
What does the α-glucosidase inhibitor look like in your eyes?
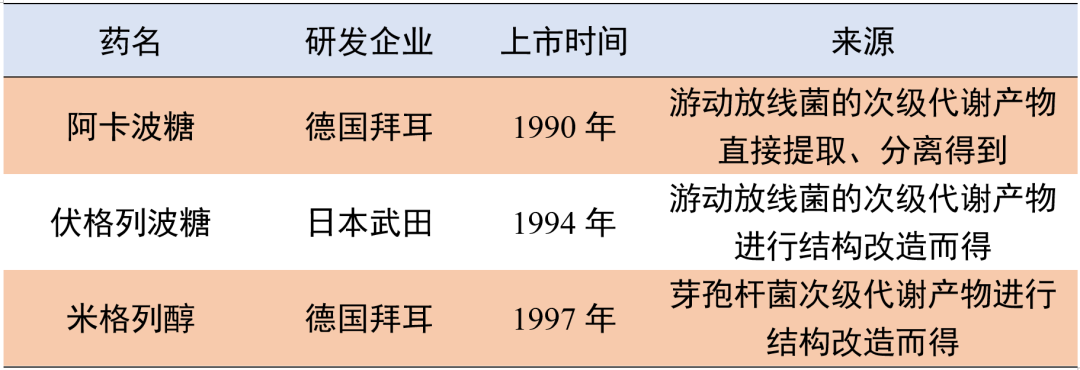
Members of the Alpha-Glucosidase Inhibitor Family[1]
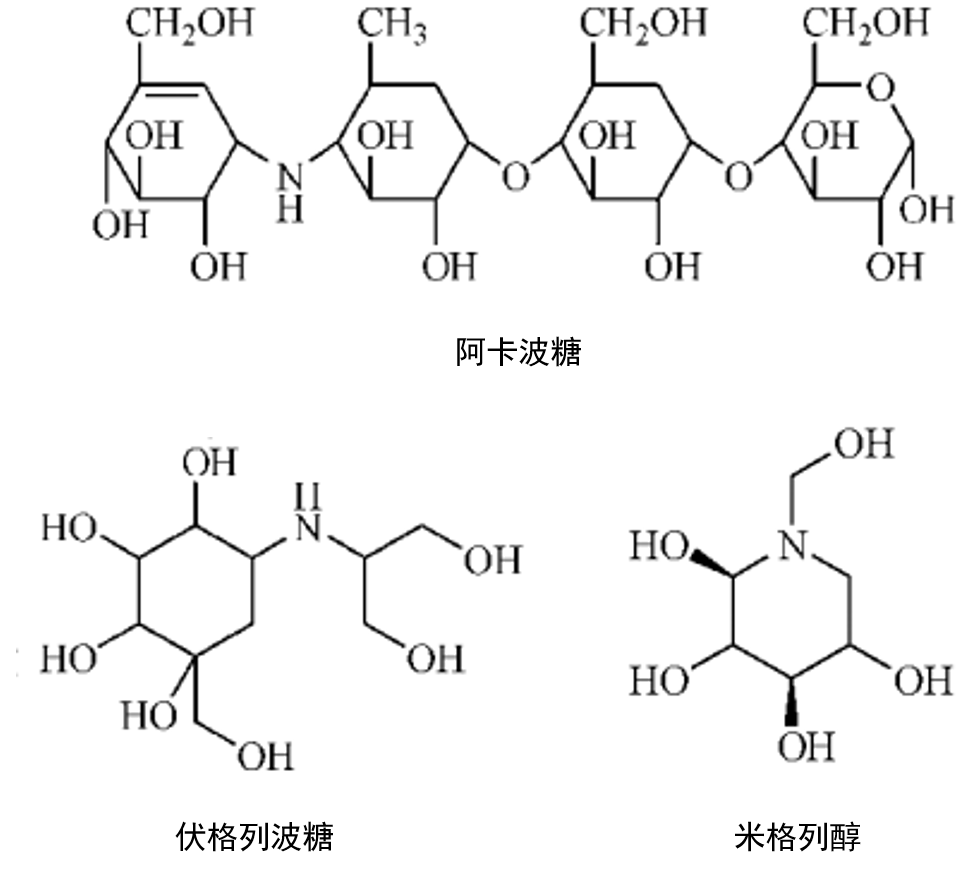
Common AGIs include Acarbose, Voglibose, and Miglitol. Let’s start by understanding their chemical structures:
Table 1 Comparison of the Three Drugs
Carbohydrates are the main source of energy for the human body. The sugars in food include polysaccharides (starch), disaccharides (such as maltose, sucrose, etc.), and monosaccharides (such as glucose, fructose, and galactose). Except for monosaccharides, which can be directly absorbed into the bloodstream by intestinal epithelial cells, others must be hydrolyzed by α-glucosidase into monosaccharides for utilization. This means that if the activity of α-glucosidase is inhibited, the absorption of sugars can be reduced.
