
Neurology Medical Network Organized by: Xuan Zhi Xuan
The structure of the brainstem is relatively complex, and different levels, locations, and sizes of lesions can produce various clinical manifestations, constituting many clinical syndromes of brainstem damage. Therefore, localization can sometimes be quite difficult. It is essential to combine the anatomical characteristics of the brainstem as a guide for lesion localization. The principles for localizing brainstem lesions are as follows.(1) Determine if there is a lesion in the brainstem:1. Damage to cranial nerve nuclei or their roots:Since cranial nerve nuclei III to XII are all located within the brainstem and are connected by afferent or efferent fibers, and the cranial nerve nuclei are quite close to each other, when there is damage to the brainstem, at least one or two or more cranial nerve nuclei or their intracranial fibers are damaged, resulting in corresponding clinical symptoms.2. Crossed syndromes are characteristic of brainstem lesions:Brainstem lesions often damage one side. Therefore, damage to the sensory and motor nuclei of cranial nerves and their fibers on the same side as the lesion leads to peripheral paralysis and sensory disorders, which often indicate the location of the lesion. At the same time, the descending motor conduction pathways and ascending sensory conduction pathways passing through the same side of the lesion are also damaged, resulting in symptoms and signs of sensory and/or motor disorders on the opposite side of the lesion, thus forming crossed syndromes. That is, peripheral paralysis and sensory disorders of the cranial nerves on the same side of the lesion, and central paralysis and conduction pathway sensory disorders of the limbs on the opposite side of the lesion, possibly accompanied by or not accompanied by sensory and motor disorders of cranial nerves below the level of the lesion on the opposite side. For example, midbrain lesions can cause oculomotor nerve-related crossed paralysis, where paralysis of the oculomotor nerve occurs on the lesion side, and central limb paralysis and central facial nerve and hypoglossal nerve paralysis occur on the opposite side of the lesion. If the lesion is located in the pons, crossed facial nerve paralysis may occur, where in addition to peripheral facial paralysis on the same side of the lesion and central paralysis of the opposite limb, central hypoglossal nerve paralysis may also appear. Similarly, if the lesion is located in the medulla oblongata, crossed hypoglossal nerve paralysis may occur, where peripheral paralysis of the hypoglossal nerve occurs on the same side of the lesion, while central paralysis of the opposite limb occurs. Because the cortical brainstem bundle terminates at the medulla, there is no upper motor neuron injury of the cranial nerves on the opposite side of the lesion.(2) Determine the level of brainstem lesions (longitudinal localization)Determining the level of brainstem lesions mainly depends on whether the cranial nerve nuclei and their outgoing intracranial fibers are damaged. Generally speaking, the third and fourth pairs of cranial nerves and their nuclei, as well as the pupillary reflex center, are located in the midbrain; the fifth, sixth, and seventh pairs of cranial nerves and their nuclei and corneal reflex center are located in the pons; the eighth pair of cranial nerves and their nuclei are located at the junction of the pons and medulla; the ninth, tenth, eleventh, and twelfth pairs of cranial nerves and their nuclei and pharyngeal reflex are located in the medulla. In addition, the spinal nucleus of the trigeminal nerve also exists in the medulla. Therefore, when paralysis of the eye muscles innervated by the oculomotor nerve occurs, along with the disappearance of the pupillary reflex, and symptoms of brainstem conduction pathway impairment, it indicates that the lesion is in the midbrain; if there is motor and sensory impairment in the distribution area of the trigeminal nerve, loss of corneal reflex, and conduction pathway dysfunction, the lesion can be confirmed to be in the pons; if there are certain symptoms of the ninth to twelfth pairs of cranial nerves, loss of pharyngeal reflex, and motor or sensory impairment of the opposite limb, the lesion must be in the medulla. Thus, it can be seen that the longitudinal localization diagnosis of brainstem lesions mainly relies on the presence of cranial nerve roots and cranial nerve nuclei. These lesions are all located on the side of cranial nerve paralysis. It should be pointed out that although cranial nerve nuclei or their roots are easily damaged during brainstem lesions, it does not necessarily mean direct damage to the lesions; it can also be due to indirect effects of pressure or blood circulation disorders caused by the lesions.(3) Determine the extent of brainstem lesions (transverse localization)Determining the extent of brainstem lesions is related to the location of the lesions. The brainstem is an irregular cylindrical body, with a thicker upper part and a thinner lower part. If the lesion is located in the medulla, due to the relatively small volume of the medulla, even small lesions, especially small lesions in the posterior medulla, can easily cause significant functional impairment, leading to bilateral damage. For example, a small amount of bleeding or small softening near the hypoglossal nucleus can often cause bilateral nuclear damage of the hypoglossal nerve, resulting in complete paralysis of the tongue. The pyramids are located at the very bottom of the medulla, and the two sides of the pyramids are closely adjacent at this point, so small lesions can cause damage to both sides of the pyramidal tract, resulting in quadriplegia. The bilateral medial lemniscus is close to each other in the lower medulla and pons, so small lesions in this midline area can lead to deep sensory impairment and sensory ataxia below the cervical spinal cord. The higher levels of the brainstem are wider, and the pons and midbrain are larger in volume, thus similar-sized lesions in the midbrain and pons often only affect one side, resulting in unilateral symptoms and signs, rarely producing bilateral nuclear damage symptoms and signs as seen in the medulla. Therefore, the range and degree of functional impairment caused by brainstem lesions do not necessarily represent the range and degree of the lesions, but the number of cranial nerve damages can, in a sense, reflect the extent of the lesions.(4) Certain special symptoms and signs during brainstem lesionsLesions in certain parts of the brainstem can produce specific symptoms, which are very helpful for the localization diagnosis of brainstem lesions. For example; ① spatial perception disorders: patients may see someone entering the adjacent room through the wall and can see other objects in the adjacent room, with the wall appearing curved or distorted, or feeling collapsed. This is seen in lesions of the brainstem at the bottom of the fourth ventricle and the area where the medial longitudinal fasciculus is located; ② hallucinations: hallucinations are quite common when lesions occur in the midbrain or the bottom of the tail of the third ventricle, resembling daydreams, suggesting that the lesions may be close to the sleep-wake center.(5) Differentiating between lesions inside and outside the brainstemCorrectly distinguishing whether the lesion is inside or outside the brainstem is of great significance for certain diseases, especially regarding the treatment and prognosis of tumors. Generally speaking, lesions outside the brainstem are mainly treated surgically, while lesions inside the brainstem are treated conservatively. The differentiation between intramedullary and extramedullary lesions in the brainstem is as follows: ① lesions inside the brainstem show significant crossed signs, while lesions outside the brainstem show insignificant or no crossed signs; ② lesions inside the brainstem have cranial nerve paralysis and limb paralysis occurring at similar times, while lesions outside the brainstem have cranial nerve paralysis appearing early and more frequently, and if there is paralysis or sensory impairment of the opposite limb, it often occurs later and is milder; ③ lesions inside the brainstem often have symptoms purely due to damage to the internal structures of the brainstem, such as damage to the medial longitudinal fasciculus causing dissociation of the eyes, inability to fixate, vertical nystagmus, or medial longitudinal fasciculus syndrome (internuclear ophthalmoplegia); lesions outside the brainstem do not exhibit symptoms such as damage to the medial longitudinal fasciculus and eye movement disorders; ④ distinguish whether cranial nerve damage is nuclear or peripheral: lesions inside the brainstem often damage part of the oculomotor nerve nuclei or both sides of the oculomotor nerve nuclei, presenting as oculomotor nerve paralysis often being incomplete and bilateral; and since the oculomotor nerve nuclei also send fibers innervating the orbicularis oculi, paralysis of the oculomotor nerve is often accompanied by paralysis of the orbicularis oculi, manifesting as widening of the palpebral fissure and inability to close the eyes. The hypoglossal nerve nucleus also sends out some fibers innervating the orbicularis oris, so lesions damaging the hypoglossal nerve nucleus can present with paralysis of the tongue muscles, along with paralysis of the orbicularis oris. (Table 2-1).
