A 60-year-old male patient was admitted due to diplopia. He had a history of hypertension for 10 years, intermittently taking antihypertensive medication without monitoring blood pressure.
On the first day of illness, he suddenly experienced diplopia while playing ball, which was more pronounced in the right eye. On the afternoon of the second day, blood pressure measured at a community health center was 150/85 mmHg (1 mmHg = 0.133 kPa), and he was given “Ginkgo biloba capsule 2 capsules”.
On the third day, he woke up with aggravated diplopia and experienced limited eye movement and unsteady walking.
Physical examination: Blood pressure was 182/102 mmHg, consciousness clear, speech fluent, pupils equal and reactive to light, right eye deviated outward, right eye adduction and downward gaze were limited, left eye showed horizontal nystagmus on left gaze, diplopia on right gaze, symmetrical forehead wrinkles, slightly shallow left nasolabial fold, mouth corner slightly deviated to the right, tongue extended in the midline, neck without resistance, negative meningeal signs. Muscle strength and tone in the limbs were normal, tendon reflexes were symmetrical, pinprick sensation was consistent and symmetrical in both limbs, and no pathological signs were elicited bilaterally.
Random blood sugar was 20.60 mmol·L-1.
Head MRI + DWI + MRA (Figure 1): Old cerebral infarcts in the right pons, left basal ganglia area, left thalamus, and left deep frontal lobe; multiple chronic ischemic lesions in bilateral frontal and parietal lobes and around the bilateral lateral ventricles; abnormal signals in both bridge arms; and arteriosclerotic changes in cerebral blood vessels.
After admission, the patient was given oral enteric-coated aspirin 0.1 g·d-1 (Bayer Healthcare), atorvastatin calcium 20 mg·d-1 (Pfizer), and butylphthalide soft capsules 0.6 g·d-1 (Shijiazhuang Pharmaceutical Group Enbip Pharmaceutical Co., Ltd.), and intravenous infusion of Shenxiong glucose injection 6 ml·d-1 (Mudanjiang Youbo Pharmaceutical Co., Ltd.), brain-glycosylated peptide injection 6 ml·d-1 (Jilin Sihuan Pharmaceutical Co., Ltd.), and edaravone injection 60 mg·d-1 (Nanjing Xiansheng Dongyuan Pharmaceutical Co., Ltd.). Blood sugar fluctuations were monitored between 11~21 mmol·L-1, and metformin hydrochloride tablets 1.5 g·d-1 (Zhongmei Shanghai Bristol-Myers Squibb Pharmaceutical Co., Ltd.) and repaglinide tablets 1.5 g·d-1 (Novo Nordisk, Denmark) were given for treatment.
On the night of the third day of illness (the day of admission), the patient’s diplopia transiently alleviated, and eye movement became free, with diplopia disappearing. However, on the fourth day of illness, diplopia symptoms reappeared, accompanied by right eyelid ptosis, covering the pupil, slightly dilated right pupil, right eye in an abducted position, and left limb ataxia, unable to walk independently.
On the ninth day of illness, the physical examination revealed clear consciousness, fluent speech, right pupil approximately 3 mm, left pupil approximately 2.5 mm, slightly sluggish light reflex on the right side, sensitive light reflex on the left side, right eyelid ptosis covering the pupil at the 3 o’clock position, right eye in an abducted position, adduction, and upward and downward gaze limited, left eye unable to abduct fully, exposing 2 mm of sclera, no nystagmus, diplopia on right gaze, inability to converge, symmetrical forehead wrinkles, slightly shallow left nasolabial fold, mouth corner slightly deviated to the right, tongue extended in the midline, muscle strength and tone in the limbs were normal, left limb finger-to-nose test and heel-to-shin test were unstable, unable to tandem walk, and positive Romberg’s sign, with no pathological signs elicited bilaterally.
