Acute gastrointestinal injury (acute gastrointestinal injury, AGI) is gastrointestinal dysfunction that occurs in critically ill patients during an acute illness. Clinically, it can be divided into four grades.
Critical neurological diseases, whether central nervous system damage or peripheral nervous system damage, can cause AGI as long as there is autonomic nervous damage.
1. Clinical Manifestations
Gastric retention or reflux, abdominal distension and diarrhea, gastrointestinal paralysis, abdominal compartment syndrome, and gastrointestinal bleeding, etc.
AGI Grade I (Risk factors for gastrointestinal dysfunction or failure): Temporary partial gastrointestinal dysfunction with clear etiology, such as early gastrointestinal motility disorders occurring during the acute phase of cerebrovascular disease.
AGI Grade II (Gastrointestinal dysfunction): The gastrointestinal tract does not have complete digestive and absorption functions, unable to meet the body’s needs for nutrients and water, but the gastrointestinal dysfunction does not affect the patient’s general condition, such as gastroparesis with significant gastric retention or reflux caused by autonomic neuropathy, spinal cord injury, etc., lower digestive tract paralysis, diarrhea, abdominal compartment syndrome Grade I (intra-abdominal pressure 12~15mmHg), food intolerance [enteral nutrition not reaching 20kcal/(kg·d) target within 72 hours].
AGI Grade III (Gastrointestinal failure): After intervention, gastrointestinal function still cannot be restored, and the patient’s general condition shows no improvement. For example: persistent food intolerance caused by the use of high doses of anesthetics when terminating status epilepticus, characterized by significant gastric retention, persistent gastrointestinal paralysis, intestinal dilation, intra-abdominal pressure Grade II (intra-abdominal pressure 15~20mmHg) and abdominal perfusion pressure <60mmHg.
AGI Grade IV (Gastrointestinal failure with distant organ dysfunction): Acute gastrointestinal injury gradually progresses, multiple organ dysfunction syndrome and shock worsen progressively, posing a life-threatening risk at any time. For example, severe infection/infectious toxic shock, intestinal ischemic necrosis caused by inappropriate nutritional support, gastrointestinal bleeding leading to hemorrhagic shock, and abdominal compartment syndrome (abdominal compartment syndrome, ACS) requiring active decompression.
1. AGI Grading Treatment Principles
AGI Grade I: In addition to providing sufficient intravenous fluids, no special interventions are needed for gastrointestinal symptoms. Early initiation of enteral nutrition should be started as soon as possible within 24-48 hours after injury. Reduce medications that impair gastrointestinal motility (e.g., catecholamines, opioids, sedatives, muscle relaxants).
AGI Grade II: Certain treatment measures are required to prevent progression to gastrointestinal failure. ① Treatment measures include intra-abdominal pressure therapy; ② Restoration of gastrointestinal function therapy, such as prokinetic agents; ③ Enteral nutrition, if significant gastric retention or reflux occurs, attempts can be made to reduce the amount of enteral nutrition; ④ For patients with gastroparesis who do not respond to prokinetic agents, post-pyloric nutrition is given.
AGI Grade III: Monitor and manage intra-abdominal pressure. ① Exclude other intra-abdominal diseases such as cholecystitis, peritonitis, intestinal ischemia; ② Stop using medications that cause gastrointestinal paralysis as soon as possible; ③ Routine trial of small amounts of enteral nutrition; ④ Avoid early parenteral nutrition (within 7 days before entering ICU) to reduce the incidence of nosocomial infections.
AGI Grade IV: When standard medical treatment is ineffective, emergency laparotomy or other emergency treatments, such as colonoscopic decompression, are required. During treatment, strengthen monitoring and accurately assess AGI grading, timely adjust treatment plans to improve gastrointestinal tolerance and prognosis.
(1) Intra-abdominal Pressure Control
1) Monitoring: Routine monitoring of intra-abdominal pressure (IAP), measuring at least twice within 6 hours, with ≥12mmHg indicating intra-abdominal hypertension (Figure 1). The target for IAP control is <12mmHg.
