Introduction
Tricuspid regurgitation (TR) is a common valvular disease. Mild TR is a benign condition, but as age increases, the severity of TR can gradually worsen, and severe TR significantly increases mortality. Moreover, more studies indicate that TR patients often undergo surgery later, mainly due to low surgical volume and higher perioperative risks associated with isolated tricuspid valve surgery. Currently, there is no good method for clinical risk assessment in TR patients. A simple scoring system to measure TR-related risks will determine which patients would benefit from early intervention to reduce overall mortality in such patients. In August 2022, Lara-Breitinger et al. published a study that developed a simple score using demographic variables and conventional clinical data, removing certain variables related to TR etiology and some echocardiographic measurements, with the primary aim of making it usable by non-cardiologists. Recently, the research team further validated the application prospects of the TRIO score in TR patients with pulmonary hypertension (PH).

Research Methods
Study Population
This single-center retrospective cohort study primarily analyzed patients with severe (i.e., moderate or greater) TR recorded by echocardiography at the Mayo Clinic from January 1, 2005, to December 31, 2016. Patients aged ≤18 years, those with a history of tricuspid valve surgery, or those who refused to authorize the study were excluded. The primary endpoint was all-cause mortality.
Echocardiographic Definitions
TR severity was defined according to ASE and EACI guidelines, with severe TR defined by any of the following criteria: (1) tricuspid annular dilation without leaflet tethering or significant central jet (greater than 50% of the right atrium); (2) vena contracta width (VCW) ≥0.7 cm; (3) dense triangular continuous wave jet or sinusoidal pattern; (4) hepatic venous systolic flow reversal; (5) effective regurgitant orifice area (EROA) >0.4 cm² and regurgitant volume ≥45 mL. Moderate TR was defined as VCW: 0.3-0.69 cm, EROA 0.2-0.4 cm², and regurgitant volume 30-44 mL. If there was inconsistency in the definitions of moderate and severe TR by the echocardiographer, it was defined as moderate-severe TR.
Score Construction
After data analysis and construction of the TRIO score in the training set, the score was validated in the validation set. The hazard ratio (HR) values in the final multivariable Cox regression model were used to develop the TRIO score. Statistically significant parameters in the TRIO score were assigned 1 or 2 points, with 2 points reflecting a higher HR (>1.5). The risk score thresholds for low, medium, and high risk were selected based on event risk detection by score in the training set. The risk score was then applied to the validation set to assess risk stratification.
Research Results
Step 1 Clinical Characteristics and Prognosis of the Entire Study Population
A total of 13,608 patients with moderate or greater TR were included in the study, analyzing baseline data and prognosis across three groups: moderate, moderate-severe, and severe TR. During a median follow-up of 6.5 years (IQR, 0.8-11.0) after diagnosis of TR, 7,823 out of 13,608 patients (57%) experienced all-cause mortality. Kaplan-Meier analysis showed that the 5-year and 10-year mortality rates for moderate TR patients were 53% and 80%, for moderate-severe TR patients were 63% and 87%, and for severe TR patients were 71% and 91%, with increased mortality risk for moderate-severe TR (HR, 1.24; 95% CI, 1.17-1.31; P<0.001) and severe TR (HR, 1.55; 95% CI, 1.47-1.64; P<0.001) compared to moderate TR. (Figure 1).
