Skip to content
Patient, female, 51 years old, thyroid nodule found during physical examination one week ago, no discomfort in the neck, no pain, no hoarseness, no chest tightness, no palpitations, no excessive sweating, no weight loss, no tremors, no difficulty breathing, no fever, and no polydipsia or polyuria.
Thyroid and bilateral neck ultrasound examination:
(1) Routine ultrasound – 2D + color Doppler
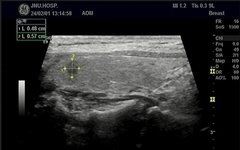
A nodule was seen in the upper pole of the right lobe of the thyroid, measuring approximately 5*6mm, vertical position, with irregular margins, no surrounding halo, solid, hypoechoic, heterogeneous internal echogenicity, no significant calcification seen, and CDFI showed a small amount of blood flow signal (Figure 1, Figure 2). A nodule was seen in the middle and lower pole of the left lobe, measuring approximately 12*6mm, horizontal position, with smooth margins, no surrounding halo, mixed cystic-solid echogenicity, predominantly solid, heterogeneous internal echogenicity, and unclear punctate strong echogenicity, with a small amount of blood flow signal seen in CDFI (Figure 3, Figure 4).
No obvious abnormal lymph nodes were seen in the bilateral neck examination.
1. Nodule in the right lobe of the thyroid C-TIRADS 4C level
2. Nodule in the left lobe of the thyroid C-TIRADS 4A level
(2) Ultrasound elastography
Nodule in the upper pole of the right lobe of the thyroid: the image shows no deformation of the nodule as a whole, the lesion appears blue, elasticity score = 4 (Figure 5)
Nodule in the middle and lower pole of the left lobe of the thyroid: the image shows slight deformation at the nodule boundary, no deformation in the center, the lesion color is a mix of blue and green, elasticity score = 3 (Figure 6)
(3) Contrast-enhanced ultrasound
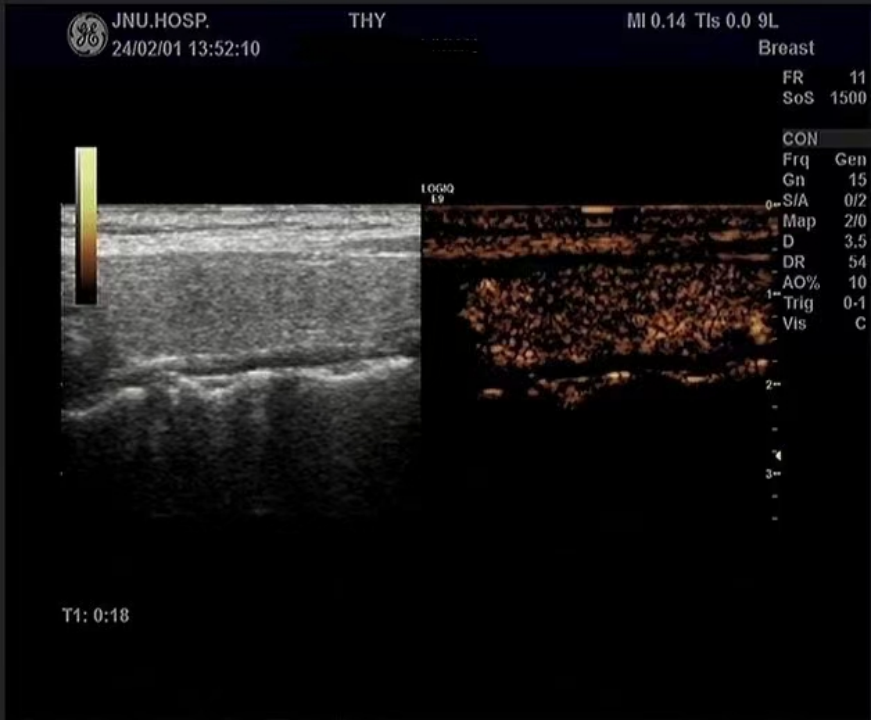
First observation of the nodule in the right lobe of the thyroid: intravenous injection of Sonovue 1.2ml, the nodule showed centripetal, uneven, low enhancement, the boundary unclear after enhancement, the range slightly larger than the two-dimensional measurement range, and the regression synchronized with the surrounding thyroid tissue (see ultrasound contrast time-intensity curve analysis attached). (Figure 7, Figure 8)
