Differential diagnosis of dementia has always been a challenge in neurology. Due to the overlap of symptoms from various causes, this process is particularly complex. However, accurate differential diagnosis is crucial for developing early personalized treatment strategies. On July 4th, Nature Medicine reported “AI-based differential diagnosis of dementia etiologies on multimodal data“ which introduced an AI model that utilizes multimodal data for identifying the causes of dementia. This model integrates demographic information, personal and family medical history, medication usage, neuropsychological assessments, functional evaluations, and multimodal neuroimaging data to identify the causes of individual dementia cases.The study involved 51,269 participants from nine independent, geographically diverse datasets, helping to identify ten different causes of dementia. Even with incomplete data, the model ensures robust predictions.The model achieved an AUROC of 0.94 in distinguishing between normal cognition, mild cognitive impairment, and dementia individuals, with an AUROC of 0.96 for differentiating dementia etiologies. For mixed dementia cases, the model’s average AUROC was 0.78. In a randomly selected group of 100 cases, neurologists’ assessments assisted by the AI model had an AUROC 26.25% higher than those assessed alone. Additionally, the model’s predictions were consistent with biomarker evidence, validated by autopsy results showing associations with different protein pathologies.The framework has the potential to serve as a dementia screening tool in clinical settings and drug trials, but further prospective studies are needed to confirm its ability to improve patient care.
Dementia is one of today’s most urgent health challenges. Nearly 10 million new cases are reported each year, characterized by a gradual decline in cognitive function that severely impairs daily life, presenting significant clinical and socioeconomic challenges. In 2017, the World Health Organization’s global action plan emphasized that timely and accurate diagnosis of dementia is a key strategic goal in addressing the increasing number of global dementia cases. Given the aging global population and the need for more accurate participant screening in drug trials, the precision of dementia diagnosis remains a critical yet unmet need. This challenge primarily arises from the overlapping clinical presentations of different types of dementia, compounded by the heterogeneity of magnetic resonance imaging (MRI) results. As the shortage of specialists (including neurologists, neuropsychologists, and geriatric care providers) exacerbates, the necessity for improved diagnostic tools becomes increasingly urgent.
 With the global aging population, the incidence of dementia is continuously rising, making early and accurate diagnosis particularly important. This study presents an AI model that utilizes multimodal data for identifying the causes of dementia, providing personalized diagnostic information through the integration of various data sources.
Dementia is a severe cognitive impairment that affects patients’ daily lives. Common types of dementia include Alzheimer’s Disease (AD), Vascular Dementia (VD), and Lewy Body Dementia (LBD). Due to the overlap in clinical presentations of different types of dementia, traditional diagnostic methods (such as clinical evaluations, neuropsychological tests, and MRI) face difficulties in distinguishing these etiologies. Furthermore, the shortage of specialists exacerbates the diagnostic challenges.
In recent years, machine learning (ML) technologies have been increasingly applied in medical diagnostics. Particularly, ML methods utilizing neuroimaging data and other clinical information have shown potential in identifying and distinguishing types of dementia. However, most existing ML methods primarily focus on distinguishing normal cognition (Normal Cognition, NC), mild cognitive impairment (Mild Cognitive Impairment, MCI), and dementia (Dementia, DE), without adequately considering the complexity and coexistence of multiple dementia etiologies.
This study proposes a multimodal ML framework that comprehensively analyzes multiple data sources, including demographic information, personal and family medical history, medication usage, neuropsychological assessments, functional evaluations, and multimodal neuroimaging data, for the differential diagnosis of dementia. The research data comes from nine independent, geographically diverse cohorts, totaling 51,269 participants.
The data comes from the National Alzheimer’s Coordinating Center (NACC), Alzheimer’s Disease Neuroimaging Initiative (ADNI), and other nine cohorts. These datasets provide extensive detailed information about patients, including demographic data, medical history, medication usage, neuropsychological test results, and neuroimaging data.
Participants include individuals with normal cognition (NC), mild cognitive impairment (MCI), and dementia (DE). Specifically, the NACC dataset includes 17,242 normal cognition individuals, 7,582 mild cognitive impairment individuals, and 16,131 Alzheimer’s disease patients.