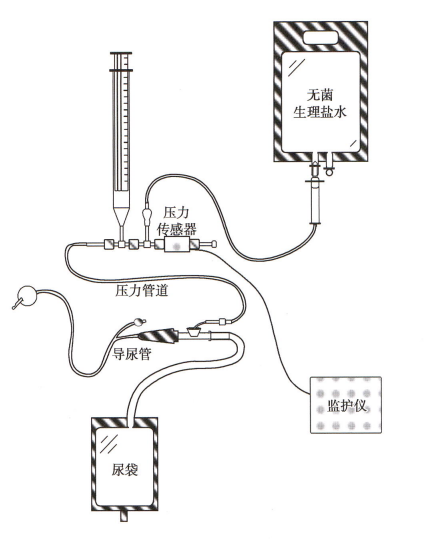 Figure 1: Intra-abdominal Pressure Monitoring Diagram
Figure 1: Intra-abdominal Pressure Monitoring Diagram
2) Treatment: Use nasogastric tube/colonic decompression method to drain gastrointestinal contents. Percutaneous drainage and decompression method to remove ascites. Elevating the head of the bed >20° can increase the risk of intra-abdominal hypertension (IAH), but adjustments should be made considering intracranial pressure increase and aspiration risk. Muscle relaxants can reduce intra-abdominal pressure but are limited in use due to their inhibitory effects on gastrointestinal motility.
ACS refers to sustained elevated intra-abdominal pressure (IAP >20mmHg) with new organ dysfunction. If standard conservative treatment is ineffective, surgical decompression should be performed.
(2) Gastric Residual Volume Control
1) Monitoring: Routine dynamic monitoring of gastric residual volume, adjusting monitoring frequency according to gastric residual volume. A single gastric residual volume >200ml is defined as significant gastric retention.
2) Treatment: Intravenous infusion of metoclopramide and/or erythromycin, without using cisapride. Routine use of prokinetic agents is not recommended. Acupuncture stimulation treatment may promote gastric emptying recovery in neurosurgical critically ill patients. Opioids should be avoided or reduced to lower sedation depth. If a single residual volume >200ml, stop enteral feeding or provide post-pyloric feeding.
1) Monitoring: Routine monitoring of daily bowel movements. More than 3 times a day with watery stools, ≥200g/d; or ≥250ml/d, is classified as diarrhea. Diarrhea can be classified as secretory, osmotic, motility-related, and exudative, and for neurological critically ill patients, it can be categorized as disease-related, food/feeding-related, and drug-related.
2) Treatment: Maintain water-electrolyte balance, hemodynamic stability, and protect tissue-organ perfusion (e.g., correct kidney function impairment caused by hypovolemia). Discontinue laxatives, sorbitol, lactulose, antibiotics, etc., and eliminate factors causing malabsorption or inflammatory bowel disease. For feeding-related diarrhea, reduce the feeding speed and adjust the nutritional formula or increase dietary fiber (to extend food transit time). For diarrhea caused by difficult-to-identify Clostridium, oral vancomycin is preferred over metronidazole.
(4) Gastrointestinal Motility Insufficiency Control
1) Monitoring: Routine monitoring of abdominal distension, decreased bowel sounds, constipation, and other signs of gastrointestinal motility insufficiency, and if necessary, check abdominal X-ray at intervals.
Paralytic ileus refers to impaired intestinal motility leading to fecal retention, clinically manifested as cessation of bowel movements for at least 3 days, with bowel sounds present or absent; supine abdominal X-ray shows generalized gastric and intestinal distension, particularly in the colon (Figure 2), and mechanical obstruction must be excluded.
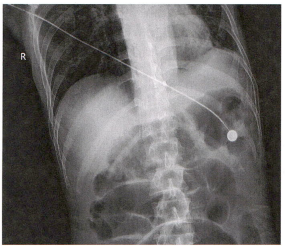 Figure 2: Paralytic Ileus Abdominal X-ray Showing Generalized Gastrointestinal Distension.