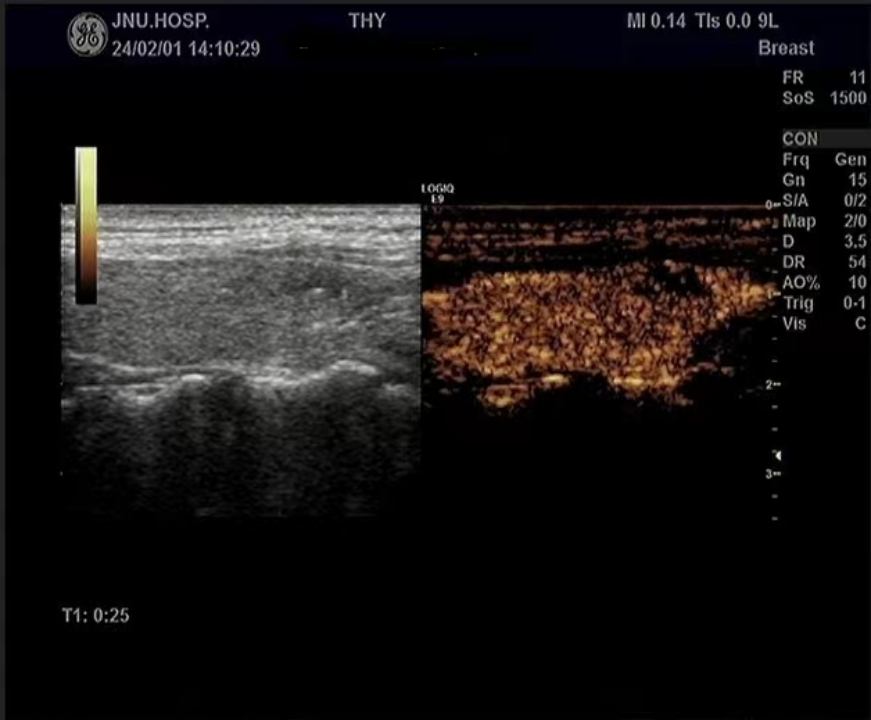
Second observation of the nodule in the left lobe of the thyroid: intravenous injection of Sonovue 1.2ml, the nodule showed diffuse, iso-enhancement, and no enhancement was seen in the cystic part of the nodule, with a clear boundary after enhancement, regular shape, and no significant change in nodule size compared to two-dimensional measurement, regression synchronized with the surrounding thyroid tissue (see ultrasound contrast time-intensity curve analysis attached). (Figure 9, Figure 10)
Contrast-enhanced ultrasound suggests:
1. Nodule in the right lobe of the thyroid C-TIRADS 5 level (increased by 1 level compared to routine ultrasound)
2. Nodule in the left lobe of the thyroid C-TIRADS 3 level (decreased by 1 level compared to routine ultrasound)
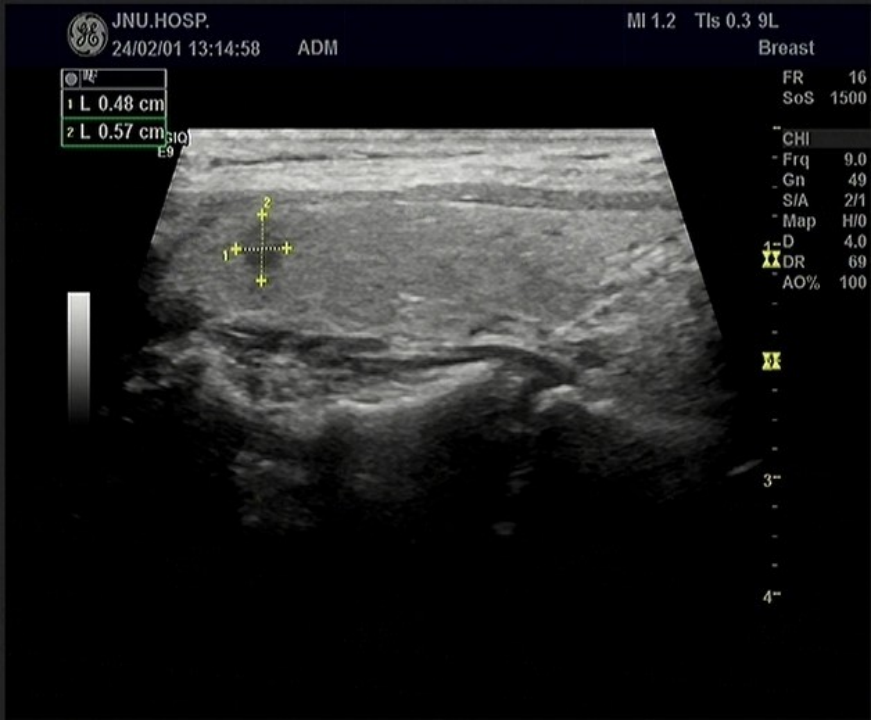 Figure 1 Nodule in the right lobe of the thyroid – 2D
Figure 1 Nodule in the right lobe of the thyroid – 2D