On the ninth day, a follow-up head MRI + DWI (Figure 2) showed acute cerebral infarction in the right midbrain and cerebral peduncle. After acupuncture treatment, on the 23rd day of illness (at discharge), the patient’s eye movement improved compared to before, able to adduct to the midline, and left limb coordination improved, allowing him to walk independently.
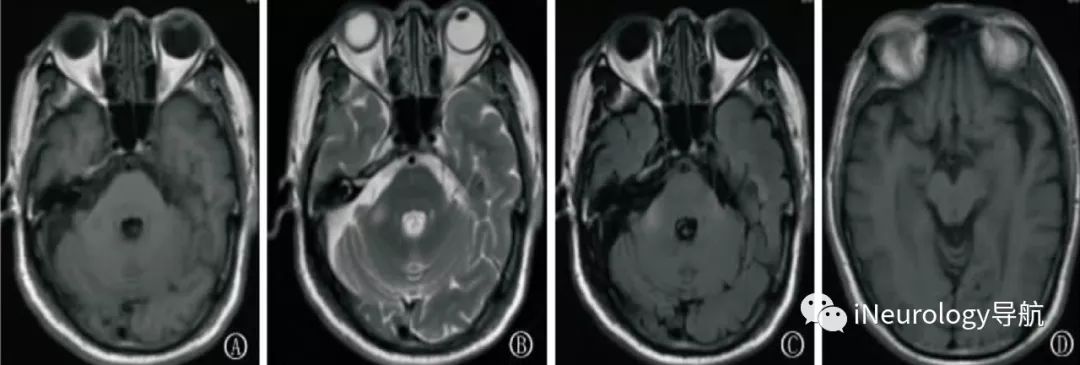
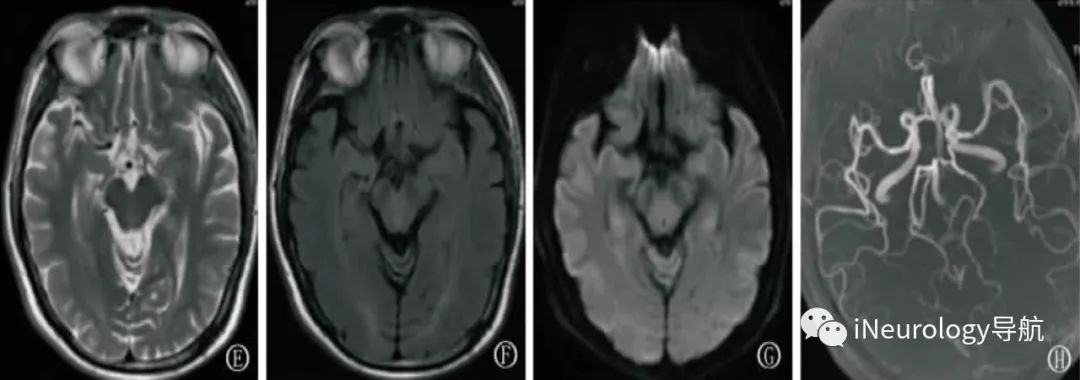
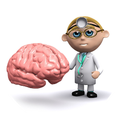
Figure 1:Head MRI + DWI + MRA on the third day of illness.
Figures A, B, C show bilateral bridge arms with long T1 and long T2 high FLAIR abnormal signals; Figures D, E, F, G show no obvious abnormal signals; Figure H indicates cerebral vascular arteriosclerosis and right vertebral artery tortuosity.