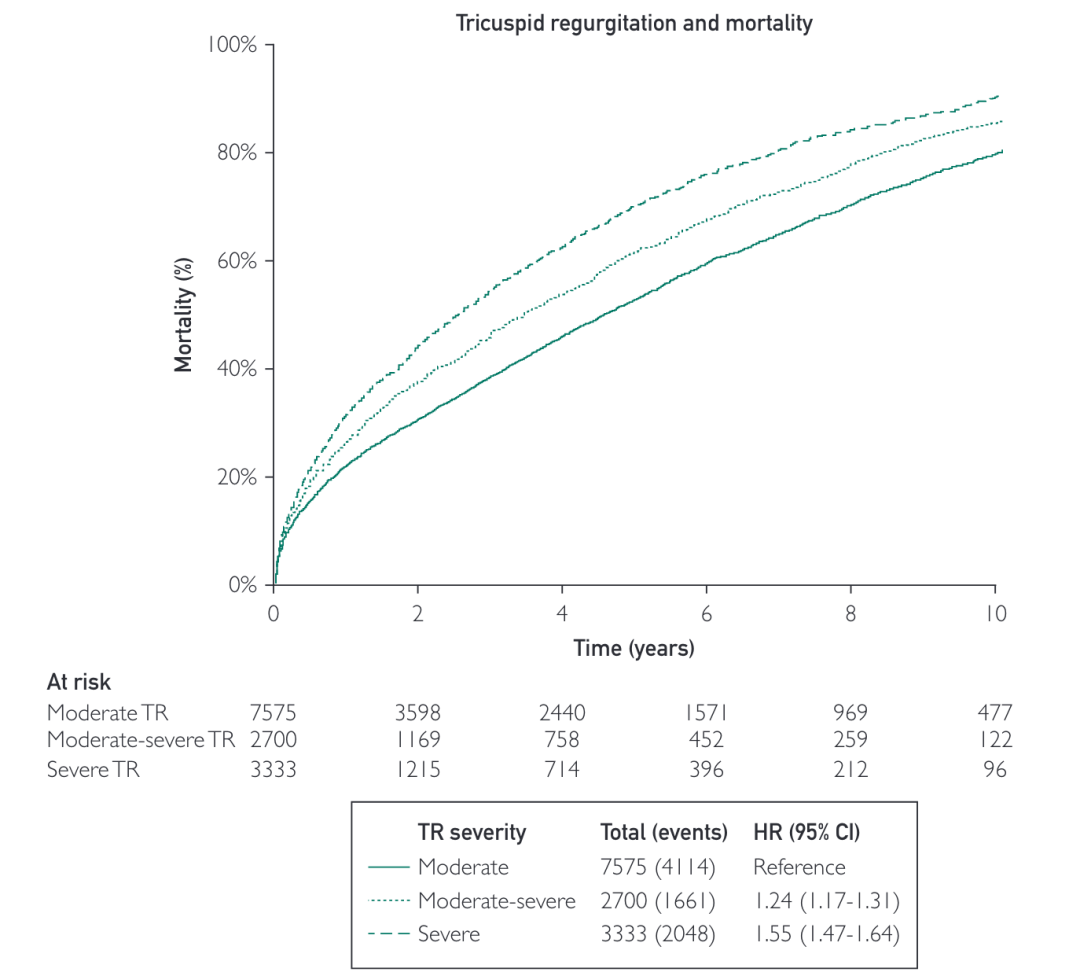
Figure 1 Survival Curves for TR Patients
This step also aimed to preliminarily assess whether the single-center population has a certain representativeness, as a recent study published in the European Journal of Heart Failure analyzed 13,469 patients with secondary TR and heart failure (HF) from community hospitals, finding similar results. Compared to HF patients with no or mild secondary TR, moderate TR (HR, 1.58; 95% CI, 1.48-1.69, p<0.001) and severe secondary TR (HR, 2.19; 95% CI, 2.01-2.38, p<0.001) had increased mortality (Figure 2).