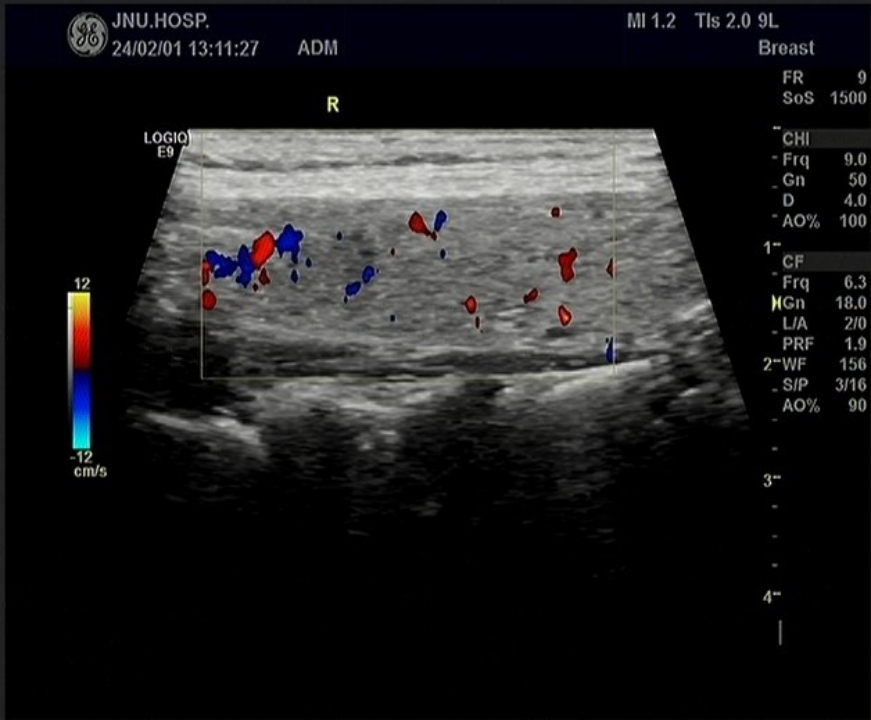 Figure 2 Nodule in the right lobe of the thyroid – color Doppler
Figure 2 Nodule in the right lobe of the thyroid – color Doppler
 Figure 3 Nodule in the left lobe of the thyroid – 2D
Figure 3 Nodule in the left lobe of the thyroid – 2D
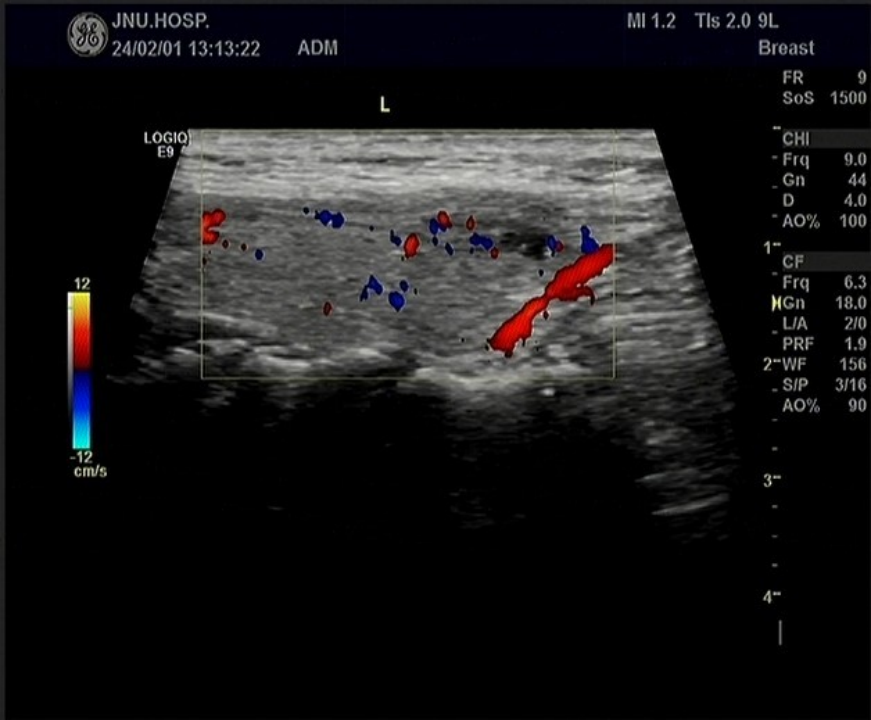 Figure 4 Nodule in the left lobe of the thyroid – color Doppler
Figure 4 Nodule in the left lobe of the thyroid – color Doppler
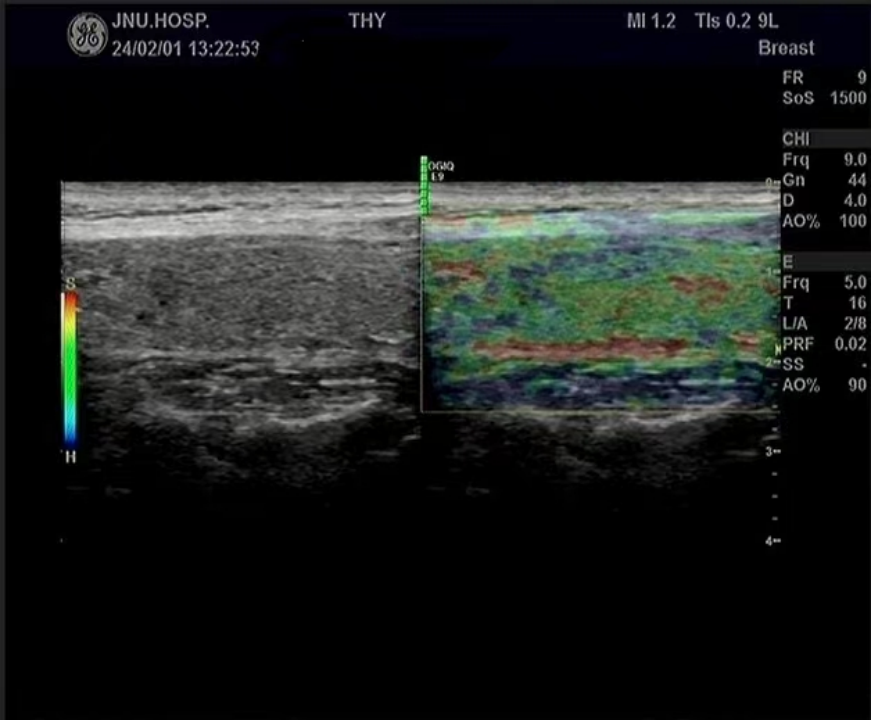 Figure 5 Nodule in the right lobe of the thyroid – strain elastography
Figure 5 Nodule in the right lobe of the thyroid – strain elastography
 Figure 6 Nodule in the left lobe of the thyroid – strain elastography
Figure 6 Nodule in the left lobe of the thyroid – strain elastography
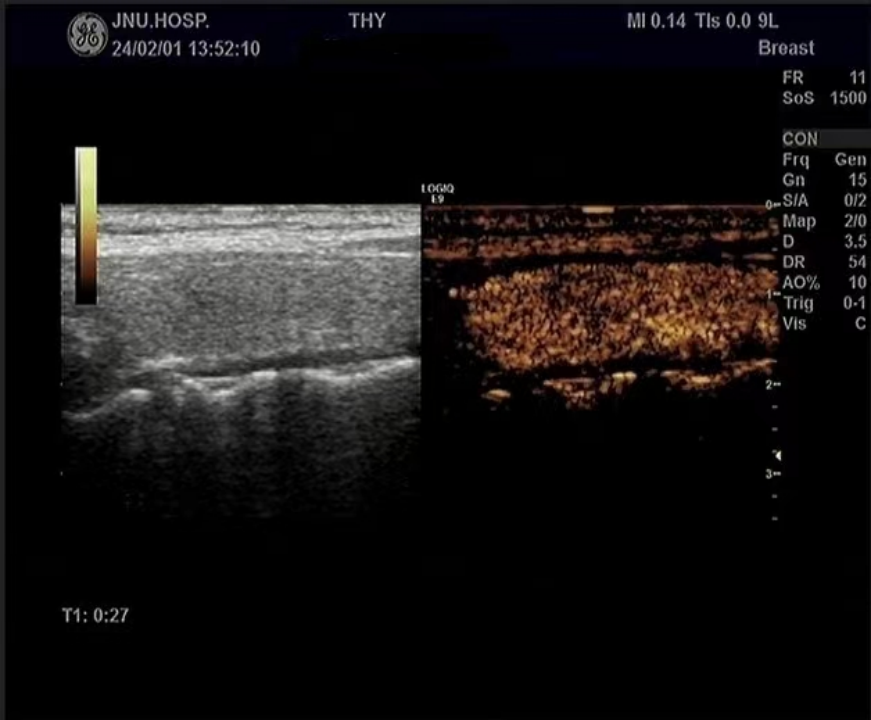 Figure 7 (1+2) Nodule in the right lobe of the thyroid – contrast-enhanced ultrasound (centripetal, uneven, low enhancement)
Figure 7 (1+2) Nodule in the right lobe of the thyroid – contrast-enhanced ultrasound (centripetal, uneven, low enhancement)
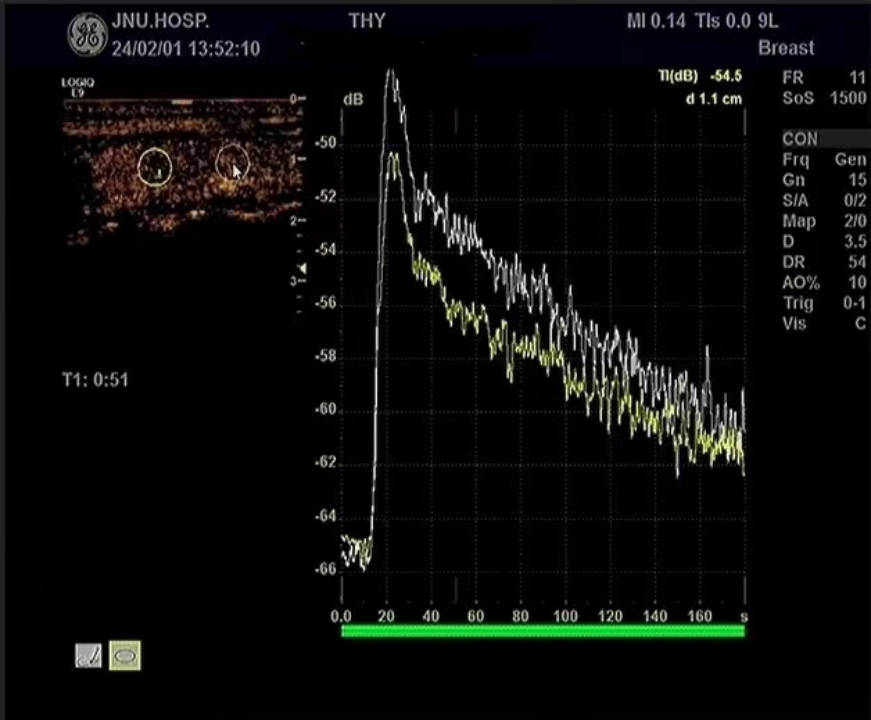 Figure 8 Nodule in the right lobe of the thyroid – ultrasound contrast time-intensity curve