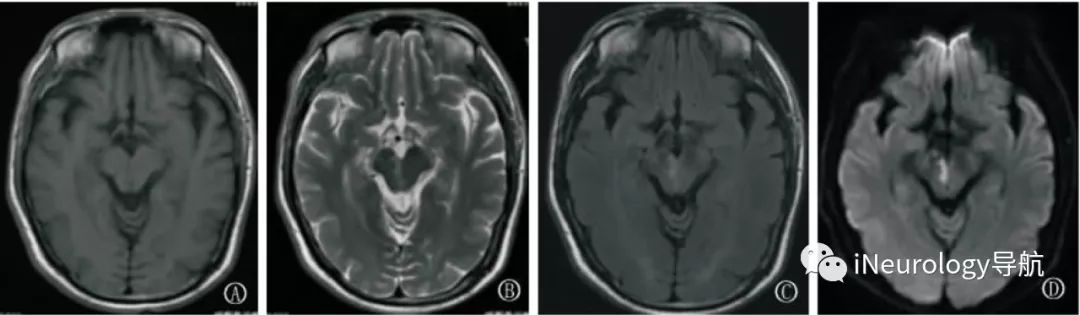
Figure 2:Figures A, B, C show right midbrain medial long T1 and high T2 FLAIR abnormal signals, Figure D DWI shows high signals in the right midbrain medial, head MRI + DWI on the ninth day of illness.

The red nucleus is part of the midbrain, closely connected with the cerebellar nuclei, cerebral cortex, globus pallidus, midbrain tectum, substantia nigra, and the external reticular nucleus of the inferior olive. Its function is mainly to assist voluntary movement through the cortical red nucleus pathway and the cerebellar red nucleus spinal cord pathway.
The nucleus of the oculomotor nerve (III cranial nerve) is located in the midbrain superior colliculus and the ventral gray matter of the cerebral aqueduct. It sends nerve fibers out through the cerebral peduncle in the oculomotor nerve groove (Figure 3).
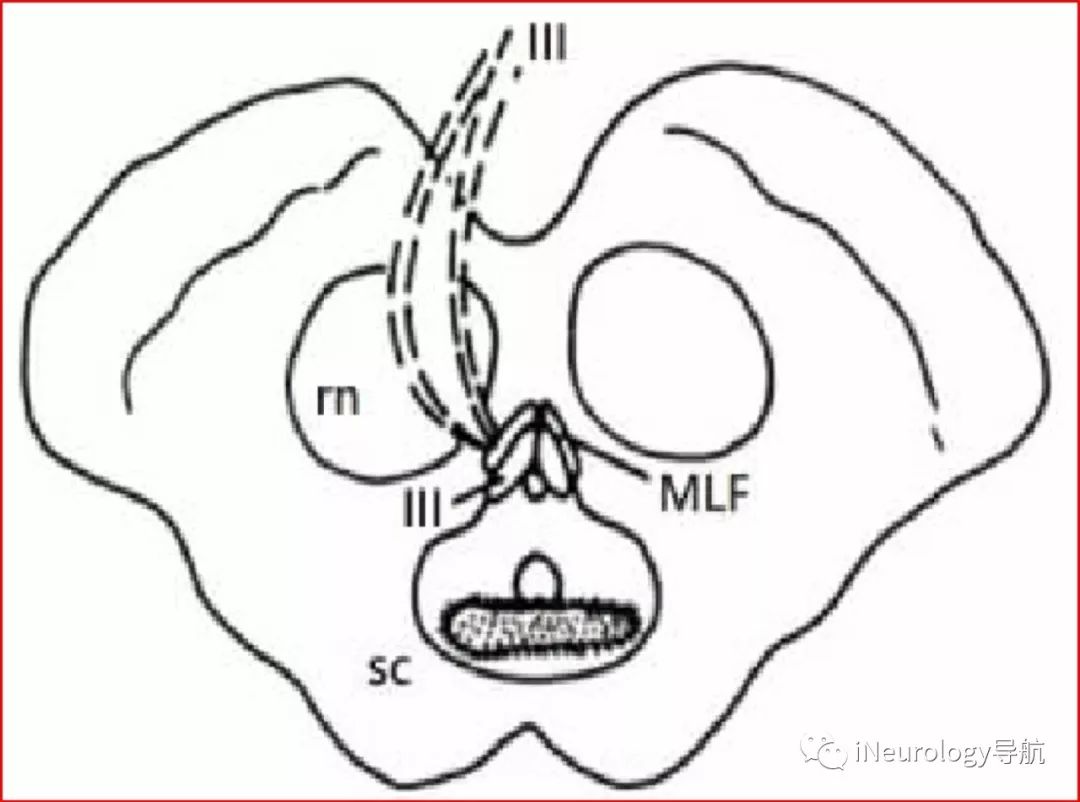
Figure 3: Schematic diagram of the midbrain horizontal section.