AGIs utilize their structural similarity to these oligosaccharides, binding to the binding sites of α-glucosidase, thereby reversibly inhibiting or competitively inhibiting α-glucosidase, reducing the breakdown of oligosaccharides into monosaccharides, thus delaying the intestinal absorption of monosaccharides, especially glucose[2], resulting in lower and flatter postprandial blood glucose peaks and significantly reduced glycosylated hemoglobin (HbA1c). For example, Acarbose is a biosynthetic pseudotetrasaccharide whose chemical structure is similar to four glucose molecules combined to form an oligosaccharide.
▎Note: α-Glucosidase is not a single enzyme but a collective term for a class of enzymes composed of α-amylase and maltase, isomaltase, α-dextrinase, sucrase, and lactase found on the brush border of small intestinal epithelial cells[3].
Table 2 Comparison of the Enzyme Inhibition Profiles of the Three Drugs
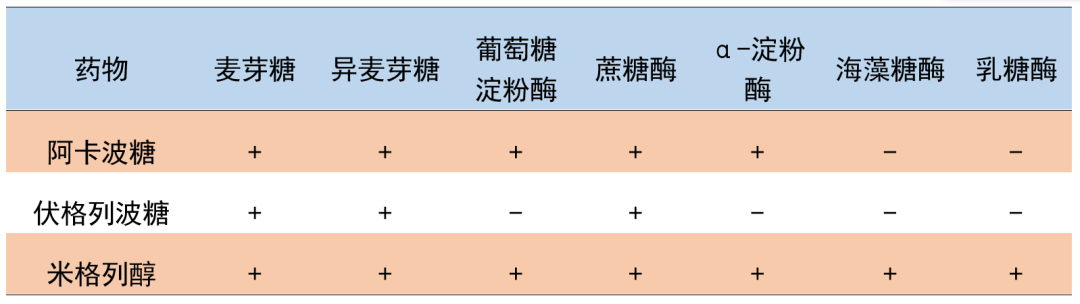
Acarbose primarily inhibits sucrase, glucoamylase, and pancreatic α-amylase.
Voglibose mainly inhibits sucrase and maltase, with much higher inhibitory activity for these two enzymes compared to Acarbose. Since it does not affect amylase, the starch in food is converted into disaccharides in the small intestine, resulting in less starch entering the large intestine, thus gastrointestinal reactions such as bloating and increased gas production are less common[5].
Miglitol has inhibitory effects on various α-glucosidases, with the highest inhibition rates against sucrase and glucoamylase, possibly due to its closer structural similarity to glucose, making it easier to approach the enzyme’s active site[6-8].
There are significant differences in individual pharmacokinetic parameters
Table 3 Comparison of the Pharmacokinetics of the Three Drugs
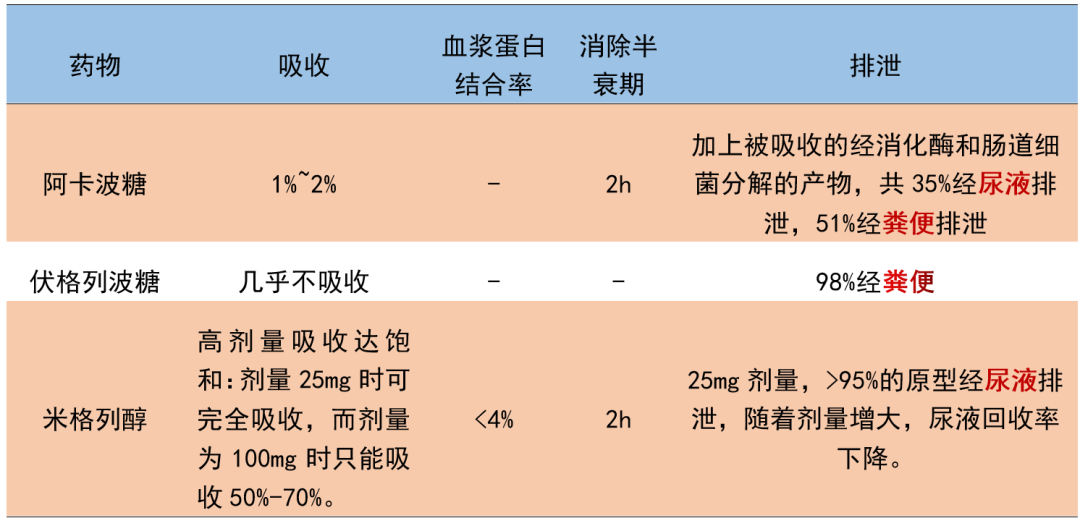
Note: 1. “-” indicates data is not available. 2. Data is referenced from the respective drug instructions.