| Distinguishing Between Intramedullary and Extramedullary Lesions | ||
| Intramedullary Lesions | Extramedullary Lesions | |
| Age | More common in children | More common in adults |
| Course and Lesion | Shorter, rapid development, often bilateral cranial nerve damage | Longer, slower progression, often unilateral initially, gradually becoming multiple cranial nerve damage |
| Cranial Nerves | Oculomotor nerve nucleus: dissociative (incomplete), bilateral muscle paralysis, incomplete paralysis of orbicularis oculi; | Oculomotor nerve root: complete oculomotor paralysis, more common unilaterally, no orbicularis oculi paralysis; |
| Hypoglossal nerve nucleus: tongue muscle paralysis with orbicularis oris paralysis; | Hypoglossal nerve root: tongue muscle paralysis without orbicularis oris paralysis; | |
| Trigeminal sensory nucleus: segmental dissociative sensory impairment; | Trigeminal nerve root: peripheral sensory impairment; | |
| Medial longitudinal fasciculus: internuclear ophthalmoplegia, dissociation of the eyes, inability to fixate, vertical nystagmus; | No damage; | |
| Abducens nucleus: both eyes gaze at the healthy side. | No damage. | |
| Pyramidal signs | Except for those originating from the brainstem base, early signs do not appear or are only mild pyramidal signs | Often appear early due to pressure on the ventral side of the brainstem; |
| Increased intracranial pressure | Less common | Often combined |
| Cerebrospinal fluid changes | Slight | Often with increased protein |
| Diseases | Intramedullary glioma | Lesions in the cerebellopontine angle, cerebellum, pineal gland, and craniopharyngioma |
(1)Symptoms of Medullary Lesions
The medulla has a relatively small volume and a dense tissue structure. A small lesion can often involve many structures with different functions, leading to widespread and significant symptoms and signs, and can easily cause bilateral damage to the medulla. Depending on the location of the lesion, various symptoms and signs can occur.
1. Motor Disorders:
Motor disorders caused by medullary lesions mainly refer to paralysis caused by damage to the pyramidal tract. The pyramidal tract within the brainstem includes both the corticospinal tract and the corticobulbar tract (corticomedullary tract). The corticobulbar tract terminates entirely at the medullary nuclei and hypoglossal nerve nucleus. The corticospinal tract travels to the lower end of the pyramids, where most fibers (about 75%-90%) cross the midline to form the pyramidal decussation. The crossed fibers descend in the lateral column of the spinal cord and terminate in the anterior horn on the same side. The pyramidal fibers begin to cross just below the bulb, continuing until they cross below the first cervical nerve root.The corticospinal tract controls the movement of the opposite limb, where fibers controlling the upper limb muscles are located medially, and fibers controlling the lower limb muscles are located laterally. The corticospinal lateral tract controls the movement of the same side limb, where the arrangement of fibers controlling upper and lower limb muscles is similar to that of the corticospinal tract, with upper limb fibers still medial and lower limb fibers lateral. At the pyramidal decussation, fibers controlling upper limb muscle activity cross first, while fibers controlling lower limb muscles cross later (as shown in Figure 2-82).
① If the lesion is above the pyramidal decussation (i.e., corticospinal tract), it presents as upper motor neuron paralysis of the opposite limb. ② If the lesion is below the pyramidal decussation, it presents as upper motor neuron paralysis of the same side. ③ If the lesion is precisely at the pyramidal decussation, quadriplegia may occur. ④ If there is a small lesion on the lateral side of the pyramidal decussation (such as thrombosis of the medullary paramedian artery), it may damage fibers that have already crossed controlling upper limb muscles and those that have not crossed controlling lower limb muscles, resulting in upper motor neuron paralysis of the same side upper limb and the opposite lower limb, known as crossed upper and lower limb paralysis (this clinical situation is not very common).
2. Cranial Nerve Paralysis:
The medulla contains the last four pairs of cranial nerve nuclei and their outgoing cranial nerves. The nucleus ambiguus sends out motor fibers that join the glossopharyngeal, vagus, and accessory nerves in the medulla. The hypoglossal nerve nucleus sends out the hypoglossal nerve.
