 Neurology Channel of the Medical Community Author:Chu Zhongren Reporting Expert: He Zhiyi
Neurology Channel of the Medical Community Author:Chu Zhongren Reporting Expert: He Zhiyi
Professor He Zhiyi from the Department of Neurology at the First Hospital of China Medical University shared an exciting lecture on the topic of “Clinical Characteristics of Acute Cerebral Infarction on MRI”. Due to the extensive content, we will split it into several parts for explanation. Let’s start the second part, bring your little stools, and learn together…
Midbrain Infarction – Claude Syndrome
A 61-year-old female patient was admitted with the main complaint of “sudden fall for 3 days, right eyelid droop for 2 days”.
Present Illness: Three days ago, she suddenly fell while playing with her child, with no loss of consciousness, no seizures, and no limb weakness, she stood up by herself. However, she tilted to the left while walking, and cranial CT showed no abnormalities. Two days ago, she developed right eyelid droop, with no diplopia, no eye pain, and no visual impairment.
Medical History: Hypertension for over 20 years. Physical examination: Conscious, right eyelid droop, right eye exotropia, and adduction deficiency, pupils equal and round, light reflex present. Nasolabial folds symmetrical, tongue protrusion midline, limb muscle strength grade V, limb tendon reflexes normal, no pathological signs, left finger-nose test slightly unstable, left alternating movement test clumsy, Romberg sign(+).
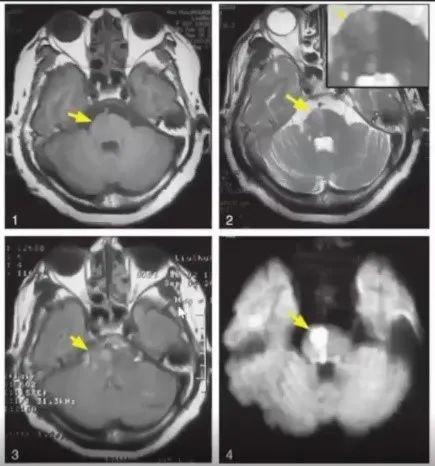
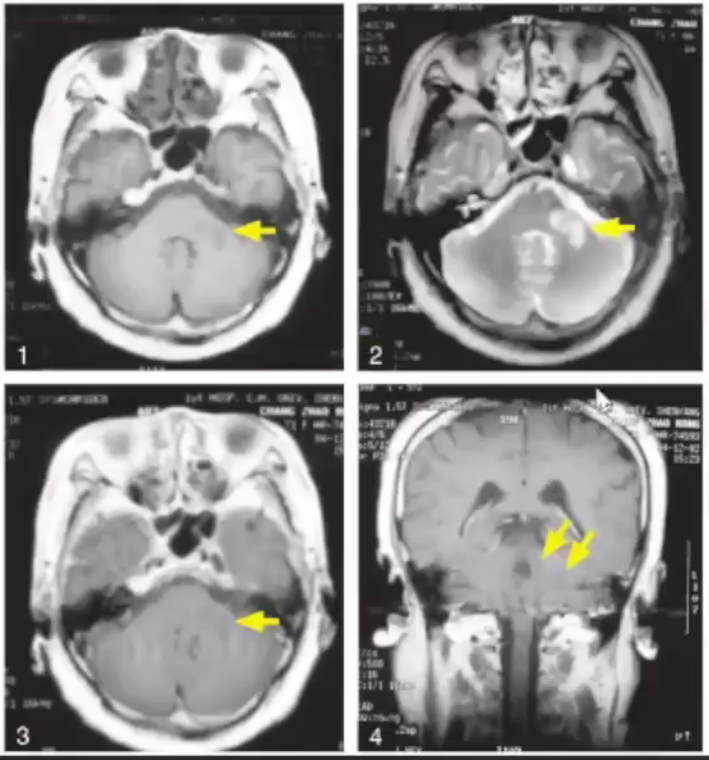
Cranial MRI showed long T1 and long T2 signal in the right midbrain, as indicated by the yellow arrow.
