Box 1: Definitions Used in the Delphi Process


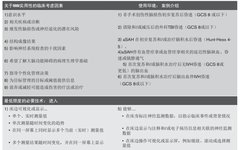
The Use Environment for Multimodal Monitoring




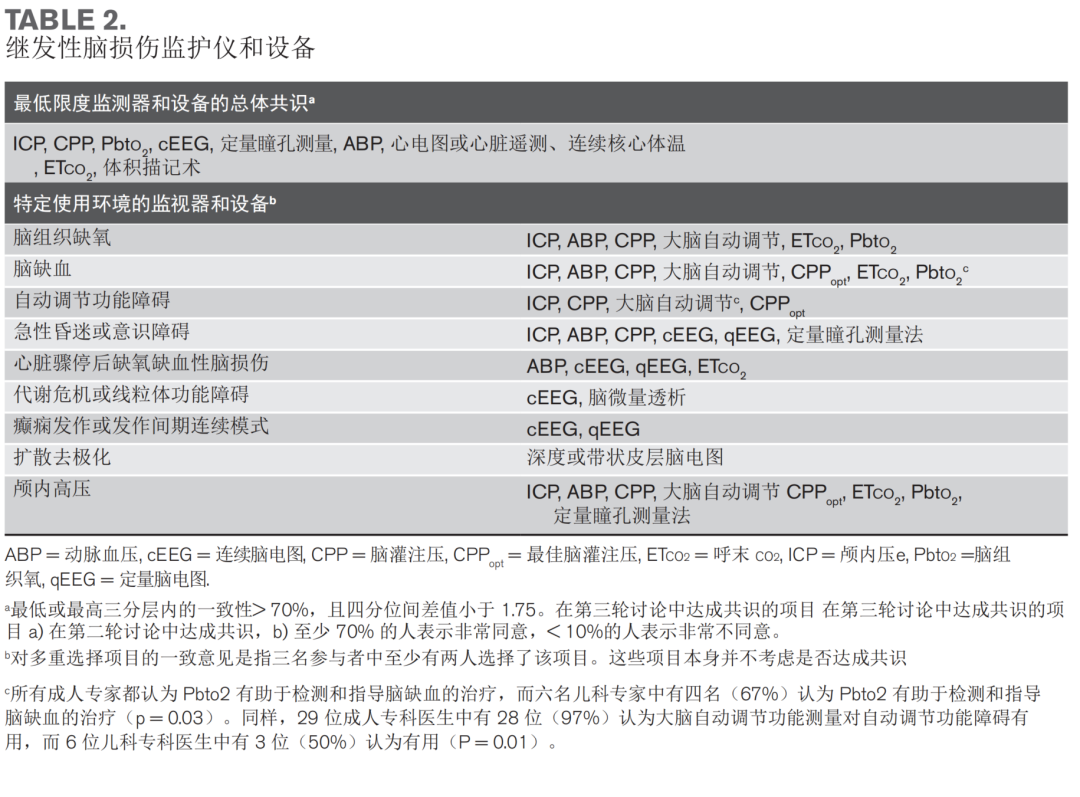
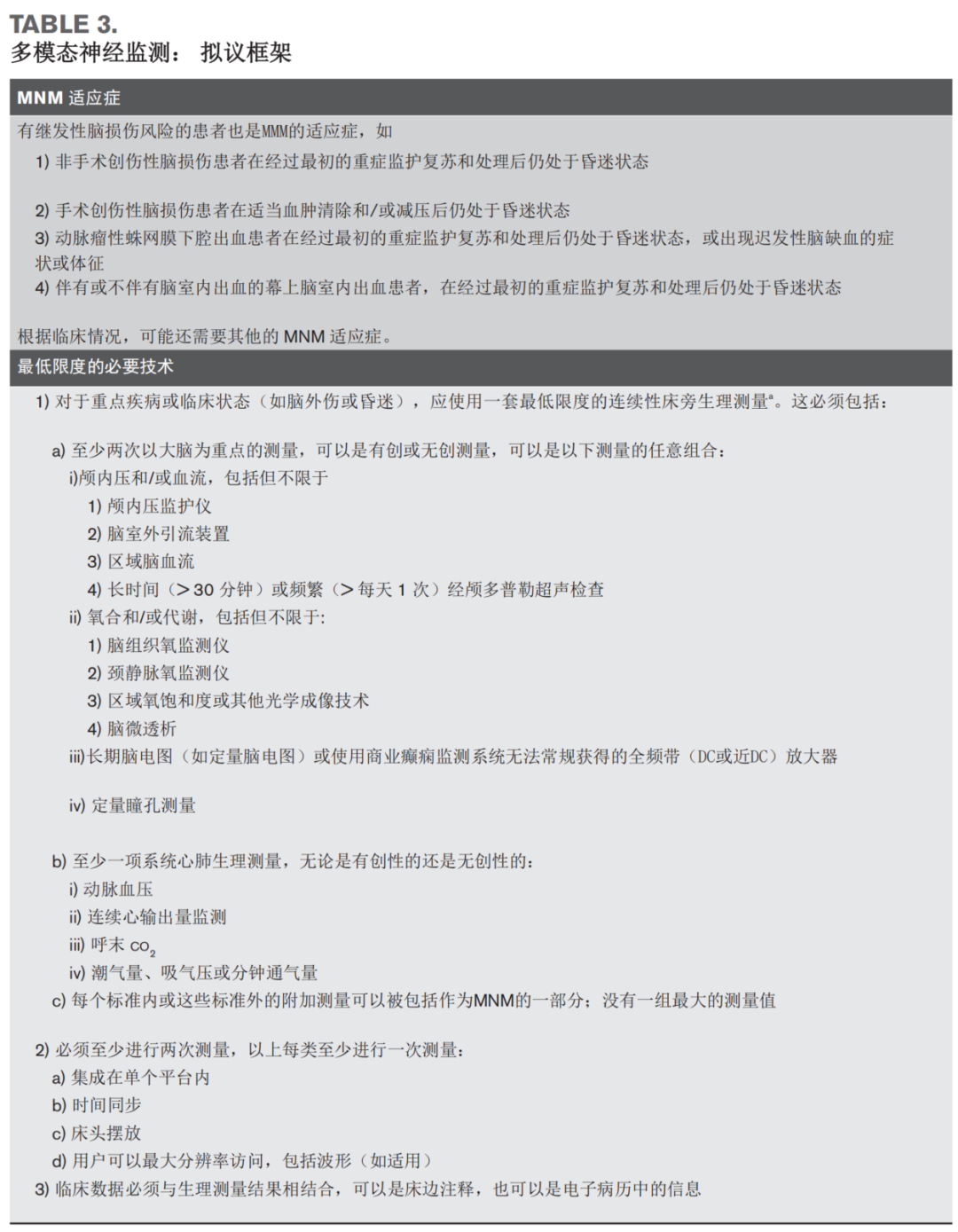
Minimum Required Monitors, Devices, and Technologies