(sc superior colliculus, MLF medial longitudinal fasciculus, rn red nucleus, III oculomotor nerve)
When near the cerebral aqueduct in the dorsal part of the midbrain, due to tumors, inflammation, and vascular lesions, the ipsilateral oculomotor nerve and cerebellar superior peduncle efferent fibers are affected, leading to a group of symptoms including ipsilateral oculomotor nerve paralysis and contralateral cerebellar ataxia.
In 1912, French psychiatrist and neurologist Claude first described this group of symptoms. Subsequently, this group of symptoms was named Claude’s syndrome, also known as the lower red nucleus syndrome. This syndrome is relatively rare, with only a few case reports internationally since its first report.
Previously, Claude’s syndrome was considered a typical manifestation of red nucleus function, but only a few case reports showed that the lesions mainly affected the red nucleus.
Seo et al. performed head MRI examinations on 6 patients with Claude’s syndrome and found that the lesions were mainly located in the cerebellar superior peduncle and the lower medial red nucleus. Pathological examinations of patients with Claude’s syndrome found that it was mainly due to some central midbrain infarction, causing lesions in the cerebellar superior peduncle and lower medial red nucleus.
Therefore, Keane et al. proposed that the main lesions of Claude’s syndrome are located in the cerebellar superior peduncle rather than the red nucleus. Song et al. also proposed the same view.
Clinically, Claude’s syndrome can easily be confused with Benedict’s syndrome (red nucleus syndrome), the latter mainly characterized by ipsilateral oculomotor nerve paralysis and contralateral limb hemiplegia, involuntary movements, tremors, etc. The lesion level is at the level of the midbrain inferior colliculus, caused by damage to the oculomotor nerve and red nucleus, with the oculomotor nerve often exhibiting incomplete paralysis.
Claude’s syndrome involves damage at the level of the midbrain superior colliculus, with only ipsilateral oculomotor nerve damage and contralateral limb ataxia, without contralateral limb motor impairment, which is different from Benedict’s syndrome.
This case involved a middle-aged male with an acute onset, a history of hypertension, and upon admission, high blood sugar was found, meeting the diagnostic criteria for diabetes. The patient had a left central mild facial paralysis, which was not a new finding in this episode, considered due to old infarction in the right pons affecting the corticobulbar tract. MRI indicated abnormal signals in both bridge arms, with infarction in the pons and thalamus, suggesting that the patient had atherosclerosis in the vertebrobasilar artery system, which had already caused ischemic infarction of local brain tissue, and the tortuosity of the vertebral artery might exacerbate ischemic episodes.
The patient initially presented with simple diplopia, considered as incomplete ocular muscle paralysis; on the third day of illness, head MRI + DWI did not show new infarcts, and that night the patient had transient relief of symptoms, indicating a transient ischemic attack of the vertebrobasilar artery system at that time. However, the patient gradually developed right eyelid ptosis, right pupil dilation, right eye in an abducted position, and right eye adduction and upward and downward gaze limitations, indicating signs of right oculomotor nerve paralysis, along with left limb ataxia, positive Romberg’s sign, and inability to tandem walk, indicating damage to the cerebellar connecting fibers; follow-up head MRI + DWI indicated newly developed lesions in the right midbrain medial, clearly localized, combined with the patient’s acute onset, history of TIA, prior hypertension, diabetes, etc., qualifying it as cerebrovascular disease. This is a relatively typical case of Claude’s syndrome..
This case also reminds the author that when patients present with new symptoms and signs, timely re-examination with imaging studies is necessary to provide evidence for clinical diagnosis and treatment.