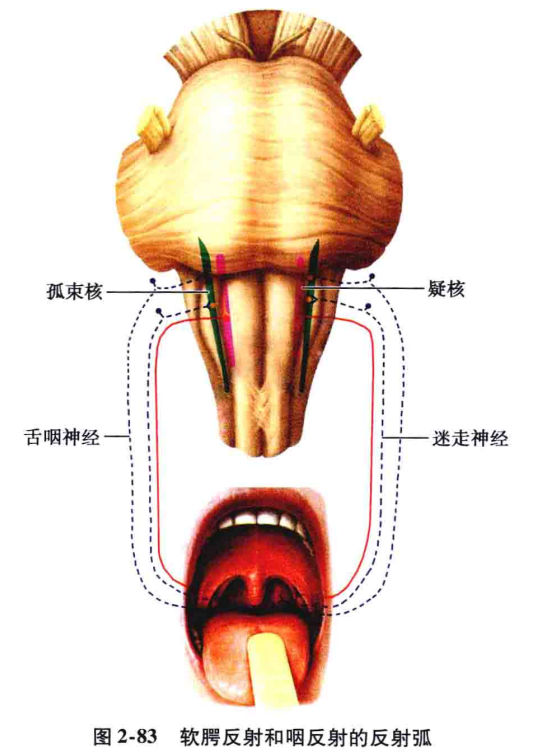
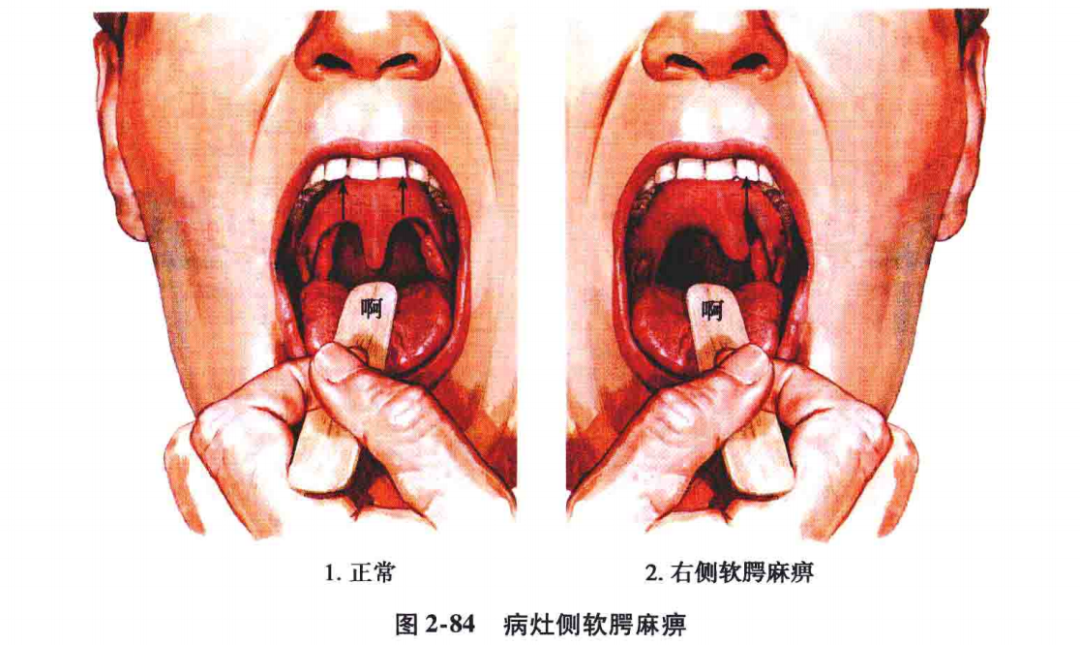
(1) Damage to the nucleus ambiguus and its outgoing fibers: It manifests as hoarseness, coughing while drinking, difficulty swallowing, peripheral paralysis of the soft palate (drooping), deviation of the uvula towards the opposite side of the lesion, and weakened or absent pharyngeal reflex, known as medullary paralysis (bulbar paralysis) (see Figures 2-83, 2-84).
One side of the nucleus ambiguus receives bilateral control from the corticobulbar tract, so unilateral damage to the corticobulbar tract does not lead to dysfunction of the nucleus ambiguus; only when bilateral damage occurs does bilateral dysfunction of the nucleus ambiguus manifest as hoarseness, coughing while drinking, difficulty swallowing, and soft palate paralysis, but with normal pharyngeal reflex, known as pseudobulbar paralysis.(2) Damage to the hypoglossal nerve nucleus and its fibers: When one side of the hypoglossal nerve nucleus and its outgoing fibers are damaged, it can lead to paralysis of the tongue muscles on the same side, with the tongue deviating towards the lesion side when extended and deviating towards the healthy side when retracted. Over time, atrophy of the tongue muscles on the paralyzed side and fasciculations or fibrillations may occur (see Figure 2-85).

One side of the hypoglossal nerve nucleus only receives control from the opposite corticobulbar tract, so when there is damage to the corticobulbar tract on one side, it presents as paralysis of the tongue muscles on the opposite side, manifesting as deviation of the tongue towards the opposite side when extended, without muscle atrophy, fasciculations, or fibrillations (see Figure 2-86).