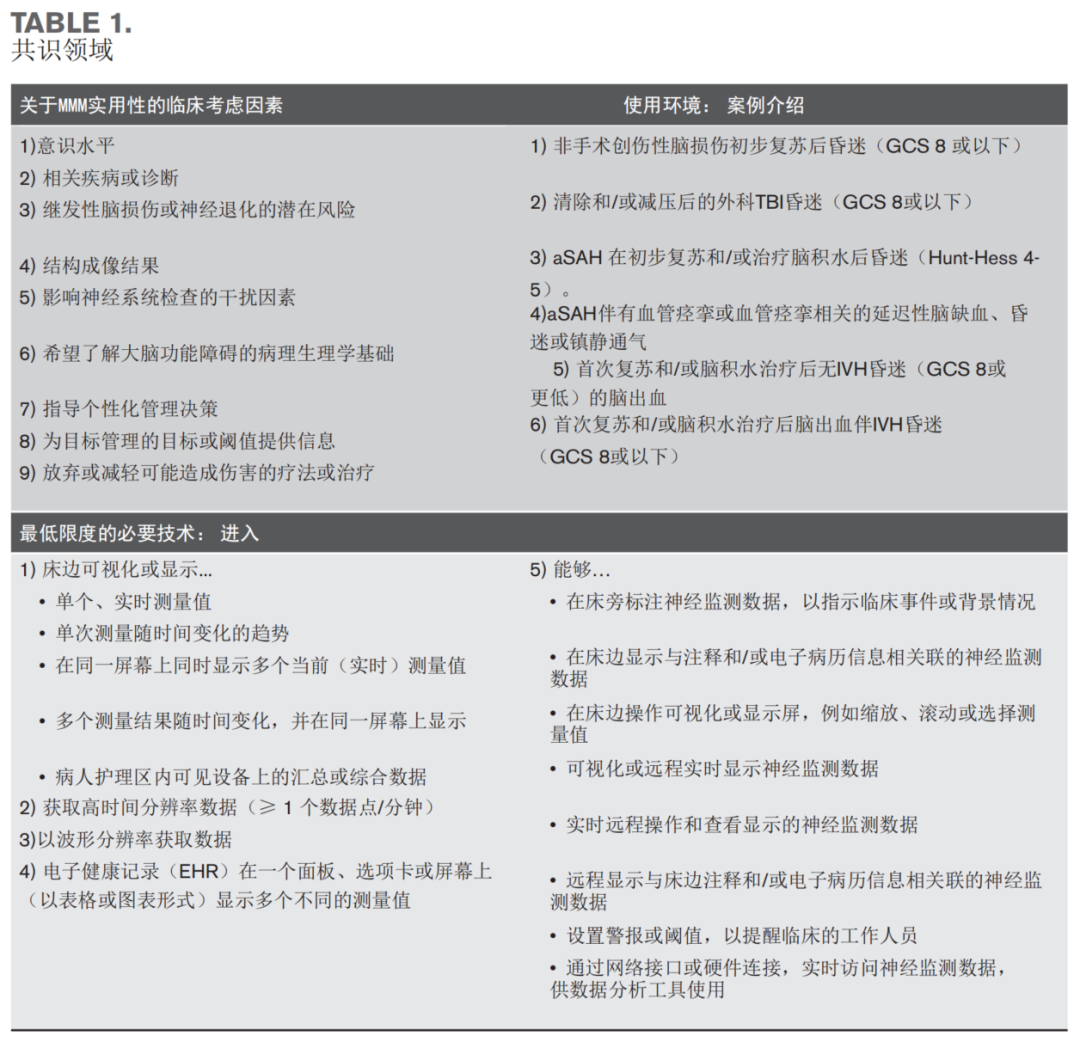
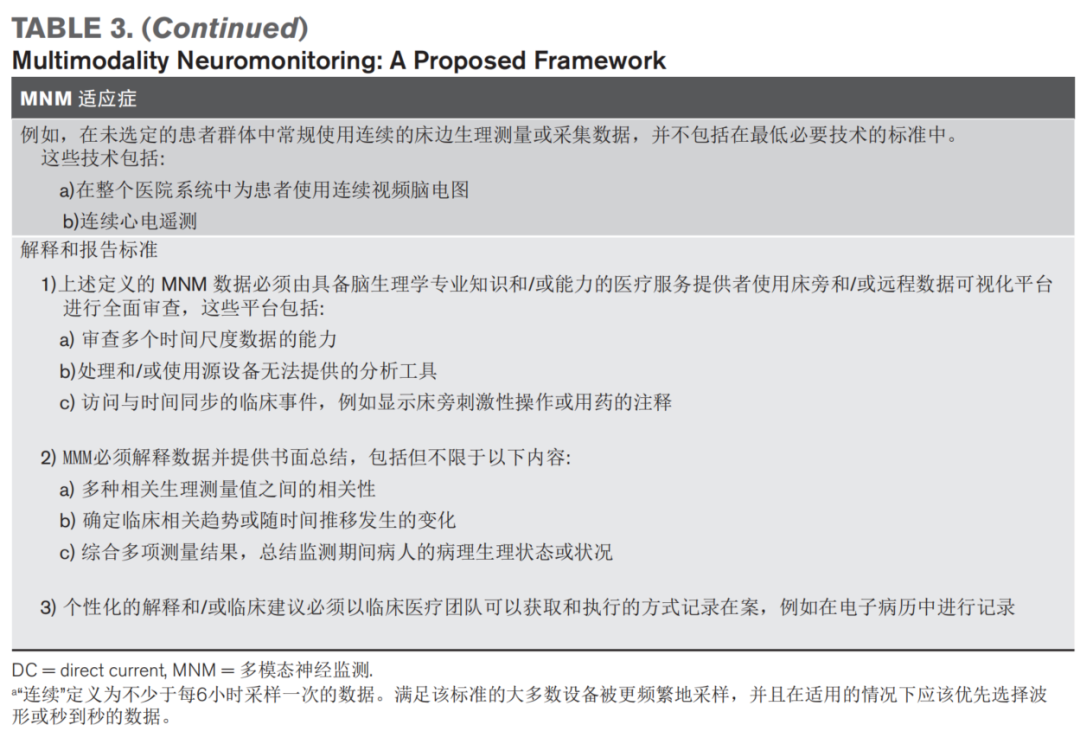
Minimum Necessary Clinical Efforts