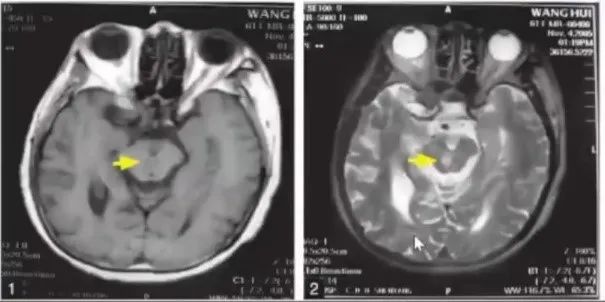
Midbrain Infarction (Claude Syndrome).
Claude Syndrome, also known as lower red nucleus syndrome, was first proposed by French psychiatrist Claude in 1912. Clinical manifestations include diplopia caused by oculomotor nerve paralysis on the same side, eyelid droop, fixed exotropia, and ataxia of the contralateral limbs caused by red nucleus damage, unstable gait, and poor alternating movements. If the lesion is extensive, it can also cause ipsilateral trochlear nerve paralysis, contralateral oculomotor nerve paralysis or sensory disturbances and consciousness disorders, and may develop into medial longitudinal fasciculus syndrome or Parinaud syndrome.
Midbrain Infarction – Wernekink Syndrome
A 59-year-old female patient was admitted with the main complaint of “dizziness and unstable walking for 15 hours”. Fifteen hours before admission, she suddenly experienced dizziness and unstable walking without obvious triggers, with slurred speech, and fell to the sides while walking.
Physical examination: Conscious, speech disorder. Pupils equal and round, diameter = 3.0mm, light reflex sensitive, left eye horizontal nystagmus, palatal myoclonus(-). Bilateral forehead wrinkles and nasolabial folds symmetrical, soft palate and uvula midline, pharyngeal reflex normal, tongue protrusion midline. Neck stiffness negative. Limb muscle strength grade V, BCR (L:++, R:++), PSR (L:++, R:++), Babinski sign (L:-, R:-). No definite abnormalities found in deep and superficial sensation examination, bilateral finger-nose test slightly unstable, bilateral heel-knee-shin test slightly unstable, tandem gait and eyes closed standing test positive. Past medical history: Hypertension for over 10 years.
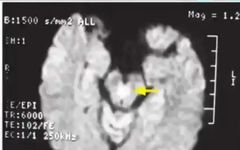
Cranial DWI showed a lesion at the midline of the midbrain, presenting as restricted diffusion high signal.
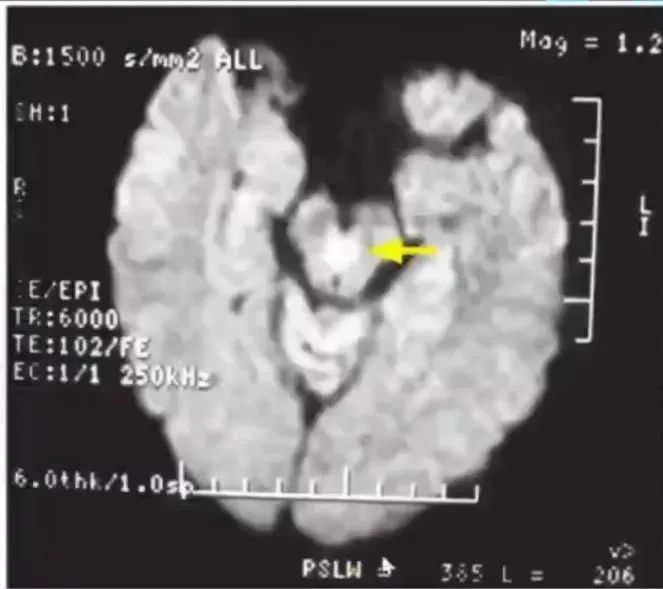
Midbrain Infarction (Wernekink Syndrome).