Figure 8 Nodule in the right lobe of the thyroid – ultrasound contrast time-intensity curve
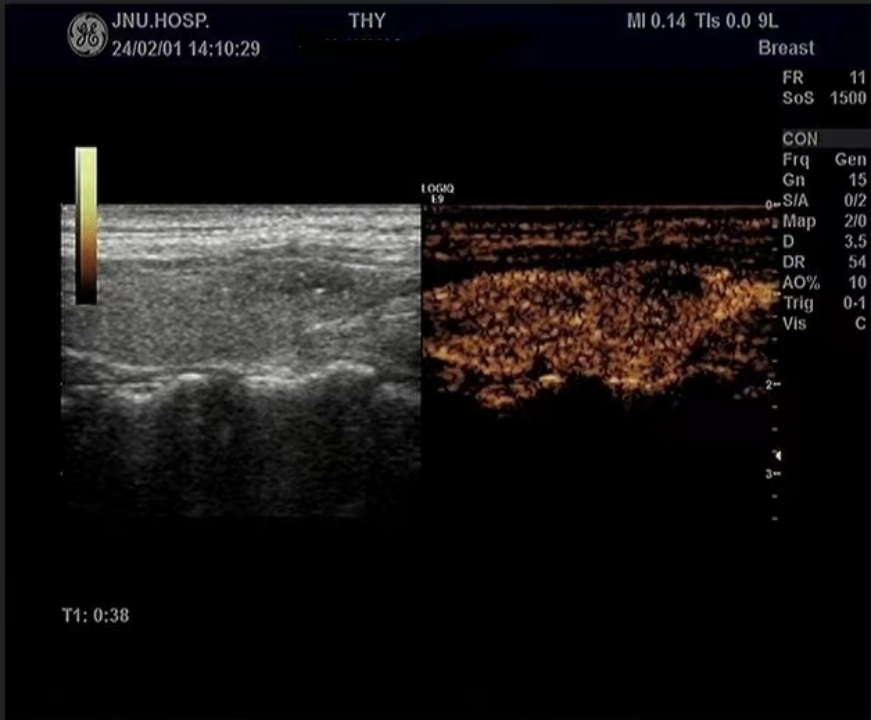 Figure 9 (1+2) Nodule in the left lobe of the thyroid – contrast-enhanced ultrasound (diffuse, iso-enhancement, no enhancement in the cystic part)
Figure 10 Pathology of the nodule in the right lobe of the thyroid – papillary carcinoma
Figure 9 (1+2) Nodule in the left lobe of the thyroid – contrast-enhanced ultrasound (diffuse, iso-enhancement, no enhancement in the cystic part)
Figure 10 Pathology of the nodule in the right lobe of the thyroid – papillary carcinoma
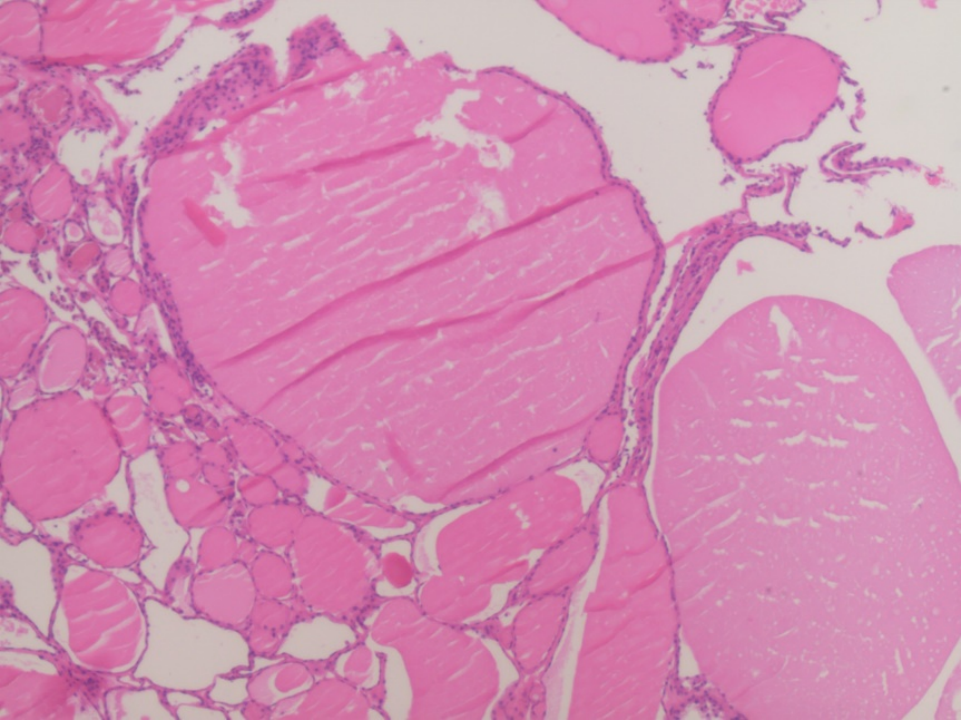 Figure 11 Pathology of the nodule in the left lobe of the thyroid – nodular goiter
Multimodal ultrasound is the combined application of two or more ultrasound examination methods for multi-angle analysis, thereby improving the differential diagnosis of benign and malignant thyroid nodules, which has been recognized in multicenter studies and widely applied in clinical diagnosis and treatment.