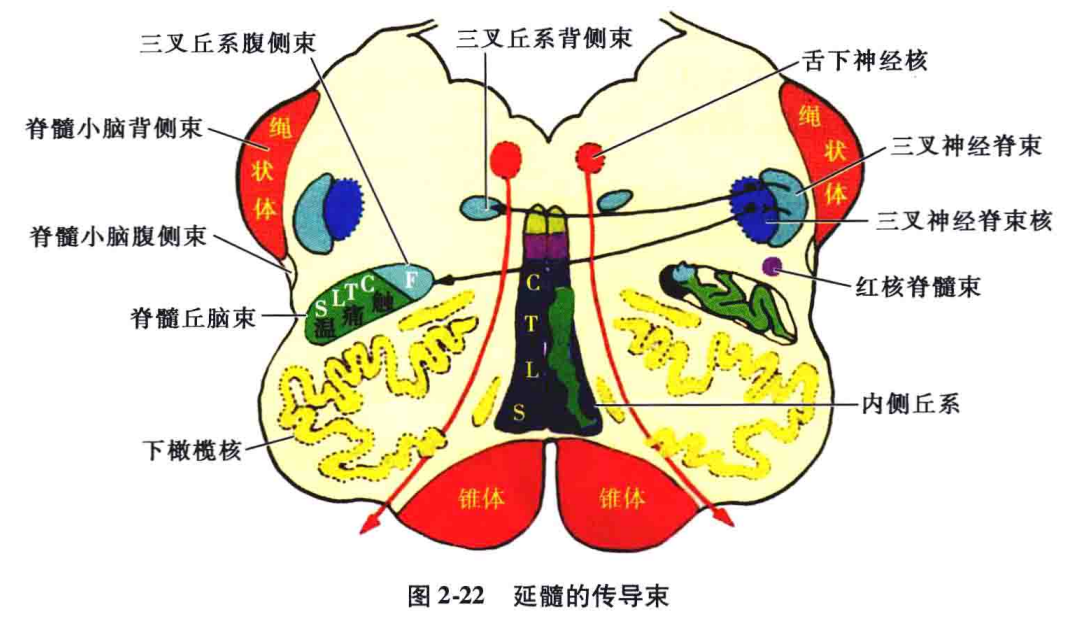
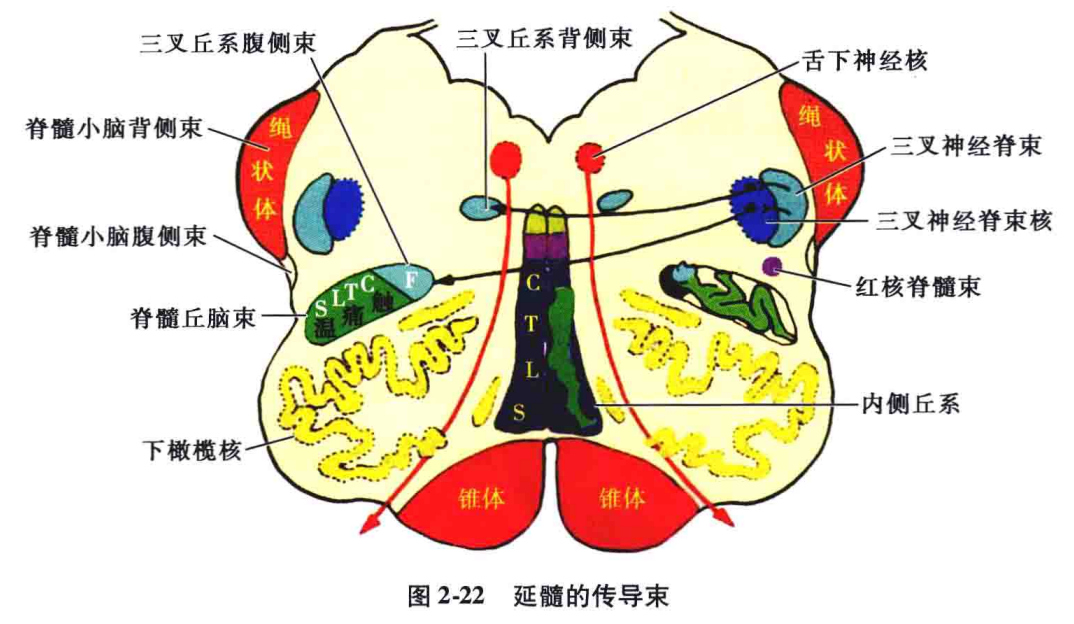
3. Sensory Disorders:Due to the small volume of the medulla, there are ascending medial lemniscus (responsible for deep sensation and touch), spinothalamic tract (responsible for pain and temperature), as well as the trigeminal spinal tract, trigeminal nucleus, and trigeminal lemniscus. These conduction pathways are relatively close together in the medulla, so small lesions can cause sensory impairment on one side or in one type, while larger lesions can cause bilateral or multiple sensory impairments.(1) Deep sensory impairments are often bilateral:Since the bilateral medial lemniscus is located on either side of the midline and is very close together, small lesions near the midline of the medulla can damage both sides of the medial lemniscus, resulting in bilateral deep sensory impairment in the limbs below C1. Some believe that the fibers of the medial lemniscus have a certain arrangement in the medulla, arranged from ventral to dorsal as sacral, lumbar, thoracic, and cervical, which has certain diagnostic significance in clinical practice.(2) Sensory dissociation is relatively common:① Deep and superficial sensory dissociation: The medial lemniscus is close to the midline, while the spinothalamic tract is located laterally. Only when the lesion is of a certain size can it simultaneously damage the fibers of both parts, resulting in complete sensory loss in the limbs on the opposite side. If the lesion is smaller and only damages one of them, it results in deep or superficial sensory impairment in the opposite limb, known as sensory dissociation (or sensory dissociation disorder).② Superficial sensory dissociation: Some believe that in the medulla, the pain fibers in the spinothalamic tract ascend medially, while the temperature fibers ascend laterally (with pain medial and temperature lateral), thus smaller lesions can cause damage to one type of fiber, resulting in the phenomenon of pain and temperature dissociation, known as superficial sensory dissociation.(3) Segmental sensory impairment can occur:In the middle of the medulla, the spinothalamic tract and anterior spinothalamic tract have combined to form the spinothalamic tract. In the medulla, the spinothalamic tract can also be layered, with fibers arranged from anterior lateral to posterior medial, sequentially from sacral, lumbar, thoracic, and cervical fibers, while the ventral trigeminal lemniscus that conveys facial superficial sensation is located posterior medial to the spinothalamic tract. Therefore, small localized lesions may only damage part of these fibers, resulting in segmental pain and temperature sensory disorders (see Figure 2-22). If there is a large lesion completely damaging these fibers, it can result in loss of pain and temperature sensation and reduced touch sensation below the level of C1 on the opposite side.
(4) Sensory impairment of the head and face:1) When the trigeminal spinal tract and nucleus are damaged, pain and temperature sensory impairment can occur in the distribution area of the trigeminal nerve on the same side. If the upper part of the trigeminal spinal tract nucleus is damaged, there will be pain and temperature sensory impairment in the area around the mouth and nose on the same side; if the lower part is damaged, there will be pain and temperature sensory impairment in the peripheral area of the face on the same side; if the middle part is damaged, there will be pain and temperature sensory impairment between the area around the mouth and nose and the peripheral area of the face (onion skin-like distribution) (see Figures 2-87, 2-88).
2) When one side of the trigeminal lemniscus is damaged, it can cause sensory impairment (mainly pain and temperature loss) on the opposite side of the face, and since other structures are also involved, it often accompanies other symptoms (as shown in Figure 2-90).(5) Crossed sensory disorders:When a unilateral medullary lesion damages the trigeminal spinal tract and its nucleus while also damaging the spinothalamic tract, it results in pain and temperature sensory impairment on the same side of the face and on the opposite side of the body, known as crossed sensory disorders (see Figure 2-91).
