In 2021, the European Society of Intensive Care Medicine (ESICM) Abdominal Working Group issued recommendations for gastrointestinal dysfunction in critically ill patients. The concept of acute gastrointestinal injury (AGI) was introduced, along with a recommendation for a graded approach to the management of AGI.
1. Definition
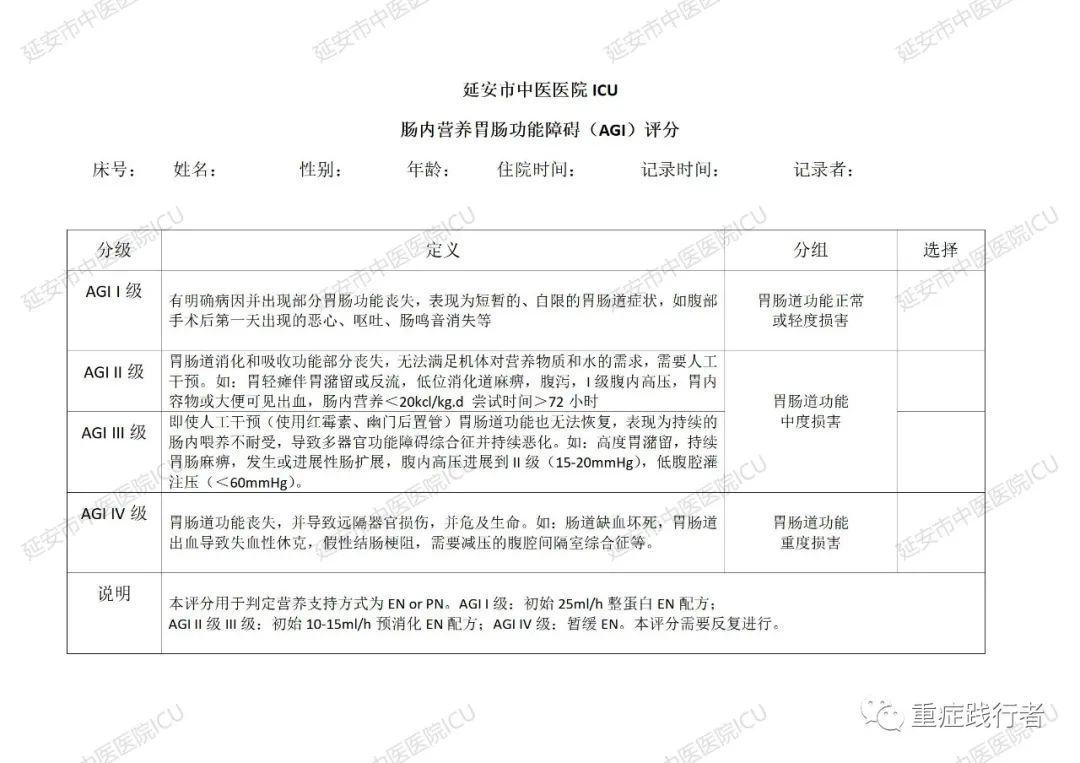
AGI refers to acute gastrointestinal dysfunction caused by the critical illness itself. It is classified into four grades based on the severity of the condition, incorporating intra-abdominal hypertension into the grading criteria.
2. Etiology
AGI is divided into primary AGI and secondary AGI. Primary AGI is caused by underlying gastrointestinal diseases and is commonly seen in the early stages of gastrointestinal injury, such as in cases of peritonitis, pancreatic or liver diseases, abdominal surgery, or abdominal trauma. Secondary AGI results from the body’s response to critical illness without any primary gastrointestinal disease.
3. Related Concepts
All standards are for adults.
1. Feeding Intolerance Syndrome (feeding intolerance syndrome, FI): This refers to enteral nutrition intolerance caused by any clinical reason (such as vomiting, diarrhea, gastrointestinal bleeding, enteric fistula, etc.). If attempts for 72 h fail to achieve a target of 20 kcal/(kg·d) via enteral route, or enteral nutrition is stopped for any clinical reason, FI should be considered.