Currently, there are four ultrasound examination techniques for thyroid nodules, and the author will focus on two of them here.
1. Routine ultrasound examination (US) includes two-dimensional ultrasound and color Doppler flow imaging (CDFI), which is often used as the initial preliminary examination and has limitations in distinguishing between benign and malignant thyroid nodules.
2. Ultrasound elastography: evaluates the hardness of nodules, divided into strain elastography (SE) and shear wave elastography (SWE).
The author will mainly discuss strain elastography here.
Select the best cutting plane (generally the long-axis section of one side of the thyroid) and fix the probe, start the strain elastography mode, and display the gray-scale ultrasound and elastography modes in real time. During the operation, try to control the pressure curve to be evenly distributed, comparing the hardness of the surrounding tissues in the lesion area, based on the different color scores displayed in the elastography image (1-5 points):
1 point: The entire lesion area is significantly deformed, similar to the surrounding thyroid tissue, appearing uniformly green.
2 points: The lesion area is partially deformed, appearing a mix of blue and green.
3 points: The edge of the lesion area is deformed, with the surrounding tissue appearing green and the center appearing blue.
4 points: The entire lesion shows no significant deformation, appearing blue.
5 points: The lesion area is completely covered in blue, with a small amount of surrounding tissue also blue.
Generally, a nodule score of 1-3 suggests that the nodule is soft, indicating benignity, while a score of 4-5 suggests that the nodule is hard, indicating malignancy.
However, this is not absolute; for example, some benign nodules may have calcifications or fibrosis that increase their hardness, resulting in an elastography score often ≥4, leading to a certain overlap in ultrasound elastography characteristics between benign and malignant thyroid nodules. Additionally, the position of the nodule also influences the elastography assessment, such as nodules close to the thyroid capsule, adjacent to neck blood vessels or the trachea, which can affect the evaluation of the nodule’s elasticity. Therefore, the author believes that ultrasound elastography should be combined with the characteristics of routine ultrasound and contrast-enhanced ultrasound for comprehensive assessment.
3. Contrast-enhanced ultrasound (CEUS)
Contrast-enhanced ultrasound is performed by injecting a contrast agent (Sonovue) via peripheral venous access, allowing for more accurate visualization of microvascular blood flow perfusion within thyroid nodules, enhancing blood flow imaging. Based on the different characteristics of microvascular blood flow perfusion mechanisms in benign and malignant thyroid nodules, it provides a more accurate assessment of nodule properties.
Overall, the typical ultrasound contrast pattern for benign thyroid nodules is fast in or same in, slow out or same out, with contrast showing high uniform enhancement. If there is a complete high enhancement ring, it can also suggest a benign nodule.
For instance, the nodule in the left lobe of this case is a nodular goiter (with cystic changes), which lacks a fibrous capsule. The distribution of blood vessels within the nodule is not significantly different from that of the surrounding normal thyroid tissue, and the blood flow state is also similar to the surrounding thyroid, thus its contrast characteristics are uniform, iso-enhanced, with no enhancement in the cystic part.
Additionally, thyroid adenomas are also relatively common benign nodules, with ultrasound contrast characteristics showing fast in (this also suggests that the nodule in the left lobe of this case tends to be a nodular goiter with cystic changes rather than primarily considering thyroid adenoma, although cystic changes in adenomas are also quite common), centripetal, uniform high enhancement, with clear boundaries and regular shape at peak enhancement, showing a significant ring of high enhancement.
The typical ultrasound contrast pattern for malignant thyroid nodules is slow in, fast out or same out, with the contrast showing uneven, centripetal, low enhancement, with the nodule enlarging at peak enhancement, unclear boundaries, and irregular shape, as seen in the nodule in the right lobe of this case.
The reasons for this analysis include several points: ① Malignant nodules typically have a denser distribution of blood vessels around the nodule, while the distribution of vessels within is sparse, thus the enhancement direction appears centripetal. ② The blood vessels within malignant nodules are irregular in shape and distribution, which can lead to narrowing, occlusion, arteriovenous fistulas, etc., resulting in uneven distribution of new blood vessels, hence the enhancement pattern is uneven. ③ The functionality of numerous new blood vessels within malignant nodules is impaired, leading to insufficient blood supply, thus the enhancement level is low.
