stage, and Calcification Stage.
1、Vesicular Stage:In this stage, the cystic membrane of the parasite is intact, and the host’s immune response is mild. At this stage, there is only liquid in the cyst. The liquid’s CT and MRI imaging features are similar to cerebrospinal fluid.
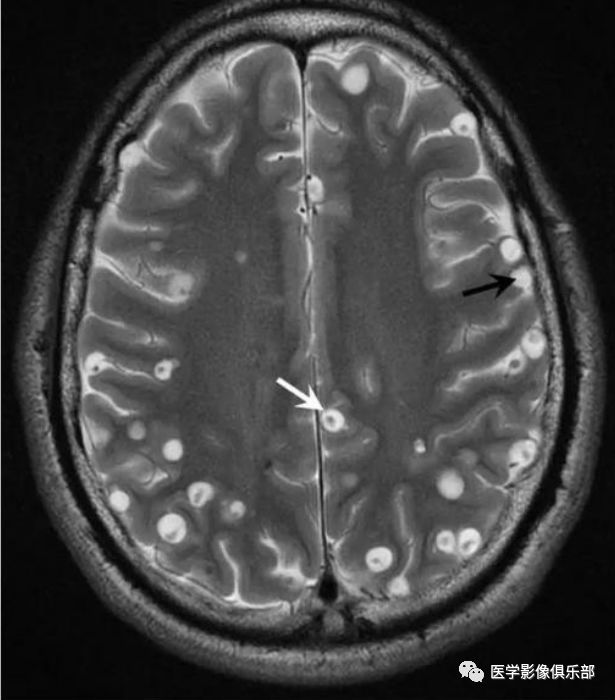
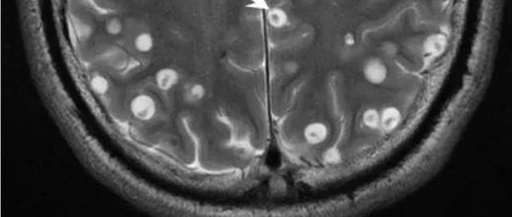
The above image shows an MR scan of the brain (axial T2-weighted imaging) showing lesions at two different stages. First, the cyst can be seen containing only liquid (indicated by the black head). The image also shows that this patient has mixed-type nodular granuloma lesions, characterized by high-signal liquid and calcified scoleces, which are low signal (indicated by the front white head).
2、Gelatinous Stage
When the cyst ruptures, the liquid inside becomes antigenic and seeps into surrounding tissues, causing a strong immune response, which is the gelatinous stage. In MRI imaging, the lesion area appears as thickened, enhanced membranes, contrasting with surrounding tissue edema; on CT, it appears as a high-density cyst.
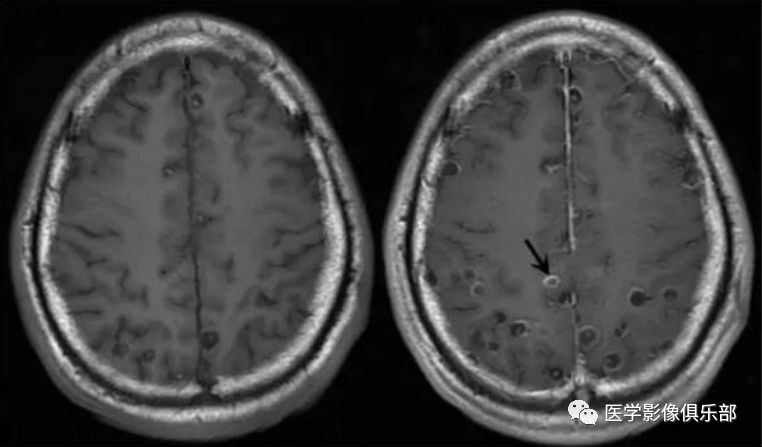
The above images show axial T1-weighted plain scans and enhanced scans, displaying the enhancement of the cyst wall.
3、Nodular Granuloma Stage
In this stage, the cyst further degenerates, and the edema condition also alleviates. MRI shows that these cysts transform into nodules or mixed tissues. The surrounding nodular lesions appear as high signal on MRI, with the central signal intensity matching that of brain white matter. Mixed-type lesions show high signal, with the central area appearing low signal due to scolex calcification; CT shows the “target sign”.