Multimodal data includes MRI scans, neuropsychological tests, demographic information, etc. MRI data encompasses various scanning modalities such as T1-weighted, T2-weighted, FLAIR, DWI, and SWI, to comprehensively capture structural and functional information of the brain.
The model utilizes a Transformer architecture to process various diagnostic data. Each data type is first converted into fixed-length vectors, which are then analyzed comprehensively through the transformer to output the probability for each etiology. The core of the transformer architecture is its ability to effectively handle sequential data and capture complex relationships within the data through self-attention mechanisms.
Random feature masking techniques are employed to handle incomplete data, ensuring the model’s robustness under varying data availability conditions. In practical applications, clinical data is often incomplete, so the model needs to maintain high accuracy even with missing portions of data.
The model’s performance was validated across ten different dementia etiologies, evaluating its ability to distinguish between normal cognition, mild cognitive impairment, and dementia individuals. Specifically, the model excels in differentiating between Alzheimer’s disease, Lewy body dementia, vascular dementia, frontotemporal degeneration, and other etiologies.
Multiple metrics, including the Pearson correlation coefficient, were used to assess the consistency between the model and neurologists. The study found that the AI model’s predictions were highly consistent with neurologists’ diagnoses, especially in complex cases, where the AI model significantly improved diagnostic accuracy.
With the global aging population, the incidence of dementia is continuously rising, making early and accurate diagnosis particularly important. This study presents an AI model that utilizes multimodal data for identifying the causes of dementia, providing personalized diagnostic information through the integration of various data sources.
Dementia is a severe cognitive impairment that affects patients’ daily lives. Common types of dementia include Alzheimer’s Disease (AD), Vascular Dementia (VD), and Lewy Body Dementia (LBD). Due to the overlap in clinical presentations of different types of dementia, traditional diagnostic methods (such as clinical evaluations, neuropsychological tests, and MRI) face difficulties in distinguishing these etiologies. Furthermore, the shortage of specialists exacerbates the diagnostic challenges.
In recent years, machine learning (ML) technologies have been increasingly applied in medical diagnostics. Particularly, ML methods utilizing neuroimaging data and other clinical information have shown potential in identifying and distinguishing types of dementia. However, most existing ML methods primarily focus on distinguishing normal cognition (Normal Cognition, NC), mild cognitive impairment (Mild Cognitive Impairment, MCI), and dementia (Dementia, DE), without adequately considering the complexity and coexistence of multiple dementia etiologies.
This study proposes a multimodal ML framework that comprehensively analyzes multiple data sources, including demographic information, personal and family medical history, medication usage, neuropsychological assessments, functional evaluations, and multimodal neuroimaging data, for the differential diagnosis of dementia. The research data comes from nine independent, geographically diverse cohorts, totaling 51,269 participants.
The data comes from the National Alzheimer’s Coordinating Center (NACC), Alzheimer’s Disease Neuroimaging Initiative (ADNI), and other nine cohorts. These datasets provide extensive detailed information about patients, including demographic data, medical history, medication usage, neuropsychological test results, and neuroimaging data.
Participants include individuals with normal cognition (NC), mild cognitive impairment (MCI), and dementia (DE). Specifically, the NACC dataset includes 17,242 normal cognition individuals, 7,582 mild cognitive impairment individuals, and 16,131 Alzheimer’s disease patients.
Multimodal data includes MRI scans, neuropsychological tests, demographic information, etc. MRI data encompasses various scanning modalities such as T1-weighted, T2-weighted, FLAIR, DWI, and SWI, to comprehensively capture structural and functional information of the brain.
The model utilizes a Transformer architecture to process various diagnostic data. Each data type is first converted into fixed-length vectors, which are then analyzed comprehensively through the transformer to output the probability for each etiology. The core of the transformer architecture is its ability to effectively handle sequential data and capture complex relationships within the data through self-attention mechanisms.
Random feature masking techniques are employed to handle incomplete data, ensuring the model’s robustness under varying data availability conditions. In practical applications, clinical data is often incomplete, so the model needs to maintain high accuracy even with missing portions of data.
The model’s performance was validated across ten different dementia etiologies, evaluating its ability to distinguish between normal cognition, mild cognitive impairment, and dementia individuals. Specifically, the model excels in differentiating between Alzheimer’s disease, Lewy body dementia, vascular dementia, frontotemporal degeneration, and other etiologies.