4. Horner’s SyndromeIn the reticular structure of the medulla, there are descending sympathetic fibers originating from the hypothalamus. When these fibers are damaged, Horner’s syndrome can occur, characterized by miosis, ptosis, and enophthalmos on the same side, accompanied by facial flushing and decreased or absent sweating (the three small and one less) (see Figure 2-92).
5. Cerebellar AtaxiaWhen one side of the spinocerebellar tract and the olive is damaged, ipsilateral cerebellar symptoms and signs can occur. When the lower olive nucleus is damaged, bilateral cerebellar ataxia may occur, and myoclonus may also occur.6. Respiratory DysfunctionThe respiratory center of the medulla is located in the middle and upper segments of the reticular structure, and it is the most important and basic component of the entire respiratory center. The medulla plays a crucial role in maintaining normal breathing, heartbeat, blood pressure, and other vital activities through the vagus nerve nucleus and vagus nerve; thus, the medulla is the center of human life. When the respiratory center of the medulla is destroyed, breathing stops immediately.7. Cardiovascular DysfunctionClinically, due to lesions or damage to the brainstem, especially the medulla, circulatory dysfunction symptoms can occur, such as bradycardia and hypotension due to damage to the heart acceleration center near the depressor area or stimulation of the heart inhibition center due to hematoma, leading to cardiac arrest.(2) Syndromes of Medullary Lesions1. Crossed Upper and Lower Limb Paralysis:This is a rare special type of crossed paralysis. It is caused by a small lesion in the lateral side of the pyramidal decussation, damaging the fibers that have already crossed controlling upper limb muscles and those that have not crossed controlling lower limb muscles, resulting in central paralysis of the upper limb on the same side of the lesion and central paralysis of the lower limb on the opposite side (see Figure 2-82), which can be caused by vascular diseases (for example, thrombosis of the medullary paramedian artery).2. Anterior Olive Syndrome:The lesion is located in the anteromedial part of the lower olive nucleus and can be caused by cerebrovascular diseases or inflammation, including medullary anterior syndrome and medullary paramedian syndrome.(1) Medullary Anterior Syndrome (Hypoglossal Nerve Crossed Paralysis):The lesion mainly damages the pyramid and hypoglossal nerve, manifesting as peripheral paralysis of the hypoglossal nerve on the same side and central paralysis of the upper and lower limbs on the opposite side (see Figure 2-93).
(2) Medullary Paramedian Syndrome (Hypoglossal Nerve Crossed Paralysis and Hemisensory Loss Syndrome):The lesion is located at the level of the ventral olive body, corresponding to the territory supplied by the paramedian artery of the medulla, and the lesion extends to the medial lemniscus and the hypoglossal nerve nucleus, thus damaging the pyramids, hypoglossal nerve roots, medial lemniscus, and hypoglossal nerve nucleus. The clinical manifestations include peripheral paralysis of the hypoglossal nerve on the same side; central paralysis of the upper and lower limbs on the opposite side; and deep sensory impairment of the opposite limb (remember: tongue, pyramid, sensation) (see Figure 2-94).
3. Posterior Olive Syndrome (Medullary Posterior Syndrome):The lesion is located in the lateral area of the medulla posterior to the olive (see Figure 2-95), often caused by tumors or vascular occlusive diseases. Due to the peripheral location of the spinothalamic tract in the lateral area of the medulla, it is often damaged, leading to sensory loss of the opposite limb and temperature loss; since the glossopharyngeal, vagus, and accessory nerve roots emerge from the posterior olive, lesions in the posterior area must also affect these nerves. Depending on the combinations of the cranial nerve roots or their nuclei involved, different syndromes can be formed (as described below).
(1) Glossopharyngeal, Vagus, and Accessory Nerve Syndrome (Schmidt Syndrome): The lesion mainly involves the ambiguus nucleus and accessory nucleus. Clinically, it manifests as paralysis of the pharynx, throat, and soft palate on the same side; paralysis of the sternocleidomastoid and trapezius muscles on the same side; and central paralysis of the upper and lower limbs on the opposite side (see Figure 2-96).
(2) Glossopharyngeal, Vagus, Accessory, and Hypoglossal Nerve Syndrome (Jackson Syndrome): The lesion mainly involves the ambiguus nucleus, accessory nerve nucleus, and hypoglossal nerve nucleus. Clinically, it manifests as paralysis of the pharynx, throat, and soft palate on the same side; paralysis of the sternocleidomastoid and trapezius muscles on the same side; and paralysis of the tongue muscles on the same side (see Figure 2-97).
(3) Glossopharyngeal, Vagus, and Hypoglossal Nerve Syndrome (Tapia Syndrome): The lesion mainly involves the ambiguus nucleus and hypoglossal nerve nucleus. Clinically, it manifests as paralysis of the pharynx, throat, and soft palate on the same side; and paralysis of the tongue muscles on the same side (see Figure 2-98).
(4) Glossopharyngeal, Vagus, Spinothalamic Tract Syndrome (Avellis Syndrome): The lesion mainly involves the ambiguus nucleus, solitary nucleus, and spinothalamic tract. Clinically, it manifests as paralysis of the pharynx, throat, and soft palate on the same side (hoarseness, coughing while drinking, difficulty swallowing, sensory loss in the throat, loss of taste in the posterior 1/3 of the tongue), and pain and temperature sensory impairment in the opposite limb (see Figure 2-99).
4. Lateral Medullary Syndrome (Wallenberg Syndrome):This is the most common syndrome caused by lesions in the medulla, where the lesion is located in the lateral part of the medulla, mainly due to occlusion of the posterior inferior cerebellar artery (or vertebral artery). The main clinical manifestations include five groups of syndromes (remember: sensation, dizziness, ataxia, crossed signs, and Horner’s syndrome) (see Figures 2-100).