The midbrain contains numerous nerve fibers connecting to the cerebellum. The fibers originating from the cerebellum cross to the contralateral midbrain red nucleus after relay through the dentate nucleus via the cerebellar peduncle, forming the Wernekink crossing. This area is supplied by the paramedian branch of the basilar artery. When the paramedian branch of the basilar artery is occluded, it can cause damage to the Wernekink connection, known as Wernekink Syndrome. The main manifestations are bilateral cerebellar ataxia, including limb ataxia, trunk ataxia, and ataxic dysarthria, occasionally accompanied by ocular movement disorders and palatal muscle spasms.
Pontine Middle Upper Paramedian Artery Infarction
A 62-year-old female patient was admitted with the main complaint of “dizziness and left limb weakness for 1 day”. One day ago, she suddenly developed dizziness accompanied by double vision, nausea, and vomiting, with weakness in the left limb. Physical examination: Conscious, dysarthria, bilateral horizontal nystagmus, left central facial paralysis, left limb muscle strength grade IV, Babinski sign (L:-, R:-).
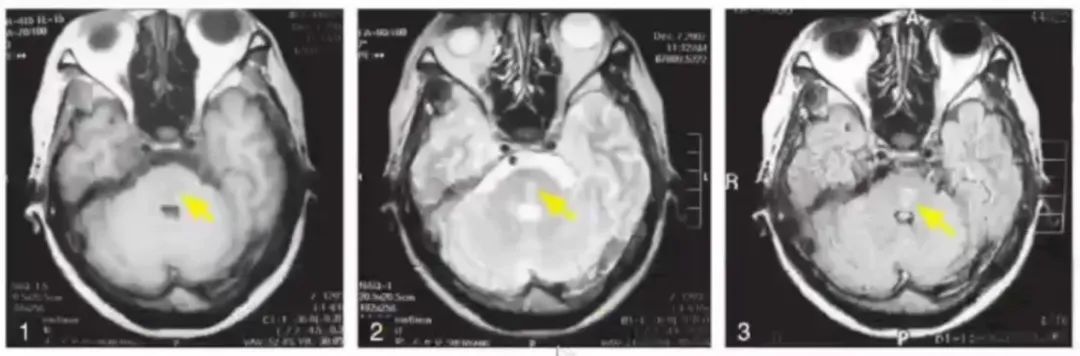
1~4: Cranial MRI showed patchy long T1 and long T2 signals in the right pons, FLAIR sequence showed high signals, DWI showed restricted diffusion high signals (as indicated by the yellow arrow); attention should be paid to distinguishing between the upper and lower parts of the pons.
Pontine middle upper paramedian artery infarction.
Pontine middle upper paramedian artery infarction can cause central facial and tongue paralysis on the opposite side due to the lesion being above the facial nerve nucleus. This disease often presents with numbness, weakness, central facial and tongue paralysis on the lesion side, and unclear speech. Clinically, there are no crossed signs, and it needs to be differentiated from hemiplegia caused by cerebral hemisphere lesions. Cranial MRI, especially DWI examination, is significant for distinguishing between the two.
Pontine Infarction – One and a Half Syndrome
A 49-year-old female patient was admitted with the main complaint of “double vision for 2 days”.
Present Illness: Two days ago in the afternoon, she developed diplopia, accompanied by dizziness, nausea, and vomiting, with no rotational vision or tinnitus, and no coughing while drinking; limb movements were possible.
Medical History: Drug-induced liver cirrhosis for 1 month, hypertension for 6-7 years.
Physical Examination: Clear consciousness, pupils equal and round, light reflex sensitive, left eye adduction and abduction disorders, right eye adduction disorder, horizontal nystagmus during abduction(+), nasolabial folds symmetrical, tongue protrusion midline, no limb paralysis. Neck stiffness negative, BCR (L:++, R:++), PSR (L:++, R:++), Hoffmann sign (L:-, R:-), Babinski sign (L:-, R:-).
Cranial MRI showed long T1 and long T2 lesions in the left lower pontine tegmentum, FLAIR showed high signals (as indicated by the yellow arrow).
Pontine Infarction (One and a Half Syndrome).