The main difference is that Acarbose and Voglibose have very little absorption of the parent drug, while Miglitol is nearly completely absorbed at low doses, leading to the differences in excretion shown in the table above.
There are differences in dosage and administration
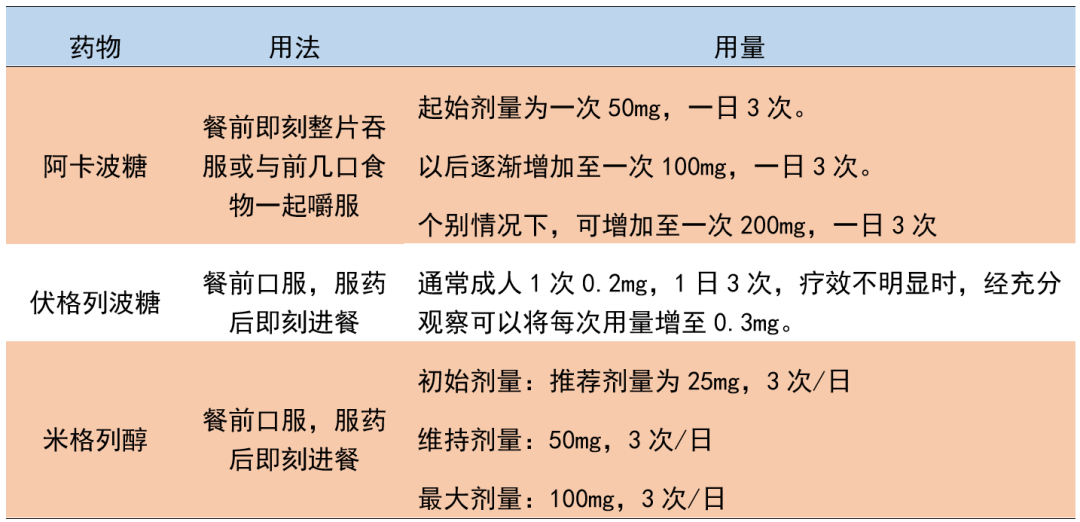
Table 4 Comparison of the Dosage and Administration of the Three Drugs
Comparison of Hypoglycemic Differences
Due to the lack of direct clinical studies comparing different AGI drugs, indirect analysis methods are used to evaluate hypoglycemic differences, which inevitably have certain issues, such as significant differences in baseline characteristics among patients, non-uniform research methods, and low research quality. It is difficult to draw reliable comparisons. Some literature indicates that compared to placebo, the efficiency of reducing HbA1c levels is in the order of Acarbose (0.77%) > Miglitol (0.68%) > Voglibose (0.47%)[9]. However, overall, α-glucosidase inhibitors can effectively lower the HbA1c levels and postprandial blood glucose (2h-PPG) levels in patients with type 2 diabetes[10].
Miglitol shows advantages in reducing postprandial glucose absorption, possibly because Miglitol’s structure is similar to glucose, allowing it to compete for absorption through the same intestinal epithelial transport system[11], whereas Acarbose and Voglibose are absorbed very little.
Patient Medication Precautions
Due to pharmacokinetic differences among the three drugs, the suitable populations also differ, and the following precautions should be noted.
Table 5 Precautions for the Three Drugs
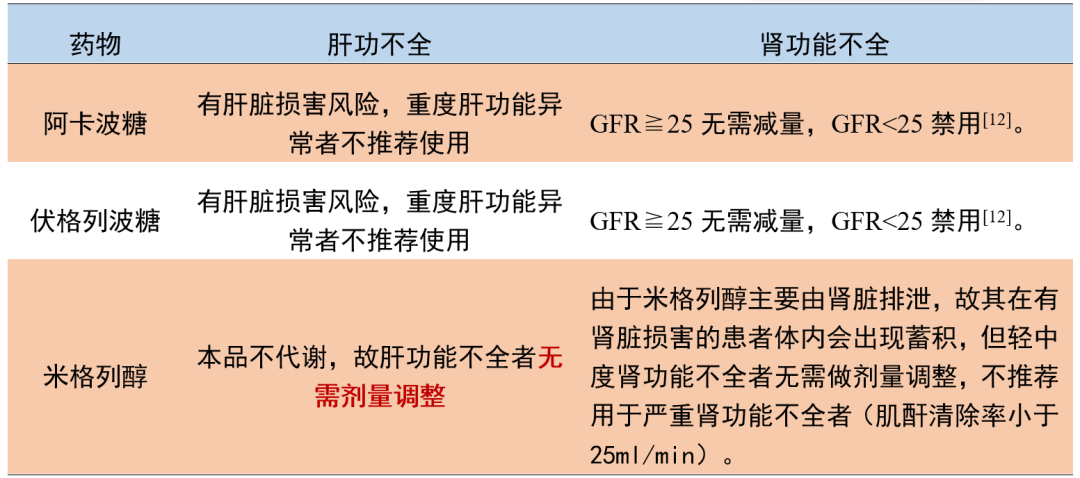
Note: Since Miglitol acts locally, adjusting the dose to correct elevated blood drug concentrations due to excretion disorders is not feasible.