Multiple metrics, including the Pearson correlation coefficient, were used to assess the consistency between the model and neurologists. The study found that the AI model’s predictions were highly consistent with neurologists’ diagnoses, especially in complex cases, where the AI model significantly improved diagnostic accuracy.
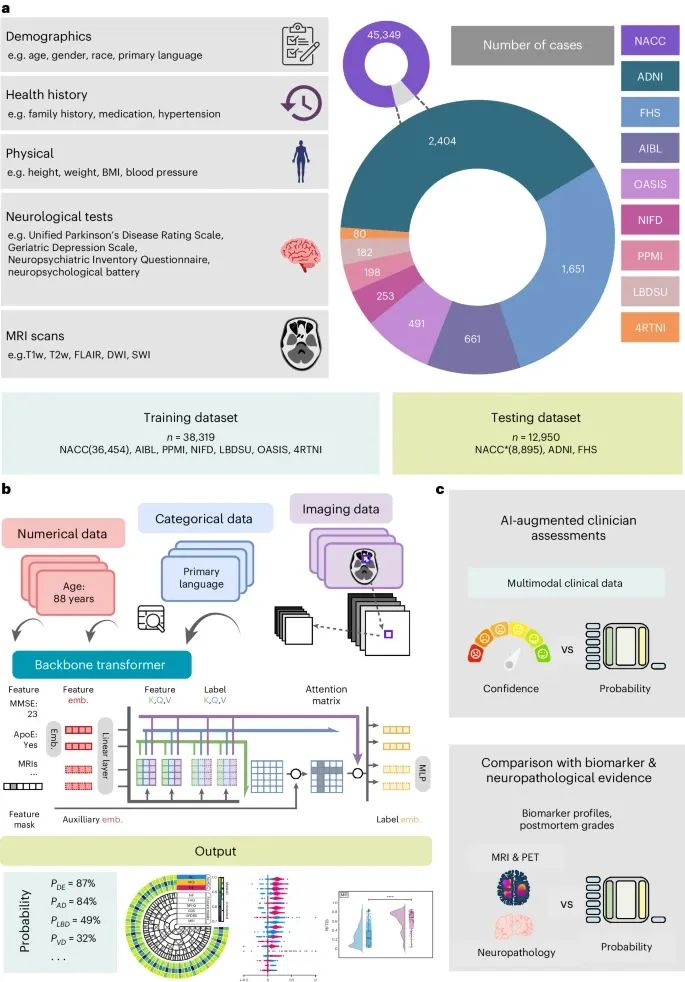
Data, Model Architecture, and Modeling Strategy (Credit: Nature Medicine)
Data Sources: The data for this study comes from nine independent cohorts, including 4RTNI, ADNI, AIBL, FHS, LBDSU, NACC, NIFD, OASIS, and PPMI. These datasets provide a variety of data types, including individual demographic information, health history, neuropsychological test results, physical and neurological examinations, and multi-sequence MRI scans. During model training, data from NACC, AIBL, PPMI, NIFD, LBDSU, OASIS, and 4RTNI were merged for model training; ADNI and FHS datasets were used for external validation.
Model Architecture: The architecture of the model is based on a Transformer, where each feature data is processed into fixed-length vectors through a specific embedding strategy and then fed as input to the transformer. A linear layer connects the transformer and the output prediction layer. To handle data incompleteness, the model employs random feature masking techniques, which simulate arbitrary missing features during training, enhancing the model’s robustness under varying data availability conditions.
Modeling Strategy: The model first converts different types of diagnostic data into fixed-length vectors and conducts comprehensive analysis through the transformer. The self-attention mechanism of the transformer effectively handles sequential data, capturing complex relationships within the data. To validate the model’s effectiveness, the study compared diagnostic performance of neurologists and neuro-radiologists with and without AI assistance. The results indicate that the AI model significantly improved diagnostic accuracy.
In distinguishing between normal cognition, mild cognitive impairment, and dementia individuals, the model achieved an AUROC of 0.94. In validation on the ADNI and NACC datasets, the model achieved AUROCs of 0.94 and 0.96, respectively, demonstrating its robustness across different datasets.