One and a Half Syndrome was proposed by Fisher in 1967, caused by lesions in the pontine tegmentum damaging the parapontine reticular formation (PPRF) and the medial longitudinal fasciculus (MLF). Lesions in one side of the pontine tegmentum can affect both the pontine gaze center and the contralateral crossed connections to the oculomotor nerve nucleus of the medial longitudinal fasciculus, resulting in the inability to adduct or abduct the affected eye during horizontal gaze, while the contralateral eye can abduct but presents with horizontal nystagmus. Common causes of One and a Half Syndrome include stroke, multiple sclerosis, and less common cases like tuberculoma, brainstem tumors, and giant cell arteritis.
Infarction in the Posterior Inferior Cerebellar Artery Supply Area
A 72-year-old male patient was admitted with the main complaint of “sudden dizziness accompanied by nausea, vomiting, and rotational vision for 1 day”. One day ago, he suddenly developed dizziness with no obvious trigger, accompanied by nausea and vomiting, with vomit being gastric contents and rotational vision. Physical examination: Clear consciousness, slow speech, horizontal nystagmus, no facial or tongue paralysis, limb muscle strength basically normal, left limb ataxia and intention tremor. Cranial DWI, MRI showed infarction in the left cerebellar hemisphere. After treatment of antiplatelet, lipid-lowering, and plaque stabilization, the patient’s symptoms gradually improved, and he was discharged without significant sequelae.
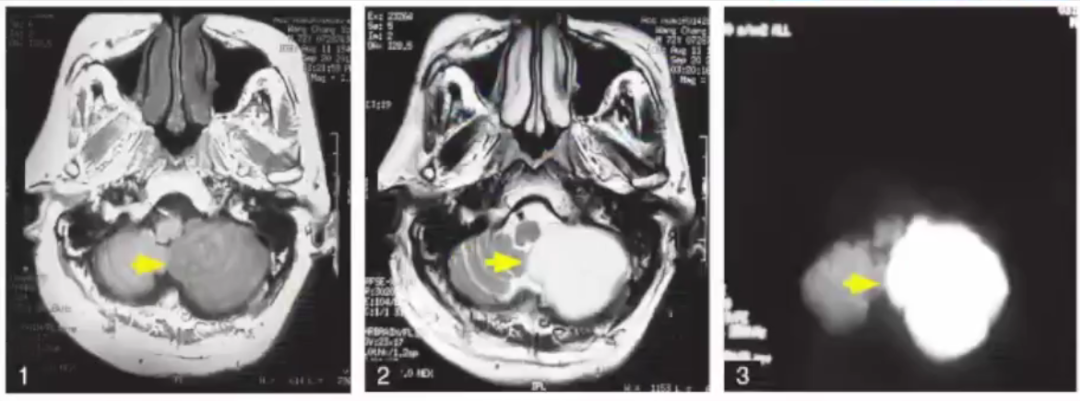
1,2: Cranial MRI showed large areas of long T1 and long T2 signals in the left cerebellar hemisphere. 3: Cranial DWI showed large areas of restricted diffusion high signals. The lesion area is indicated by the yellow arrow.
Cerebellar Infarction (Infarction in the Posterior Inferior Cerebellar Artery Supply Area).
A 59-year-old male patient was admitted with the main complaint of “headache, nausea, and dizziness for 3 days”. Present illness: The patient developed a headache 3 days ago, with a feeling of pressure on the right side of the head, accompanied by nausea without vomiting, and dizziness that relieved after 10 minutes. The next afternoon, the headache recurred and relieved after 10 minutes. This morning at 4 a.m., the above symptoms recurred and progressively worsened, with coughing while drinking, numbness on the right side of the face, and hoarseness. Past medical history: Hypertension for 30 years, diabetes for 4 years, myocardial ischemia for 3 years, and suffered from cerebral infarction in 2001, leaving unclear speech. Physical examination: Clear consciousness, dysarthria, mild hoarseness, right eyelid droop, unequal pupils, left diameter ≈ 3.0mm, right diameter ≈ 2.0mm, light reflex sensitive, shallow nasolabial fold on the right side, limb muscle strength grade IV, Babinski sign (L:-, R:-).