Most Common Adverse Reactions
Gastrointestinal reactions are determined by the pharmacological properties of the drug itself. Theoretically, if the drug acts appropriately, oligosaccharides should be completely digested and absorbed before reaching the end of the ileum; however, in reality, undigested oligosaccharides and starches are broken down by enzymes in the colon, producing acetic acid, lactic acid, and other organic acids, leading to a decrease in intestinal pH and an increase in osmotic pressure, causing diarrhea; the CO2 and H2 produced may cause bloating[3].
Therefore, it is recommended to start with a small dose, as most patients will gradually adapt after 2 weeks of medication.
Comparison of Special Precautions for AGIs
Table 6 Contraindications for the Three Drugs
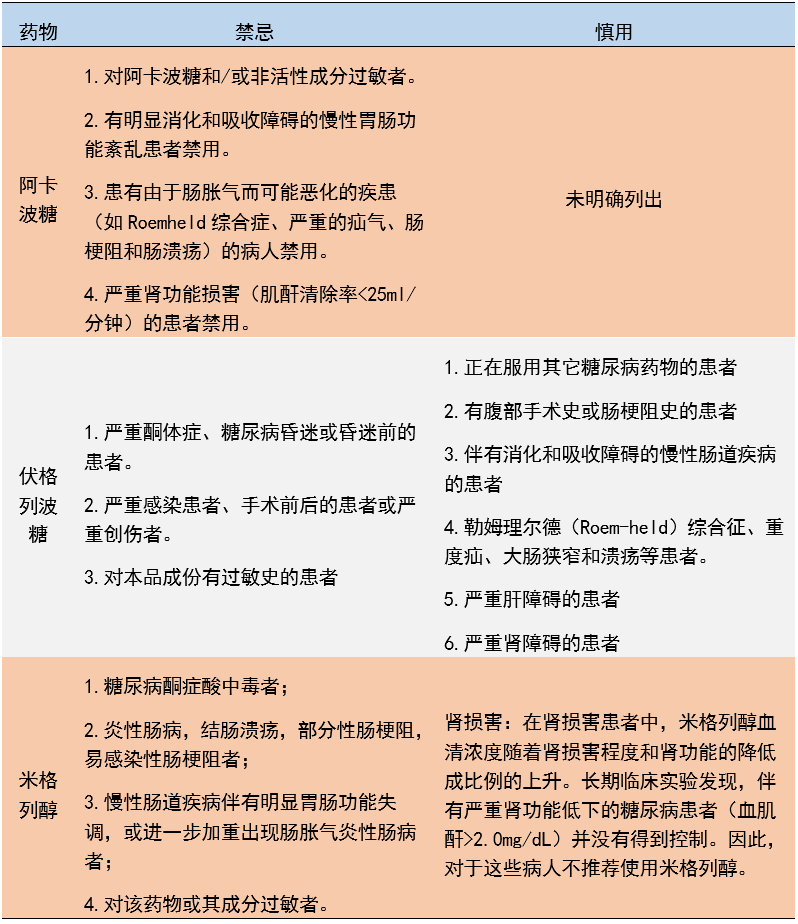
Note: The contraindications for the three AGIs are basically consistent, except that Voglibose reduces the contraindications for patients with gastrointestinal diseases or histories from the other two drugs to “use with caution”, possibly because Voglibose has milder gastrointestinal adverse reactions.
Overall, the main theoretical difference among the three AGIs is their different enzyme inhibition profiles; in clinical applications, Voglibose has milder gastrointestinal reactions and can be chosen when Acarbose or Miglitol cause gastrointestinal intolerance; Miglitol does not cause liver damage, and no dose adjustment is needed in cases of liver dysfunction. However, all can effectively lower HbA1c levels and postprandial blood glucose (2h-PPG) levels in patients with type 2 diabetes, and have good safety profiles.
References:
First published in the Endocrinology Channel of the Medical Community
Author of this article: Yuan Shijia
Reviewed by: Attending Physician Xu Naijia
Editor: Amelia
Previous Excellent Articles
Dietary Guidelines for Gout Patients – Please Check!
Allopurinol Can Lower Uric Acid, But Does Not Protect the Kidneys? | Weekly News
“Transforming” Hyperthyroidism – Beware of Its “Face-Changing” Effects! | Internal Medicine Insights
Welcome Submissions to the Editor’s Email:
Please indicate: [Submission] Hospital Department Name
Generous remuneration for submissions, submit quickly!
Submissions must be original; others will not be considered