(1) Severe dizziness, nausea, vomiting, and nystagmus, due to damage to the vestibular nerve nucleus. (2) Hoarseness, coughing while drinking, difficulty swallowing, and paralysis of the soft palate on the same side of the lesion, due to damage to the ambiguus nucleus and its root fibers, causing paralysis of the glossopharyngeal and vagus nerves. (3) Crossed hemibody sensory impairment, that is, pain and temperature sensory loss on the same side of the face and on the opposite side of the body; this is due to damage to both the trigeminal spinal tract and its nucleus, while also damaging the spinothalamic tract. (4) Ipsilateral limb ataxia, due to damage to the inferior cerebellar peduncle. (5) Horner’s syndrome on the same side, due to damage to the sympathetic fibers descending from the hypothalamus through the reticular structure of the medulla.5. Medullary Hemisyndrome:(1) Cestan-Chenais Syndrome: ① Ipsilateral cerebellar ataxia (damage to the olive or spinocerebellar tract); ② Horner’s syndrome on the same side (damage to the descending sympathetic fibers); ③ Sensory impairment on the same side of the face (damage to the trigeminal spinal tract and nucleus); ④ Paralysis of the pharynx, throat, and soft palate on the same side (damage to the ambiguus nucleus); ⑤ Central paralysis of the opposite limb; ⑥ Pain and temperature sensory impairment below the neck on the opposite side (see Figure 2-102).
(2) Babinski-Nageotte Syndrome: ① Ipsilateral cerebellar ataxia and tilting phenomenon (damage to the olive); ② Horner’s syndrome on the same side (damage to the descending sympathetic fibers); ③ Pain and temperature sensory impairment on the same side of the face (damage to the trigeminal spinal tract); ④ Pain and temperature sensory impairment below the neck on the opposite side (damage to the spinothalamic tract); ⑤ Central paralysis of the opposite upper and lower limbs (damage to the pyramidal tract) (see Figure 2-103).
(3) Common Symptoms and Syndromes of Medullary Lesions(Table 2-2)(1) Symptoms of Pons Lesions1. Motor Disorders:Lesions in the pons can damage the corticospinal tract, corticobulbar tract, facial nerve, abducens nerve, trigeminal motor nucleus, and their fibers and the cortical center for eye movement. Therefore, when lesions occur in the pons, cranial nerve paralysis, upper and lower limb paralysis, and lateral eye movement disorders can occur. Lesions in the upper part of the pons can present as central facial paralysis, tongue paralysis, and upper and lower limb paralysis on the opposite side of the lesion; while lesions in the lower part of the pons can present as peripheral facial paralysis and abducens nerve paralysis on the same side of the lesion, central paralysis of the hypoglossal nerve and upper and lower limbs on the opposite side (Millard-Gubler Syndrome). Bilateral lesions in the ventral part of the pons can lead to complete or incomplete damage to the corticospinal tract and corticobulbar tract, resulting in central paralysis of the limbs and pseudobulbar paralysis. Damage to the abducens nerve nucleus can lead to lateral gaze paralysis, where the eyes cannot gaze towards the lesion side, while gazing towards the opposite side (the side of the paralysis of the limbs, for example, when a lesion occurs in the dorsal part of the pons, it presents as Foville syndrome, characterized by peripheral facial paralysis and lateral gaze paralysis on the same side of the lesion, with central paralysis of the hypoglossal nerve and upper and lower limbs on the opposite side).
2. Sensory Disorders:In the pons, the trigeminal lemniscus, spinothalamic tract, and medial lemniscus are all crossing fibers, so sensory disorders often occur on the opposite side of the lesion. The main sensory nucleus of the trigeminal nerve is located in the middle-upper part of the pons, and when lesions occur near the trigeminal sensory main nucleus, crossed sensory disorders can occur, meaning loss of touch on the same side of the face and pain and temperature sensory loss on the opposite side of the body. In the lower part of the pons, the spinothalamic tract and medial lemniscus are far apart, while in the upper part of the pons, the spinothalamic tract is located in the dorsal lateral part of the medial lemniscus. Therefore, most patients with lesions in the pons present with dissociative sensory disorders, meaning that deep sensory impairment or pain and temperature sensory impairment occur separately, while simultaneous impairment of deep and superficial sensations is relatively rare.
3. Cranial Nerve Paralysis:(1) Trigeminal Nerve: ① Damage to the trigeminal sensory main nucleus and its fibers leads to loss of touch on the same side of the face, reduced or absent corneal reflex, and sometimes corneal inflammation; ② Damage to the upper part of the trigeminal spinal tract nucleus leads to pain and temperature sensory loss in the central part of the face on the same side; ③ Damage to the trigeminal motor nucleus and its intramedullary fibers leads to paralysis of the masseter muscle on the same side, causing the jaw to deviate towards the lesion side when the mouth is opened.
(2) Abducens Nerve: Damage to the abducens nucleus can lead to paralysis of the abducens nerve on the same side, manifesting as strabismus, diplopia, and inability to abduct the eye, often accompanied by peripheral facial paralysis on the same side.
(3) Facial Nerve: Damage to the facial nerve nucleus and its intramedullary fibers leads to peripheral facial paralysis on the same side. If there is an external lesion stimulating the facial nerve, it may cause muscle spasms on the side of the lesion.
(4) Auditory Nerve: One side of the auditory nerve transmits impulses to the central nervous system through both sides of the brainstem, so unilateral brainstem lesions do not cause auditory impairment. Auditory nerve lesions are more common outside the brainstem, especially in the cerebellopontine angle (inflammation, tumors), stimulating lesions of the auditory nerve often cause tinnitus, while destructive lesions can lead to hearing loss or even complete deafness.
4. Cerebellar Ataxia:When the pontine nuclei, superior cerebellar peduncle (brachium conjunctivum), middle cerebellar peduncle (brachium pontis), and inferior cerebellar peduncle (rope body, located in the lateral part of the lower pons and upper medulla) are damaged, cerebellar symptoms and signs can occur, primarily on the same side, but can also affect the opposite side, resulting in cerebellar ataxia.
5. Central Hyperthermia:Due to damage to the pons, hyperthermia can occur due to the loss of control from the hypothalamus temperature regulation center.
6. Mental Symptoms and Sleep Disorders:When lesions occur in the pons, they can cause mental disorders, intellectual impairment, and sleep disorders due to damage to the reticular structure of the brainstem.
(2) Syndromes of Pons Lesions
1. Posterior Inter-Nuclear Ophthalmoplegia:This is caused by damage to the posterior part of the medial longitudinal fasciculus, which is the part of the corticobulbar tract that mediates head turning and eye movement, or the medial longitudinal fasciculus connecting the lateral gaze centers to the abducens nerve nucleus. Clinically, it presents as an inability to perform lateral eye movement on the side of the lesion, while the medial rectus muscles function normally during lateral eye movement or convergence. There is no significant strabismus during straight gaze, nor diplopia; only during lateral gaze towards the lesion side does diplopia, abduction paralysis, and dissociative nystagmus appear (i.e., the healthy eye moves more than the affected eye) (see Figure 2-104).