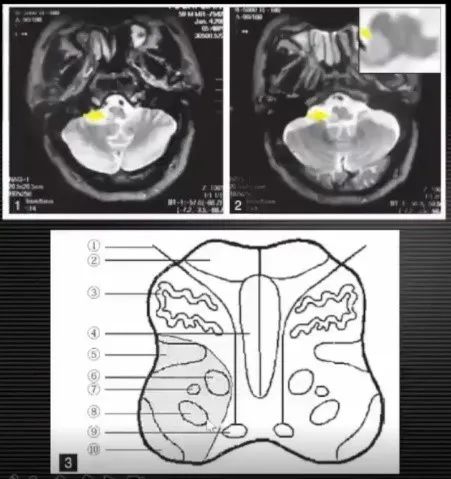
1,2: Cranial MRI showed long T2 signals in the lateral medulla (as indicated by the yellow arrow). 3: Schematic diagram of Wallenberg Syndrome, with the shaded area indicating the infarct area. ① Hypoglossal nerve; ② Pyramidal tract; ③ Inferior olive; ④ Medial lemniscus; ⑤ Spinothalamic tract; ⑥ Nucleus of the ambiguous; ⑦ Sympathetic fibers; ⑧ Trigeminal spinal tract and nucleus; ⑨ Hypoglossal nucleus; ⑩ Cerebellar peduncle (spinal cerebellar posterior tract).
Medullary Infarction (Wallenberg Syndrome).
The posterior inferior cerebellar artery supply area mainly includes the dorsal internal area of the cerebellum, the lateral medulla, and the anterior external area of the cerebellum, which can present with symptoms such as dizziness, ataxia, and nystagmus. Involvement of the medulla can present complete or incomplete Wallenberg syndrome. Clinically, when encountering patients with dizziness, this disease should be considered, and when encountering patients with Wallenberg syndrome, attention should be paid to determine whether the cerebellum is involved. Typical clinical diagnosis of Wallenberg syndrome is relatively easy, but due to anatomical variations of blood vessels and differences in lesion size, atypical Wallenberg syndrome can have complex clinical manifestations, leading to misdiagnosis and missed diagnosis. Detailed inquiry of medical history and careful physical examination can reduce the rate of misdiagnosis or missed diagnosis, and early cranial MRI examination is beneficial for early detection of lesions.
Infarction in the Anterior Inferior Cerebellar Artery Supply Area
A 71-year-old female patient was admitted with the main complaint of “dizziness, head pressure for 4 days, and left facial numbness for 23 hours”. Present illness: Four days ago, she woke up with dizziness and head pressure without any trigger, at which time her blood pressure was measured at 180/100mmHg. After taking antihypertensive medication, there was no significant improvement in symptoms; that night, dizziness and head pressure worsened, accompanied by tinnitus and diplopia, and the above symptoms worsened with activity or turning her head, slightly relieved by resting in bed, vomiting twice with gastric contents; 23 hours ago, the patient developed left facial numbness. There was no loss of consciousness, no coughing while drinking, and no swallowing difficulties; eating, sleeping, and bowel movements were normal. Positive neurological signs; bilateral horizontal nystagmus(+), left facial pain sensation decreased, left alternating movement was clumsy, left heel-knee-shin test was slightly unstable, limb tendon reflexes were weakened, Babinski sign (L:-, R:-).
1,2: Cranial MRI showed patchy long T1 and long T2 signals in the left pontine arm. 3,4: No enhancement effect after enhancement.
Cerebellar Infarction (Pontine Infarction).
A 61-year-old male patient was admitted with the main complaint of “dizziness for 7 days”. The patient felt dizzy after exertion 7 days ago, accompanied by unclear speech and frequent nausea and vomiting, with no tinnitus or hearing loss. Past medical history: Hypertension for 40 years, coronary heart disease, atrial fibrillation for 20 years. Family history: Both parents had hypertension.