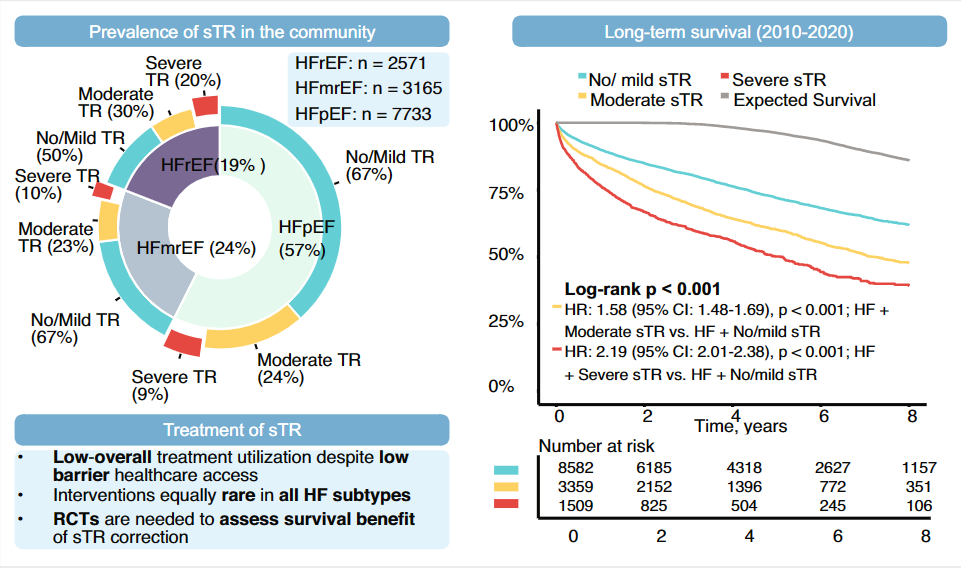
Figure 2 Epidemiology, Prognosis, and Treatment Status of Secondary Tricuspid Regurgitation (sTR) in HF Patients from Community Hospitals
Step 2 Constructing Training and Validation Sets
Patients were randomly assigned to the training set (N=10,205 [75%]) and validation set (N=3,403 [25%]) in a 3:1 ratio. This step aimed to assess baseline data of patients across two groups while minimizing differences between baseline data of the two groups to enhance the robustness of the model. Analysis confirmed that baseline characteristics were very similar between the two groups, and mortality rates were also very similar.
Step 3 Cox Regression Analysis of Factors Affecting TR Prognosis
Through univariate and multivariate Cox regression analyses, a multivariable model that could calculate the TRIO score was included (Table 1). In the multivariable analysis of the training set, important predictors of all-cause mortality included age 70-79 years (HR, 1.30; 95% CI, 1.21-1.39; P<0.0001), age ≥80 years (HR, 2.02; 95% CI, 1.89-2.16; P<0.0001), male (HR, 1.17; 95% CI, 1.11-1.23; P<0.001), serum creatinine ≥2 mg/dL (HR, 1.89; 95% CI, 1.76-2.04; P<0.0001), congestive heart failure (HR, 2.62; 95% CI, 1.53-1.72; P<0.0001), chronic lung disease (HR, 1.55; 95% CI, 1.46-1.65; P<0.0001), serum transaminases (AST) ≥40 U/L (HR, 1.38; 95% CI, 1.30-1.47; P<0.0001), heart rate ≥90 beats/min (HR, 1.38; 95% CI, 1.29-1.48; P<0.0001), and severe TR (HR, 1.34; 95% CI, 1.26-1.42; P<0.0001).