Figure 2: Paralytic Ileus Abdominal X-ray Showing Generalized Gastrointestinal Distension.
2) Treatment: Discontinue medications that slow intestinal motility, such as catecholamines, sedatives, and opioids; eliminate factors affecting intestinal motility, such as hyperglycemia, hypokalemia, etc.; provide or prophylactically give laxatives as soon as possible, but routine use of opioid receptor antagonists is not recommended; if necessary, prokinetic agents such as domperidone, metoclopramide, and erythromycin can be used to promote gastric and small intestine motility, or neostigmine to promote small intestine and colon motility, as prokinetic agents have become standard treatment measures for intestinal motility disorders.
Intestinal dilation abdominal X-ray or CT scan shows: colon diameter >6cm (cecum exceeds 9cm) or small intestine diameter >3cm (Figure 3). Major management measures include maintaining water-electrolyte balance and gastrointestinal decompression. When the cecum diameter >10cm, and no improvement within 24 hours, after excluding mechanical obstruction, intravenous infusion of neostigmine; when the cecum diameter >10cm, and conservative treatment shows no improvement within 24-48 hours, colonoscopic decompression is performed, with an effective rate of up to 80%, but there is a certain risk of colon perforation; when the cecum diameter ≤12cm, combined colonoscopic decompression treatment can be sustained for 48-72 hours. When the above standard medical treatments are ineffective, surgical intervention is performed to prevent intestinal perforation.
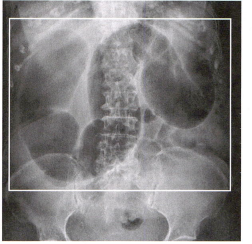 Figure 3: Intestinal Dilation Abdominal X-ray Showing Small Intestine Dilation, Diameter >3cm.
Figure 3: Intestinal Dilation Abdominal X-ray Showing Small Intestine Dilation, Diameter >3cm.
(5) Food Intolerance Control
1) Monitoring: Feeding intolerance syndrome (FI) is based on clinical assessment, without a precise definition. When enteral nutrition fails to reach the energy supply target of 20kcal/(kg·d) for 72 consecutive hours, or enteral nutrition is stopped for any clinical reason, it is considered FI. FI often requires clinical intervention to maintain or adjust gastrointestinal function.
2) Treatment: Limit the use of medications that impair intestinal motility; provide prokinetic agents and/or laxatives; control intra-abdominal pressure; attempt small amounts of enteral nutrition, and if necessary, supplement with parenteral nutrition. Compared to early parenteral nutrition, delaying parenteral nutrition by a week can promote recovery.
Logistic regression analysis shows that AGI is an independent risk factor for mortality in critically ill patients. The mortality rate of critically ill patients with AGI is significantly higher than that of patients without AGI (37.74% vs 4.03%). The mortality rates corresponding to different AGI grades are: AGI Grade II 5.08%; AGI Grade III 30%; AGI Grade IV 71.05%; AGI Grade IV 89.66%.
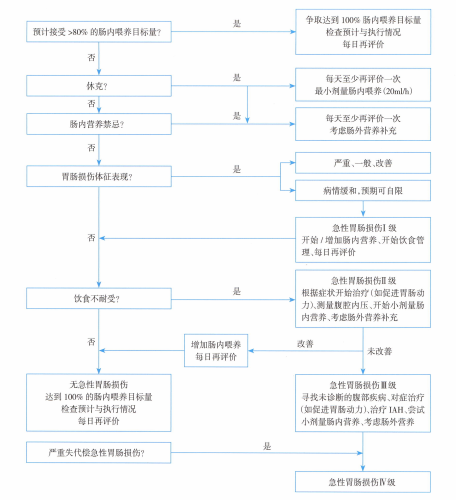
Diagnosis and Treatment Process