To help everyone remember, I simplified a diagram, a “Y” diagram (because it is simplified, the anatomy is not very rigorous).
Now, let’s take a look at Anterior Inter-Nuclear Ophthalmoplegia:
2. One-and-a-half Syndrome (Figure 2-105):It is caused by damage to the medial longitudinal fasciculus originating from the abducens nerve nucleus, which immediately crosses to the opposite side after leaving the abducens nerve nucleus, closely adjacent to the accessory abducens nerve nucleus and the abducens nerve nucleus. Lesions in the medial part of the pons can simultaneously affect one side of the abducens nerve nucleus and the fibers crossing from the opposite side.Damage to the abducens nucleus on the same side leads to paralysis of lateral gaze towards that side. Damage to the medial longitudinal fasciculus leads to internuclear ophthalmoplegia. A left-sided pontine lesion causes left-sided lateral gaze paralysis and left-sided internuclear ophthalmoplegia, presenting as complete lateral gaze paralysis towards the left side, and the left eye cannot adduct when gazing to the right (the right side is equivalent to “one-and-a-half syndrome”). The most common causes are cerebral infarction and demyelinating diseases.
Let’s look at the simplified version of One-and-a-half Syndrome:
Remembering how to draw the “Y” diagram is quite helpful and unforgettable.
3. Medullary Basal Medial Syndrome (Foville Syndrome):Lesions in the medial part of the base of the pons, this syndrome is commonly seen due to vascular diseases (occlusion of the pontine paramedian artery) or inflammation and tumors. Lesions damage the pyramidal tract, abducens nerve, and medial longitudinal fasciculus. Clinically, it presents as paralysis of the abducens nerve on the same side; central paralysis of the hypoglossal nerve and upper and lower limbs on the opposite side, hence this syndrome is also called crossed facial paralysis (see Figure 2-107). If the corticobulbar tract is damaged, it can cause contralateral (or bilateral) limb ataxia, hypotonia, etc.; if the lesion involves the medial part of the tegmentum, it can affect the medial lemniscus, resulting in deep sensory impairment in the opposite limb; if the pontine nuclei are damaged, it can also lead to lateral gaze paralysis, where both eyes cannot gaze towards the side of the lesion, and both eyes deviate towards the healthy side.
4. Pontine (Basal) Lateral Syndrome (Millard-Gubler Syndrome):Lesions in the lower lateral part of the pons, often caused by inflammation, tumors, etc., vascular diseases are less common. Lesions damage the pyramidal tract, corticobulbar tract, facial nerve roots or nuclei, presenting with peripheral facial paralysis on the same side of the lesion and central paralysis of the hypoglossal nerve and upper and lower limbs on the opposite side, hence this syndrome is also called crossed facial paralysis (see Figure 2-108). If the lesion expands to damage the abducens nerve root, symptoms of abducens nerve paralysis may occur.
5. Pontine Tegmental Syndrome (Raymond-Cestan Syndrome):Lesions are located in the upper part of the pons (above the facial nerve nucleus and abducens nerve nucleus), which can be caused by vascular diseases (branches of the superior cerebellar artery) or tumors. Its main symptoms are as follows: damage to the medial lemniscus and lateral spinothalamic tract leads to sensory loss on the opposite side of the body and facial sensory loss on the same side; damage to the trigeminal motor nucleus can lead to paralysis of the chewing muscles; damage to the central tegmental tract can lead to muscle atrophy; damage to the medial longitudinal fasciculus can cause nystagmus; and when the brachium conjunctivum is involved, it can lead to cerebellar ataxia on the same side (see Figure 2-109).
6. Common Symptoms and Syndromes of Pons Lesions(Table 2-3)(1) Symptoms of Midbrain Lesions1. Motor Disorders:When one side of the midbrain, especially the ventral part, is damaged, it leads to central paralysis of the opposite side, namely central facial nerve paralysis, central hypoglossal nerve paralysis, and central upper and lower limb paralysis, similar to the same-side hemiplegia caused by lesions in the internal capsule and cerebral hemisphere.However, when lesions occur in the midbrain cerebral peduncles, the resulting hemiplegia often also involves damage to the myelinated fibers of the oculomotor nerve or the myelinated root of the oculomotor nerve, resulting in combined oculomotor nerve paralysis, known as Weber syndrome, characterized by oculomotor nerve paralysis on the same side of the lesion and central hemiplegia of the opposite side (as described later).2. Sensory Disorders:In the dorsal lateral part of the midbrain, the medial lemniscus and spinothalamic tract are very close together, so small lesions in the midbrain can damage both the medial lemniscus and spinothalamic tract simultaneously, causing sensory impairment in the opposite limb.3. Eye Movement Disorders:The midbrain contains the oculomotor nerve nucleus, trochlear nerve nucleus, and their outgoing nerve fibers. In the dorsal part of the tectum, there is also the second-level center for vertical eye movements. If any of these four parts are damaged, corresponding eye movement disorders and abnormal pupil changes will occur.(1) Oculomotor Nerve Paralysis:The oculomotor nerve nucleus is located in the ventral part of the midbrain at the level of the superior colliculus, and the nuclei are relatively long and close together, so lesions affecting the oculomotor nerve nucleus often involve both sides, and complete lesions are rare. Therefore, lesions of the oculomotor nerve nucleus are often bilateral and incomplete.Oculomotor nerve paralysis manifests as: ptosis, external strabismus, diplopia, dilated pupils, loss of direct and consensual light reflexes, and significant restrictions on upward and inward movements of the eye.(2) Trochlear Nerve Paralysis:The trochlear nerve nucleus is located in the central gray matter at the level of the midbrain below the oculomotor nerve nucleus, and the fibers from the trochlear nerve nucleus wrap around the central gray matter and descend to exit the brain at the level of the midbrain. Therefore, paralysis of the trochlear nerve can lead to contralateral trochlear nerve paralysis. If accompanied by oculomotor nerve damage, it will also present with the same side oculomotor nerve paralysis, known as oculomotor-trochlear nerve cross paralysis, but isolated trochlear nerve paralysis is rare.Trochlear nerve paralysis leads to limited eye movement, with the affected eye showing reduced ability to move down and outward, often accompanied by diplopia.