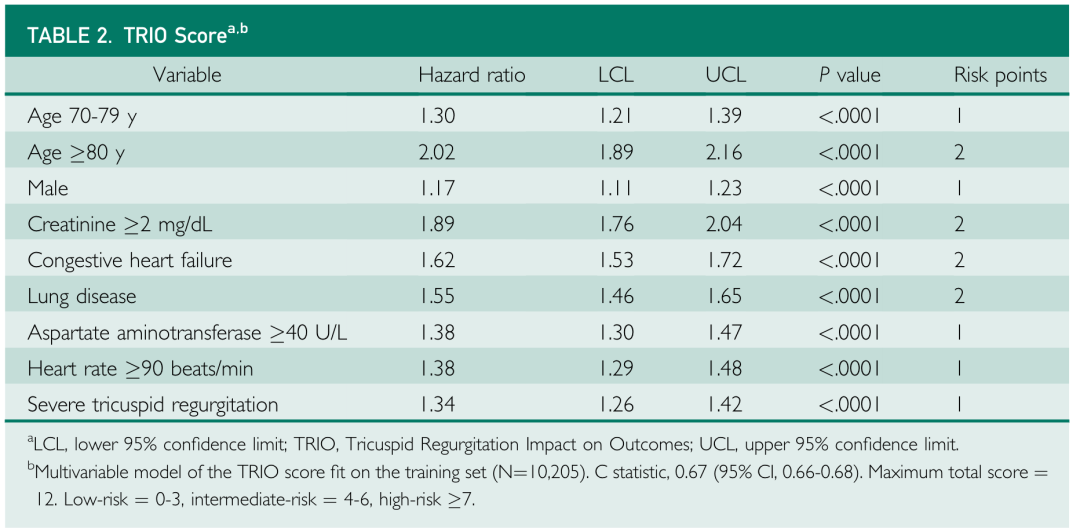
Table 1 Variables Included in the TRIO Score
Step 4 Constructing the TRIO Score and Calculating C-Statistic
The TRIO score was constructed by summing scores associated with eight clinical variables, with a total score of 12 points. In the training set, the C-statistic (i.e., area under the ROC curve) for the correlation of the TRIO score with all-cause mortality was 0.67 (95% CI, 0.66-0.68). In the validation set, the C-statistic was 0.67 (95% CI, 0.65-0.68).
Step 5 Validating the Predictive Value of the TRIO Score
The mortality rates by risk score are shown in Figure 3. The higher the risk score, the higher the mortality rate. The cutoff values for clinical use of the score were defined as low risk (total score, 0-3), medium risk (4-6), and high risk (7). The correlation of high-risk scores with 10-year mortality probability was 79%, for medium-risk scores it was 63%, and for low-risk scores it was 40%.
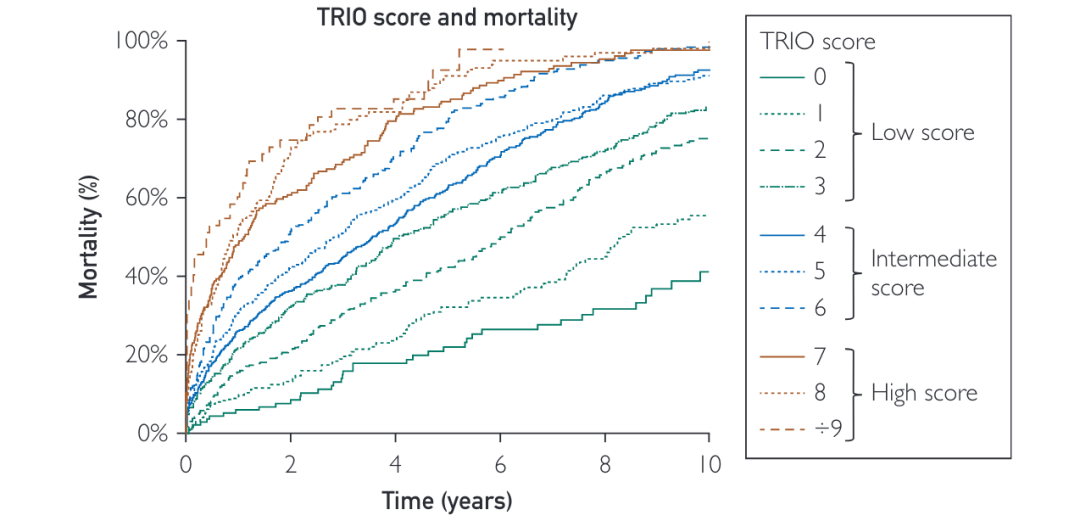
Figure 3 Survival Curves Classified by TRIO Score
Step 6 Testing the Robustness of the Model
(1) Removing TR Severity
To assess the patient population most likely to benefit from TR intervention, the researchers recalculated the TRIO score without TR severity as a parameter and further analyzed the impact of TR severity on mortality across risk categories in the validation set. For the overall population, mortality rates across different TRIO score risk strata were significantly influenced by TR severity (Figure 4). However, when stratifying the validation set according to the TRIO score, increased TR severity was associated with increased mortality in the low-risk group, but not in the medium-high risk groups.