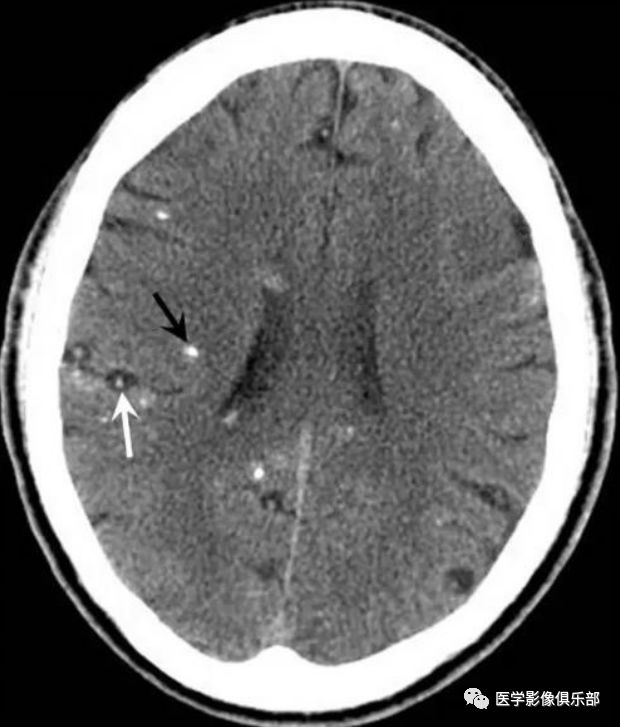
The above image shows a CT scan of the head (axial plain scan) displaying two different stages of the disease. The “target sign” (indicated by the white arrow) is seen in the nodular granuloma stage. Calcified lesions (indicated by the black arrow) are seen in the calcification stage.
4、Calcification Stage
In this stage, the cyst calcifies, forming granulomas within the nodules. CT shows calcified lesions in the brain parenchyma. MRI shows small nodular lesions, appearing isosignal on T1 weighted images and low signal on T2 weighted images.
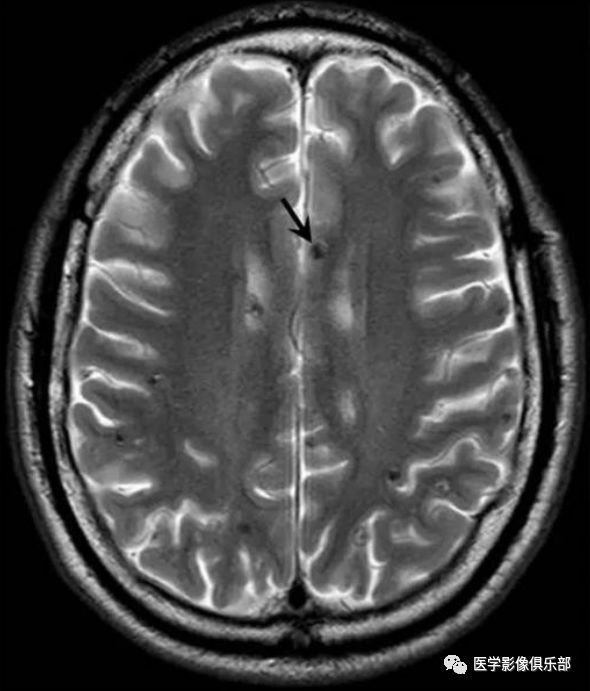
The calcified component has a low hydrogen proton density, which cannot produce a stronger signal, generally showing low signal performance across various sequences.
Diagnosis and Differential Diagnosis
1.Key points for diagnosis: ① Clinical manifestations are diverse, mainly including seizures, intracranial hypertension, motor disorders, mental abnormalities, and meningeal irritation signs; ② History of tapeworm infection and subcutaneous nodules; ③ Cysticercus complement fixation test or indirect hemagglutination test is positive; ④ CT and MRI manifestations as described above.
2. Differential Diagnosis
(1)Encephalitis type needs to be differentiated from multiple sclerosis, multiple cerebral infarcts, and subcortical arteriosclerotic encephalopathy.
(2)Single large cyst type needs to be differentiated from dermoid cysts, epidermoid cysts, arachnoid cysts, and brain penetrating malformations.
(3)Multiple small cyst types need to be differentiated from brain metastases and cerebral abscesses.
3.Comparative diagnostic value: MRI shows advantages over CT in assessing the survival of cysticerci. Additionally, MRI has a higher detection rate for areas that are not easily displayed by CT, such as the brain base and orbits.