The author emphasizes another type of thyroid nodule, known as a so-called retraction nodule, which is essentially a type of thyroid cystic or cystic-solid nodule where cystic fluid is absorbed, and colloid decreases, causing the nodule to shrink and morphologically change. Such nodules may present low echogenicity, microcalcifications, an aspect ratio greater than 1, unclear margins, etc., which are characteristics of malignant nodules. This is similar to the two-dimensional ultrasound appearance of the nodule in the right lobe of the thyroid in the above patient; thus, routine ultrasound often rates it higher, TI-RADS ≥4A, easily misdiagnosed as thyroid papillary carcinoma. If there is a clear medical history (previous cystic or cystic-solid nodules at the same site in the thyroid), the diagnosis of retraction nodule can be confirmed. However, many patients have not undergone regular follow-up thyroid ultrasound examinations, and often discover such nodules during the first examination, making it relatively difficult to distinguish based solely on routine ultrasound. In such cases, performing contrast-enhanced ultrasound is very effective, with contrast showing no enhancement or only sparse punctate enhancement within the nodule, distinguishing it from the centripetal uneven low enhancement of thyroid papillary carcinoma nodules. Through contrast-enhanced ultrasound, the nodule rating can be directly adjusted to TI-RADS 2, allowing for regular follow-up observation and avoiding unnecessary punctures and surgeries.
4. Ultrasound-guided percutaneous fine-needle aspiration biopsy (FNA)
FNA is performed under real-time ultrasound guidance, using a fine needle to puncture the thyroid nodule to obtain cellular components for cytological diagnosis of the target lesion. It is currently an important standard for diagnosing thyroid nodules, being simple, convenient, minimally invasive, requiring no anesthesia, and having a high accuracy rate, providing a clinical basis for the next treatment plan. The case was hospitalized for surgical treatment and did not undergo FNA.
Ultrasound examination is the preferred imaging method for thyroid diseases. Multimodal ultrasound can provide various features of thyroid nodules from multiple angles, dimensions, and layers, including size, shape, echogenicity, blood flow distribution, microvascular perfusion, and tissue hardness, integrating information from each single-modal ultrasound for cross-validation and complementary information, comprehensively utilizing morphological and biological information to better assist ultrasound physicians in understanding and assessing the nature of nodules, thereby improving diagnostic accuracy.
Image and text sources: Provided by the author
[1]. Yang Qihui, Li Yinquan, Ma Xiaoqin. Research value of multimodal ultrasound in thyroid nodules. World Composite Medicine, 2022, 8(5): 30-33
[2]. Yu Miao, Guo Hao, Li Caijuan. Application value of multimodal ultrasound imaging in differentiating benign and malignant thyroid nodules. Imaging Technology, 2022, 34(5): 54-59.
[3]. Bai Yazhou. Application observation of multimodal ultrasound in the differential diagnosis of thyroid nodules. Journal of Qiqihar Medical College, 2022, 43(17): 1621-1625.
[4]. Huang Lili, Zhang Aihong, Yang Lei. Discussing the diagnostic value of combined multimodal ultrasound with contrast-enhanced ultrasound and elastography in the TI-RADS grading of thyroid nodules. Smart Health, 2021, 7(31): 1-3.
Figure 11 Pathology of the nodule in the left lobe of the thyroid – nodular goiter
Multimodal ultrasound is the combined application of two or more ultrasound examination methods for multi-angle analysis, thereby improving the differential diagnosis of benign and malignant thyroid nodules, which has been recognized in multicenter studies and widely applied in clinical diagnosis and treatment.
Currently, there are four ultrasound examination techniques for thyroid nodules, and the author will focus on two of them here.
1. Routine ultrasound examination (US) includes two-dimensional ultrasound and color Doppler flow imaging (CDFI), which is often used as the initial preliminary examination and has limitations in distinguishing between benign and malignant thyroid nodules.
2. Ultrasound elastography: evaluates the hardness of nodules, divided into strain elastography (SE) and shear wave elastography (SWE).
The author will mainly discuss strain elastography here.
Select the best cutting plane (generally the long-axis section of one side of the thyroid) and fix the probe, start the strain elastography mode, and display the gray-scale ultrasound and elastography modes in real time. During the operation, try to control the pressure curve to be evenly distributed, comparing the hardness of the surrounding tissues in the lesion area, based on the different color scores displayed in the elastography image (1-5 points):
1 point: The entire lesion area is significantly deformed, similar to the surrounding thyroid tissue, appearing uniformly green.
2 points: The lesion area is partially deformed, appearing a mix of blue and green.
3 points: The edge of the lesion area is deformed, with the surrounding tissue appearing green and the center appearing blue.
4 points: The entire lesion shows no significant deformation, appearing blue.
5 points: The lesion area is completely covered in blue, with a small amount of surrounding tissue also blue.
Generally, a nodule score of 1-3 suggests that the nodule is soft, indicating benignity, while a score of 4-5 suggests that the nodule is hard, indicating malignancy.
However, this is not absolute; for example, some benign nodules may have calcifications or fibrosis that increase their hardness, resulting in an elastography score often ≥4, leading to a certain overlap in ultrasound elastography characteristics between benign and malignant thyroid nodules. Additionally, the position of the nodule also influences the elastography assessment, such as nodules close to the thyroid capsule, adjacent to neck blood vessels or the trachea, which can affect the evaluation of the nodule’s elasticity. Therefore, the author believes that ultrasound elastography should be combined with the characteristics of routine ultrasound and contrast-enhanced ultrasound for comprehensive assessment.
3. Contrast-enhanced ultrasound (CEUS)
Contrast-enhanced ultrasound is performed by injecting a contrast agent (Sonovue) via peripheral venous access, allowing for more accurate visualization of microvascular blood flow perfusion within thyroid nodules, enhancing blood flow imaging. Based on the different characteristics of microvascular blood flow perfusion mechanisms in benign and malignant thyroid nodules, it provides a more accurate assessment of nodule properties.