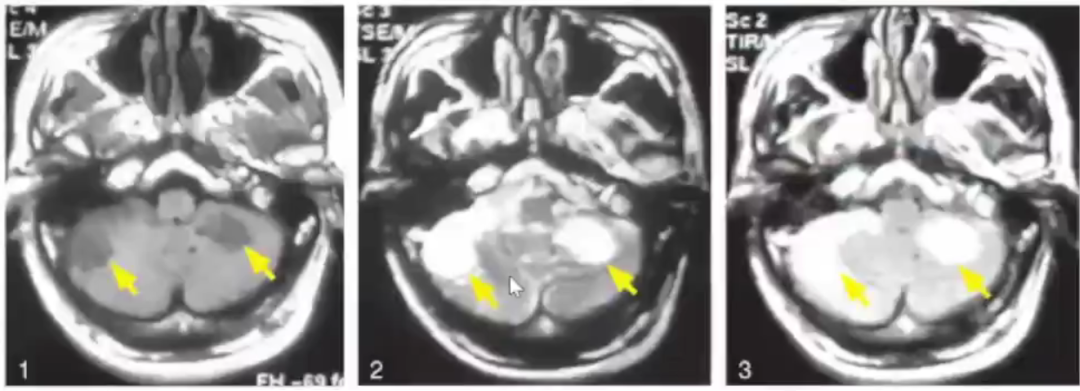
Cranial MRI showed long T1 and long T2 signals in both anterior inferior cerebellar arteries, with high signals in FLAIR (as indicated by the yellow arrow).
Bilateral Infarction in the Anterior Inferior Cerebellar Artery Supply Area.
A 75-year-old female patient was admitted with the main complaint of “dizziness for half a year, worsening with right limb weakness for half a month”. The patient developed dizziness without obvious trigger half a year ago, which was heavier when getting up, relieved in the supine position, but did not improve with systematic diagnosis and treatment. In the past half month, the dizziness symptoms worsened, occasionally accompanied by diplopia, slurred speech, and tinnitus, with no nausea or vomiting. Physical examination: Clear consciousness, cooperative during the examination. Slurred speech, pupils equal and round, diameter about 2.5mm, light reflex sensitive. Bilateral eye movements in all directions were sufficient, obvious horizontal nystagmus. Bilateral forehead wrinkles and nasolabial folds symmetrical, soft palate and uvula midline, pharyngeal reflex normal, tongue protrusion midline. Neck stiffness negative. Left limb muscle strength grade V, right limb muscle strength grade IV, limb muscle tone normal, limb tendon reflexes normal, Babinski sign (L:-, R:-).
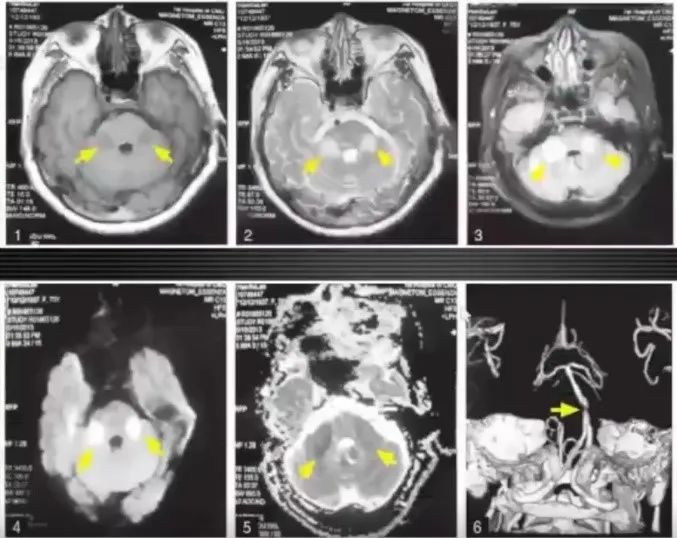
1-3: Cranial MRI showed isolated long T1 and long T2 lesions in both pontine arms, FLAIR showed high signals (as indicated by the yellow arrow). 4, 5: DWI showed high signals and ADC showed low signals. 6: CT angiography of the head and neck showed near-complete occlusion of the basilar artery.