Implementing Neuromonitoring




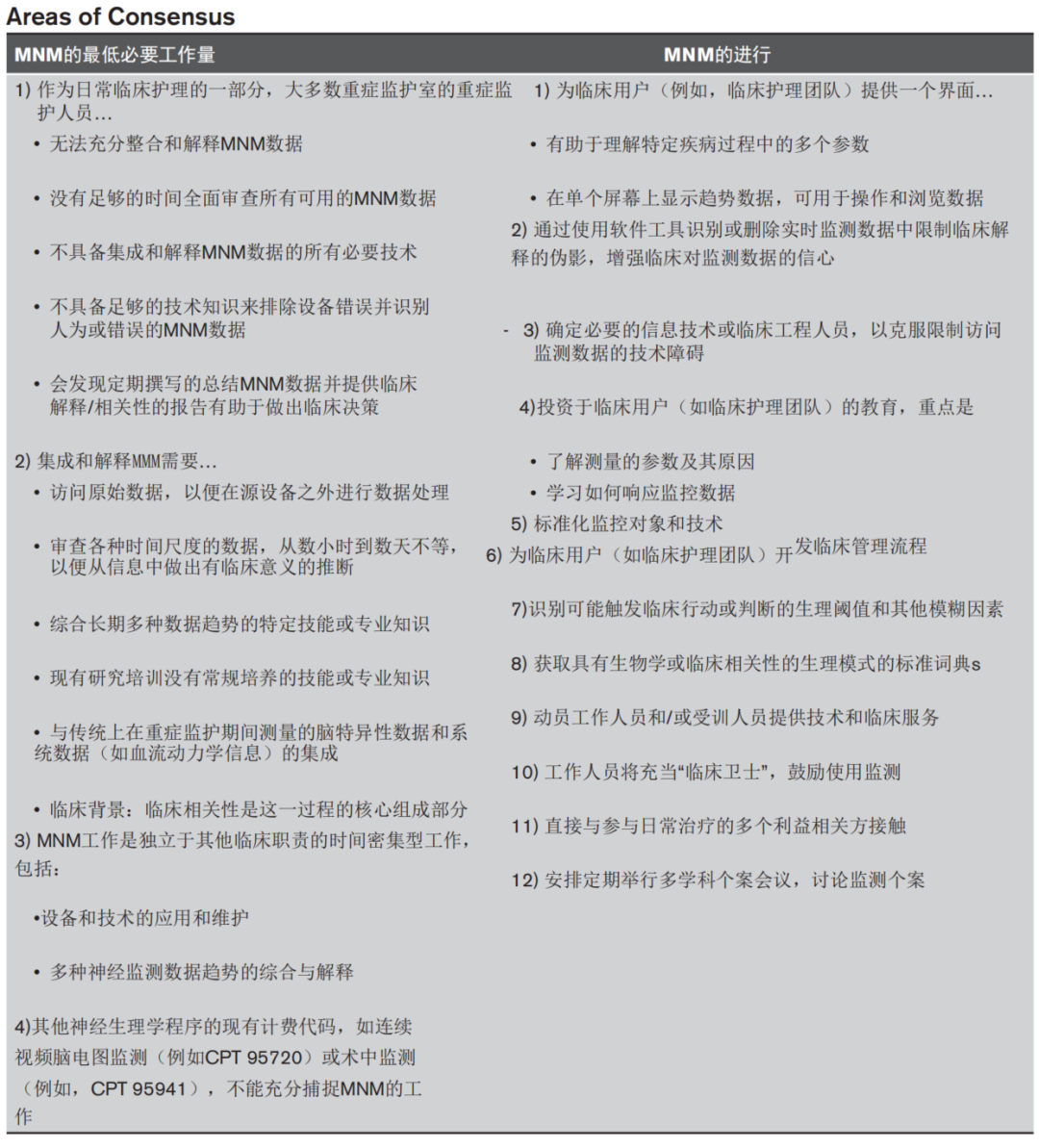
Training Background and Educational Opportunities