Even with incomplete data, the model maintains high predictive accuracy. For example, in the ADNI dataset, despite 69% of the data being missing, the weighted average AUROC still reached 0.91. This indicates the model’s strong resilience against missing data.
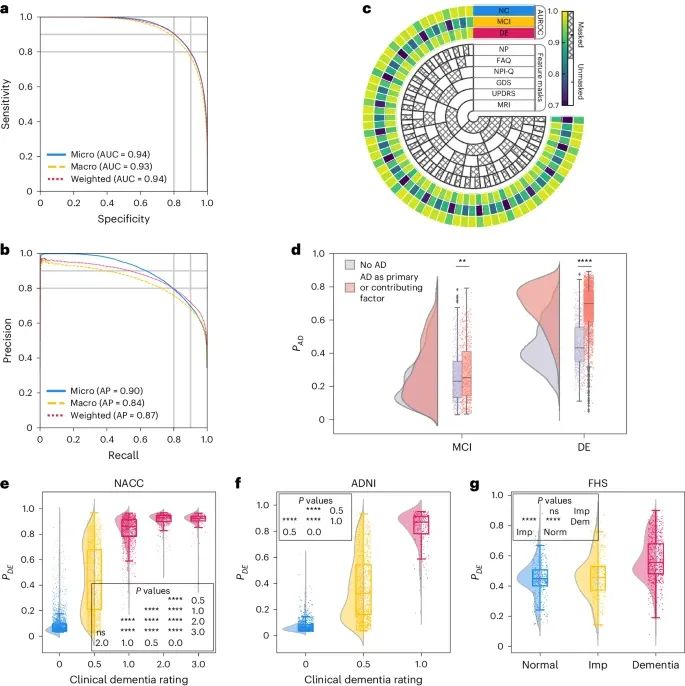
Model Performance (Credit: Nature Medicine)
ROC Curve and PR Curve (a, b): The ROC curve and PR curve show the model’s micro-average, macro-average, and weighted average calculations on normal cognition (NC), mild cognitive impairment (MCI), and dementia (DE) labels. In the test set (including the NACC data not used for training, ADNI, and FHS data), the model demonstrated strong classification ability in classifying NC, MCI, and DE, achieving an AUROC (area under the curve) of 0.94 and an AUPR (area under the precision-recall curve) of 0.90. The macro-average AUROC is 0.93, and the AUPR value is 0.84. The weighted average AUROC and AUPR are 0.94 and 0.87, respectively. These metrics demonstrate the model’s robust performance across different cognitive states.
Performance with Missing Data (c): Schematic diagrams illustrate the model’s varying performance in the presence of missing data. The inner concentric circles represent different scenarios when specific test information is omitted (masked) or included (unmasked). The three outer concentric circles represent the model’s AUROC performance on NC, MCI, and DE labels. Even with missing data such as MRI, Unified Parkinson’s Disease Rating Scale, Geriatric Depression Scale, Neuropsychiatric Inventory Questionnaire, and Functional Activities Questionnaire, the model still produces reliable scores.
Raincloud Plot of Predicting AD Probability (d): The raincloud plot shows the model’s predictions of AD probability for individuals with MCI and DE in the NACC cohort. The Kolmogorov-Smirnov (KS) two-sample two-tailed test compares cases where AD is a cognitive impairment factor with those of non-AD etiology. In the MCI group (n=1,486) and DE group (n=4,085), the KS test results for AD factors were KS=0.09, P=4.29×10^-3 and KS=0.57, P<1×10^-200, indicating a significant impact of AD factors.
Distribution of CDR Scores and Model Predicted Probabilities (e–g): Raincloud plots and violin plots illustrate the relationship between Clinical Dementia Rating (CDR) and model-predicted dementia probabilities across the NACC, ADNI, and FHS cohorts. In the NACC dataset, as CDR scores increase, P(DE) also increases, and the differences across varying cognitive impairment spectra are statistically significant (P<0.0001). In the ADNI dataset, P(DE) shows significant differences between baseline CDR scores and higher scores (P<0.0001). In the FHS dataset, P(DE) shows significant differences between normal, cognitively impaired, and dementia (P<0.0001), but no significant differences were noted between normal and cognitively impaired. This indicates that the model may face challenges in identifying early cognitive decline.