Bilateral Infarction in the Anterior Inferior Cerebellar Artery Supply Area (Isolated Bilateral Pontine Infarction).
The clinical features of infarction in the anterior inferior cerebellar artery supply area include not only cerebellar ataxia, peripheral facial paralysis, and facial pain, temperature sensation disorders, but also can cause hearing loss and tinnitus on the lesion side, sometimes easily confused with ear diseases. The most important diagnostic tool is cranial MRI examination. If unilateral (or bilateral) pontine and/or anterior inferior cerebellar hemisphere infarction occurs, this disease should be considered, but this area can also have demyelinating lesions or malignant tumor occupancy changes, and cranial enhanced MRI should be performed for differentiation.
If you found this helpful, please click “Looking” in the lower right corner, thank you!
Follow me, don’t get lost, learn a little bit every day
Basic Memory of Brainstem Syndromes [Easy to Remember Version]
[Recommended] Neurological Imaging Video Course, 31 Chapters in Total!
Brainstem Physiology, Anatomy, and Lesion Localization [One Copy per Person]
Evolution of Signals in Intracranial Hemorrhage, you won’t forget after watching, if you forget, come find me!
Learning Anatomy One Cut at a Time, In-Depth Analysis!
Analysis and Diagnostic Thinking of High Signal Lesions in T1WI in the Brain [From Pathogenesis to Imaging]
Characteristic Abnormal Brain Imaging Collection – MRI Edition
Chinese Guidelines for the Diagnosis and Treatment of Myasthenia Gravis (2020 Edition)
Illustrated Explanation of Thalamic Infarction
Evolution of MR Signals in Intracerebral Hemorrhage and Molecular Mechanisms, this is the essence of understanding!
Wang Yongjun | Selection of Suitable Populations for Venous Thrombolysis in Ischemic Stroke (2021)
Learning Neuroanatomy Stroke by Stroke [Continuation 9 Episodes Completed]
Learning Neuroanatomy Stroke by Stroke [Six Lectures. All]
Definition, Imaging Performance, Principles, and Clinical Application of FLAIR Vascular High Signal Sign!
CT Imaging of Intracranial Anatomy
[Quality Lectures] Neurology Video Lectures, 10 Episodes in Total!
Interpretation of ESO Guidelines for Venous Thrombolysis in Acute Ischemic Stroke
Specific Imaging Signs of Intracranial Diseases on CT
Thesis | Analysis of Causes of Diplopia (“MIDNIGHTS” Principle)
Guidelines for Diagnosis and Treatment of Dizziness in Emergency (2021)
Jiang Guihua: Looking at Diseases from Images in Intracranial Tumors [Replay]
[Quality Recommendation] Clinical “Genius” for Reading Cranial MR Images
The Most Detailed Brain Sulci and Gyri Marking Atlas So Far
Comprehensive Summary of Knowledge Points Related to Cerebrovascular Diseases
[Quality] Detailed Explanation of the Ten Brainstem Anatomical Levels and Functions!
Neuroanatomy: Lesion Presentation and Localization Diagnosis [Local In-Depth Explanation]
Classic Knowledge Points of the Nervous System – Illustrated
Classic Analysis: Differences Between Low Back Pain, Referred Pain, Radicular Pain, and Nerve Root Disease
[Cerebrovascular Special Topic] Application Anatomy of Cerebrovascular
Easy Misdiagnosis Imaging Series for Head MRI Entry (Complete)
[T2WI Inversion Imaging + Specimen] High-Definition Cranial Section Anatomy
[One Copy per Person] The Most Detailed High-Definition Cranial MR Anatomy
Clearly Understanding Brain Sulci and Gyri, Simple Functional Anatomy!
[Thalamic Special Topic]: Functional Anatomy of the Internal Capsule, Master This Chart, No Worries About the Internal Capsule!
[Cerebrovascular Disease Imaging Special Topic] Common MRI Performances of Cerebrovascular Diseases
Basic Neuroscience – Localization and Qualitative Analysis
[Must Read] These Cranial MR Easily Missed Diagnoses Have Been Summarized!