Overall, the typical ultrasound contrast pattern for benign thyroid nodules is fast in or same in, slow out or same out, with contrast showing high uniform enhancement. If there is a complete high enhancement ring, it can also suggest a benign nodule.
For instance, the nodule in the left lobe of this case is a nodular goiter (with cystic changes), which lacks a fibrous capsule. The distribution of blood vessels within the nodule is not significantly different from that of the surrounding normal thyroid tissue, and the blood flow state is also similar to the surrounding thyroid, thus its contrast characteristics are uniform, iso-enhanced, with no enhancement in the cystic part.
Additionally, thyroid adenomas are also relatively common benign nodules, with ultrasound contrast characteristics showing fast in (this also suggests that the nodule in the left lobe of this case tends to be a nodular goiter with cystic changes rather than primarily considering thyroid adenoma, although cystic changes in adenomas are also quite common), centripetal, uniform high enhancement, with clear boundaries and regular shape at peak enhancement, showing a significant ring of high enhancement.
The typical ultrasound contrast pattern for malignant thyroid nodules is slow in, fast out or same out, with the contrast showing uneven, centripetal, low enhancement, with the nodule enlarging at peak enhancement, unclear boundaries, and irregular shape, as seen in the nodule in the right lobe of this case.
The reasons for this analysis include several points: ① Malignant nodules typically have a denser distribution of blood vessels around the nodule, while the distribution of vessels within is sparse, thus the enhancement direction appears centripetal. ② The blood vessels within malignant nodules are irregular in shape and distribution, which can lead to narrowing, occlusion, arteriovenous fistulas, etc., resulting in uneven distribution of new blood vessels, hence the enhancement pattern is uneven. ③ The functionality of numerous new blood vessels within malignant nodules is impaired, leading to insufficient blood supply, thus the enhancement level is low.
The author emphasizes another type of thyroid nodule, known as a so-called retraction nodule, which is essentially a type of thyroid cystic or cystic-solid nodule where cystic fluid is absorbed, and colloid decreases, causing the nodule to shrink and morphologically change. Such nodules may present low echogenicity, microcalcifications, an aspect ratio greater than 1, unclear margins, etc., which are characteristics of malignant nodules. This is similar to the two-dimensional ultrasound appearance of the nodule in the right lobe of the thyroid in the above patient; thus, routine ultrasound often rates it higher, TI-RADS ≥4A, easily misdiagnosed as thyroid papillary carcinoma. If there is a clear medical history (previous cystic or cystic-solid nodules at the same site in the thyroid), the diagnosis of retraction nodule can be confirmed. However, many patients have not undergone regular follow-up thyroid ultrasound examinations, and often discover such nodules during the first examination, making it relatively difficult to distinguish based solely on routine ultrasound. In such cases, performing contrast-enhanced ultrasound is very effective, with contrast showing no enhancement or only sparse punctate enhancement within the nodule, distinguishing it from the centripetal uneven low enhancement of thyroid papillary carcinoma nodules. Through contrast-enhanced ultrasound, the nodule rating can be directly adjusted to TI-RADS 2, allowing for regular follow-up observation and avoiding unnecessary punctures and surgeries.
4. Ultrasound-guided percutaneous fine-needle aspiration biopsy (FNA)
FNA is performed under real-time ultrasound guidance, using a fine needle to puncture the thyroid nodule to obtain cellular components for cytological diagnosis of the target lesion. It is currently an important standard for diagnosing thyroid nodules, being simple, convenient, minimally invasive, requiring no anesthesia, and having a high accuracy rate, providing a clinical basis for the next treatment plan. The case was hospitalized for surgical treatment and did not undergo FNA.
Ultrasound examination is the preferred imaging method for thyroid diseases. Multimodal ultrasound can provide various features of thyroid nodules from multiple angles, dimensions, and layers, including size, shape, echogenicity, blood flow distribution, microvascular perfusion, and tissue hardness, integrating information from each single-modal ultrasound for cross-validation and complementary information, comprehensively utilizing morphological and biological information to better assist ultrasound physicians in understanding and assessing the nature of nodules, thereby improving diagnostic accuracy.
Image and text sources: Provided by the author
[1]. Yang Qihui, Li Yinquan, Ma Xiaoqin. Research value of multimodal ultrasound in thyroid nodules. World Composite Medicine, 2022, 8(5): 30-33
[2]. Yu Miao, Guo Hao, Li Caijuan. Application value of multimodal ultrasound imaging in differentiating benign and malignant thyroid nodules. Imaging Technology, 2022, 34(5): 54-59.
[3]. Bai Yazhou. Application observation of multimodal ultrasound in the differential diagnosis of thyroid nodules. Journal of Qiqihar Medical College, 2022, 43(17): 1621-1625.
[4]. Huang Lili, Zhang Aihong, Yang Lei. Discussing the diagnostic value of combined multimodal ultrasound with contrast-enhanced ultrasound and elastography in the TI-RADS grading of thyroid nodules. Smart Health, 2021, 7(31): 1-3.