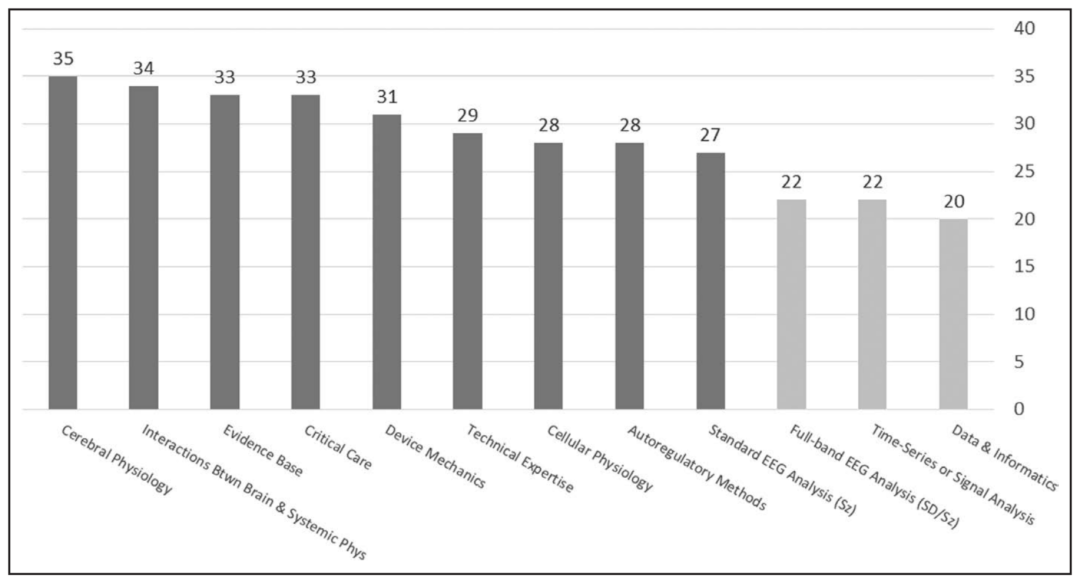
Figure 2. Core Concepts Required for Clinical Neuromonitoring. Participants were asked to select each core concept, which were deemed to have a sufficient knowledge base for clinicians to understand and interpret multimodal neuromonitoring information. Dark gray concepts reached consensus, meaning that more than two of the three participants selected these concepts; light gray concepts did not reach a consensus threshold. The y-axis reflects the number of participants selecting each concept among a total of 35 participants. EEG = electroencephalography, sd = spread depolarization, Sz = seizure



Discussion




Conclusion




Key Points


Source:Practice Standards for the Use of Multimodality Neuromonitoring: A Delphi Consensus Process
Critical Care Medicine
DOI: 10.1097/CCM.0000000000006016