Learning Brain White Matter Fiber Anatomy, Now It’s Clear
Localization Diagnosis of Neurological Diseases
Anatomical Imaging of the Cerebrovascular System: 3D Mode Presentation
[Recommended] High-Definition Brain Section Anatomy, Step by Step Features of the Brainstem and Nuclei
[Collection] The Most Comprehensive CT Section Anatomy Atlas
Common Cerebrovascular Lesions on CTA, This PPT is Enough
High-Definition Detailed Diagram of the Brain Pool Above and Below the Curtain
Neuroanatomy – High-Definition Atlas of the Brain
Illustrative Diagram of Blood Supply of Important Nerve Structures
[Recommended] Qualitative Diagnosis and Imaging Features of Pontine Lesions
Pathological Basis, Clinical, and Imaging Manifestations of Various Cerebrovascular Malformations [Summary Collection]
[Quality] Analysis of MRI Features of Demyelinating Diseases and Differential Diagnosis
Localization Diagnosis of Neurological Diseases
[Deep Learning] High-Definition Anatomy of the Head and Neck Arterial System
[Teaching Video of Clinical Stroke Assessment Scale] NIHSS Scoring Video Teaching First Prize Work
Professor Rao Zhiren | Localization Diagnosis of Neurological Diseases
These Common Cerebrovascular Diseases Imaging Diagnoses Need to Be Mastered!
Remember These Typical Distribution Areas, Pay Attention to Details in Diagnosing [Cerebral Infarction]
The Most Comprehensive Imaging Diagnosis and Differential Diagnosis of Bilateral Basal Ganglia Lesions [Most Comprehensive]
How to Diagnose Cerebral Infarction Without MRI in the Very Early Stage Using CT
Involuntary Movements of the Head and Face [You Will Definitely Encounter in Outpatient Clinics]
Expert Consensus on Diagnosis and Treatment of Intracranial Cavernous Hemangiomas – Summary of Key Points
Intracranial DWI High Signal Disease Presentation – From Understanding the Disease to Specific Diagnosis
Those Things About Hoffmann’s Sign
Common Nerve Root Innervation Areas – This Article Clarifies the Muscle Segments and Skin Segments
Should Antiplatelet Treatment Be Restarted After Intracerebral Hemorrhage, and When is the Best Time to Restart?
Persistent Dizziness – Brainstem and Cerebellar Lesions
In-Depth Analysis – Hand-Related Infarction
Cerebrovascular | When Anatomy Meets Clinic!
Summary of Cerebrovascular Anatomy Learning
Hematoma Staging | Just Remember This Gesture!
Lumbar Disc Herniation, This is the Best Article I’ve Read!
Vestibular Nervous System Anatomy and Physiology
Techniques for Applying Mannitol in Acute Cerebrovascular Disease Treatment
[Quality Chinese Version] Imaging Differential Diagnosis of Stroke (Complete Collection)
Ultra High Definition Cranial 7T-MRI Three-Dimensional Dynamic Imaging (Can Be Used as Teaching Material)
Diplopia | From Anatomy to Clinic
Collection of Classic Version | MRI Manifestations of Toxic Metabolic Encephalopathy
Clinical Super Practical | Step-by-Step Teaching of Diagnosis and Treatment of Benign Paroxysmal Positional Vertigo (BPPV)
[Updated Version] Inferring Responsible Vessels from Infarct Locations
The “Eccentric Target Sign” That We Keep Mentioning, Turns Out to Be This Disease!
One Document to Determine the Landscape | Basic Anatomy of Cerebrovascular
[Classic] Interpretation of Cerebrovascular Diseases Based on Vascular Anatomy
Illustration of Mechanism of Pontine Infarction and Lenticulostriate Artery Infarction | Anatomy and Diagram
Brief Thoughts on Neurological Examination
Classic PPT | MRI Manifestations of Autoimmune, Toxic, and Metabolic Encephalopathy
Follow the public account, let us know what content you are interested in, leave a message
Reprint, Submission, Business Cooperation: zmh17337166505 (WeChat)