2. Gastric Retention: A single gastric fluid aspiration exceeding 200 ml is defined as significant gastric retention.
3. Lower Gastrointestinal Paralysis (Paralytic Ileus): Refers to impaired intestinal motility leading to inability to expel feces. No bowel movement for at least 3 d, with bowel sounds present or absent, and excluding mechanical obstruction.
4. Intestinal Dilation: Abdominal X-ray or CT shows colonic diameter exceeding 6 cm (cecal diameter exceeding 9 cm) or small intestinal diameter exceeding 3 cm.
5. Intra-abdominal Hypertension (intra-abdominal hypertension, IAH): This refers to an average intra-abdominal pressure (IAP) of at least 12 mmHg recorded at least twice within 6 h or at least four times in one day.
6. Abdominal Compartment Syndrome (ACS): This refers to sustained elevated intra-abdominal pressure, with at least two measurements of IAP exceeding 20 mmHg within 6 h, accompanied by new organ dysfunction.
4. Grading and Management
(1) AGI Grade I (Risk factors for gastrointestinal dysfunction and failure present)
Clear etiology, partial gastrointestinal function impairment. Characterized by temporary and self-limiting features. Commonly seen in postoperative nausea and vomiting and absent bowel sounds after abdominal surgery; decreased intestinal motility in early shock.
Treatment principles: (1) General condition will gradually improve; adequate intravenous fluids are given, and generally, no special interventions for gastrointestinal symptoms are needed. (2) Early enteral nutrition should be provided as soon as possible within 24~48 h after injury (evidence level 1B). (3) Minimize the use of medications that impair gastrointestinal motility, such as catecholamines and opioids (evidence level 1C).
(2) AGI Grade II (Gastrointestinal dysfunction)
Dysfunction of digestion and absorption, unable to meet the body’s needs for nutrients and water, but has not yet affected the patient’s overall condition. Characterized by acute gastrointestinal symptoms requiring certain interventions to meet the body’s needs for nutrition and water. Clinical manifestations: gastroparesis with significant gastric retention or reflux, lower gastrointestinal paralysis, diarrhea, IAH Grade I (IAP 12~15 mmHg), visible bleeding in gastric contents or feces, food intolerance.
Treatment principles: Implement certain therapeutic measures to prevent progression to gastrointestinal failure. Including: (1) Treat IAH (evidence level 1D); (2) Restore gastrointestinal motility, use prokinetic agents (evidence level 1C); (3) Provide enteral nutrition; if significant gastric retention or reflux is present, attempt small amounts of enteral nutrition (evidence level 2D); (4) If prokinetic agents are ineffective in patients with gastroparesis, consider post-pyloric feeding (evidence level 2D).
(3) AGI Grade III (Gastrointestinal failure)
Loss of gastrointestinal function, and gastrointestinal function does not recover despite intervention; overall condition does not improve, such as persistent food intolerance after aggressive treatment (erythromycin, placement of post-pyloric tubes, etc.), and multi-organ dysfunction continues to exist or worsen. Clinically, it may present as significant gastric retention, persistent gastrointestinal paralysis, intestinal dilation, and intra-abdominal hypertension progressing to Grade II (IAP 16~20 mmHg), and decreased intra-abdominal perfusion pressure (<60 mmHg).
Treatment principles: (1) Monitor and manage IAH (evidence level 1D); (2) Exclude other intra-abdominal diseases, such as cholecystitis, peritonitis, and intestinal ischemia. Discontinue medications that can cause gastrointestinal paralysis as soon as possible (evidence level 1C); (3) Avoid early parenteral nutrition (within 7 d before ICU admission) to reduce the incidence of nosocomial infections (evidence level 2B); (4) Routine attempts to provide small amounts of enteral nutrition should be made (evidence level 2D).
(4) AGI Grade IV (Gastrointestinal failure with distant organ dysfunction)
AGI progresses to a life-threatening state, with patients experiencing MODS and deteriorating shock, posing an imminent risk to life. The patient’s overall condition sharply deteriorates, accompanied by distant organ dysfunction. This may include intestinal ischemic necrosis, gastrointestinal bleeding leading to hemorrhagic shock, Ogilvie’s syndrome (acute colonic pseudo-obstruction), or ACS requiring urgent decompression.
Treatment principles: Emergency laparotomy or other urgent interventions (such as colonoscopic decompression) (evidence level 1D).