Model Consistency with Biomarkers
The model’s predictions were validated against different protein pathologies through autopsy results. For example, the model accurately identified frontotemporal degeneration (FTD) associated with TDP-43 protein aggregates. In the NACC dataset, the model-predicted FTD probability was highly consistent with the patterns of frontal lobe metabolic decline and atrophy shown by MRI and FDG PET biomarkers.
The model’s predicted probabilities for Alzheimer’s disease (AD) were highly correlated with Aβ, tau, and FDG PET biomarkers. In the NACC and ADNI datasets, AD probabilities in Aβ, tau, and FDG PET positive groups were significantly higher than in negative groups, indicating the model’s diagnostic process is highly consistent with current AD diagnostic ATN standards.
AI-Assisted Clinical Evaluation
In a randomly selected group of 100 cases, neurologists’ assessments assisted by the AI model had an AUROC 26.25% higher than those assessed alone. This indicates that the AI model can significantly enhance diagnostic accuracy for clinicians, especially in complex cases.
AI-assisted evaluations showed significant performance improvements across various dementia etiologies. For instance, in Parkinson’s disease-related dementia (PRD), AI model assistance increased AUROC by 69%, and in traumatic brain injury (TBI), AUROC increased by 72%.
Model Performance in Mixed Dementia Cases
The study found that the model performed excellently in handling mixed dementia cases, achieving an average AUROC of 0.78. This indicates that the model can effectively handle complex situations with multiple coexisting etiologies.
In cases with two coexisting etiologies (such as AD and VD), the model’s AUROC was 0.73, demonstrating high diagnostic accuracy. The study shows that the AI model can effectively differentiate between different etiologies and provide accurate diagnostic suggestions.
This research demonstrates an AI model that integrates multimodal data, effectively distinguishing between various dementia etiologies and providing personalized diagnostic information. Although the findings indicate that the model has high robustness and accuracy across multiple independent cohorts, its generalizability in broader populations and clinical environments still requires further validation. Additionally, future research should further assess the practical application of this model in clinical practice, including its potential in early diagnosis and personalized treatment.
In practical applications, this AI model is expected to significantly enhance the diagnostic accuracy of dementia and the quality of patient care. By integrating multiple data sources, the model not only provides accurate diagnoses but also offers decision support for clinicians, aiding in the formulation of personalized treatment plans. In the future, as more data is accumulated and technologies advance, the application of AI in healthcare will become increasingly widespread, providing new solutions to complex medical challenges.
In summary, the development and application of this AI model provide a new tool for the differential diagnosis of dementia, with broad application prospects, and is expected to significantly enhance the diagnostic accuracy and quality of patient care for dementia. In the future, as technology continues to evolve and improve, AI will play an increasingly important role in healthcare, bringing more benefits to patients.
https://www.nature.com/articles/s41591-024-03118-z
Xue C, Kowshik SS, Lteif D, Puducheri S, Jasodanand VH, Zhou OT, Walia AS, Guney OB, Zhang JD, Pham ST, Kaliaev A, Andreu-Arasa VC, Dwyer BC, Farris CW, Hao H, Kedar S, Mian AZ, Murman DL, O’Shea SA, Paul AB, Rohatgi S, Saint-Hilaire MH, Sartor EA, Setty BN, Small JE, Swaminathan A, Taraschenko O, Yuan J, Zhou Y, Zhu S, Karjadi C, Alvin Ang TF, Bargal SA, Plummer BA, Poston KL, Ahangaran M, Au R, Kolachalama VB. AI-based differential diagnosis of dementia etiologies on multimodal data. Nat Med. 2024 Jul 4. doi: 10.1038/s41591-024-03118-z. Epub ahead of print. PMID: 38965435.
Editor| Explorer
Typesetting| Explorer
Please cite the source from【Bio Exploration】
Understanding Cell Death | 24-Year Cell Review (Long Article Collection Version)
Cell | What Determines the Size of Cells?
Nature | Seven Technologies to Watch in 2024
Nature | Can Autoimmune Diseases Be Cured? Scientists Finally See Hope
Evolution of CRISPR Technology | 24-Year Cell Review