3. Vertical Eye Movement Disorders:The superior colliculus is the cortical center for vertical eye movements. Stimulation of the upper part of the superior colliculus can result in vertical nystagmus, while destructive lesions can lead to paralysis of vertical eye movements.4. Pupil Abnormalities:When lesions damage the constrictor nucleus and its fibers, it leads to pupil dilation on the same side of the lesion, with weakened or absent light reflexes. If the lesion affects the anterior region of the tectum (the light reflex center), it can cause a unilateral or bilateral loss of the pupillary light reflex, with the accommodation reflex remaining intact, known as Argyll-Robertson pupils (see Figure 2-54).
5. Cerebellar Ataxia:The cerebellar superior peduncle crosses at the lower end of the midbrain, so when lesions occur in one side of the superior cerebellar peduncle, cerebellar ataxia may occur on the opposite side. If lesions occur in the lower olive nucleus, bilateral cerebellar ataxia may occur, and myoclonus may also occur.6. Involuntary Movements:The midbrain contains the red nucleus and substantia nigra. When these areas are damaged, involuntary movements can occur.
7. Muscle Tone Changes:When lesions damage the cerebral peduncles, acute lesions may present with flaccid paralysis (acute shock), while lesions that are recovering or have a chronic onset may present with spastic paralysis (characterized by increased muscle tone); when lesions occur in the red nucleus, increased muscle tone may occur on the opposite side (as seen in Parkinson’s disease).
8. Decerebrate Rigidity:When midbrain lesions occur, decerebrate rigidity can occur, characterized by rigidity of the limbs, shoulder internal rotation, arm adduction, elbow extension, forearm pronation, and extension of the wrist joints, with the legs extended and the neck hyperextended, accompanied by irregular breathing, generalized muscle spasms or fasciculations, chills, fever, and sweating. Decerebrate rigidity can be complete or incomplete, unilateral, symmetrical, or asymmetrical, and can occur spontaneously or be induced by painful stimuli.
9. Mental and Sleep Disorders:When midbrain lesions occur, they can cause mental disorders, intellectual impairment, and sleep disorders due to damage to the ascending reticular activating system.
(2) Syndromes of Midbrain Lesions
1. Cerebral Peduncle Syndrome (Weber Syndrome):This syndrome is also known as midbrain ventral syndrome or oculomotor nerve crossed hemiplegia, characterized by lesions located in the ventral part of the midbrain, damaging the oculomotor nerve and the pyramidal tract located in the middle of the cerebral peduncle. It manifests as oculomotor nerve paralysis on the same side of the lesion, central facial paralysis, tongue paralysis, and central upper and lower limb paralysis (see Figure 2-111). Common causes include cerebral thrombosis, inflammation, tumors, trauma, and early tentorial herniation.
2. Red Nucleus Syndrome (Benedikt Syndrome):This syndrome is also known as oculomotor nerve crossed extrapyramidal syndrome, resulting from lesions on one side of the midbrain tegmentum, affecting the oculomotor nerve fibers, red nucleus, substantia nigra, and even the brachium conjunctivum, leading to oculomotor nerve paralysis on the same side, incomplete hemiplegia on the opposite side, and tremors or chorea on the opposite side (see Figure 2-112).
3. Claude Syndrome (Oculomotor Nerve Crossed Red Nucleus Syndrome):This syndrome can also be referred to as oculomotor nerve crossed cerebellar syndrome, first reported in 1912 by Claude. It involves lesions in the midbrain tegmentum near the cerebral aqueduct, along with severe damage to the brachium conjunctivum. Clinically, it presents as oculomotor nerve paralysis on the same side, and cerebellar ataxia symptoms and signs on the opposite side, such as impaired finger-nose test, impaired finger-finger test, impaired rapid alternating movements, and impaired heel-knee-shin test, with varying degrees of trunk ataxia (see Figures 2-113 to 115).
4. Common Symptoms and Syndromes of Midbrain Lesions(Table 2-5)
| Symptom Group | Lesion | Symptoms of Unilateral Lesion | Disease | |
| Same Side | Opposite Side | |||
| Oculomotor Nerve Crossed Hemiplegia (Weber Syndrome) (see Figure 2-111) |
Cerebral Peduncle Base 1. Oculomotor Nerve 2. Corticobulbar Tract 3. Corticospinal Tract |
1. Oculomotor Nerve Paralysis |
2. Central Facial and Tongue Paralysis 3. Central Hemiplegia |
Cerebral Thrombosis, Inflammation, Tumor, Trauma, Tentorial Herniation |
| Red Nucleus (Claude Syndrome) (see Figure 2-113) |
Red Nucleus Area 1. Oculomotor Nerve Myelinated Fibers 2. Red Nucleus |
1. Oculomotor Nerve Paralysis | 2. Cerebellar Ataxia, Tremors | Cerebral Thrombosis, Aneurysm, Trauma, Tumor |
| Red Nucleus (Benedikt Syndrome) (see Figure 2-112) |
Lower Red Nucleus 1. Oculomotor Nerve Myelinated Fibers 2. Substantia Nigra |
1. Oculomotor Nerve Paralysis | 2. Tremors, Chorea, Hand-foot Dyskinesia | Cerebral Thrombosis, Cerebral Hemorrhage, Trauma, Tumor |
| Upper Red Nucleus Syndrome (see Figure 2-116) |
Red Nucleus and Thalamus Subthalamic Nucleus |
Pupil Constriction, Irregular Edges, Eye Tremors | Intentional Tremors, Reduced Muscle Tone | Vascular Disease |
| Quadrigeminal Body Syndrome (see Figure 2-16) |
Superior Colliculus Tectum Inferior Colliculus Tectum |
Early Vertical Nystagmus, Late Vertical Gaze Paralysis, Inability to Converge Auditory Impairment |
Colloid Tumor, Pineal Tumor, Encephalitis, Multiple Sclerosis | |
| Midbrain Reticular Structure Syndrome | Tegmental Area | False Hallucinations, Sleep Disorders, Consciousness Disorders, Decerebrate Rigidity | Vascular Disease, Inflammation, etc. |
Book: “Illustrated Diagnosis of Central Nervous System Diseases”, “Clinical Neurology” (2nd Edition)
Related Reading:Introduction to Brainstem Syndromes [Easy-to-Remember Simplified Version]