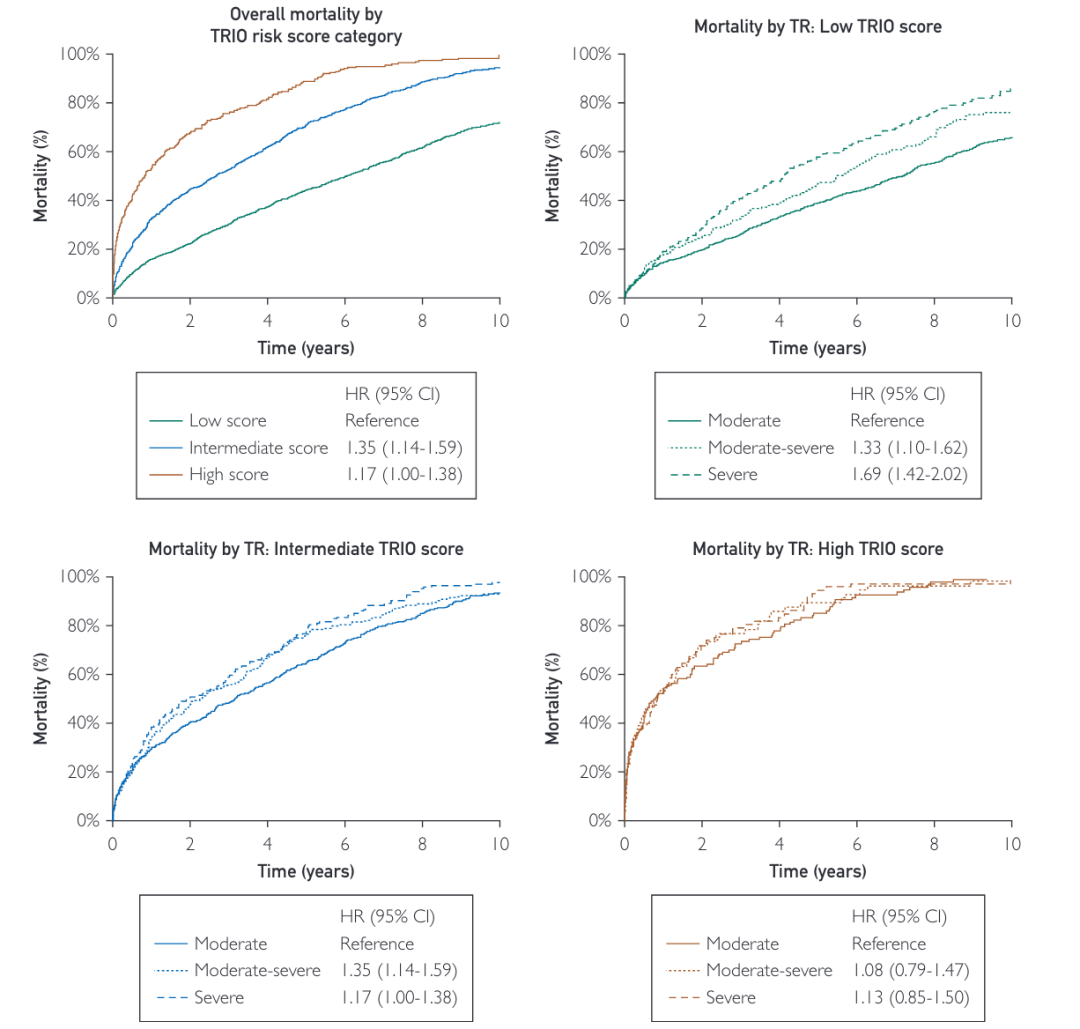
Figure 4 Survival Curves after Removing TR Severity from TRIO Score
(2) External Validation
The independent validation results of the TRIO score in data from 7,138 patients from two other research centers found that the C-statistic calculated for the risk scores in these two cohorts was also 0.67 (95% CI, 0.66-0.68), and the mortality rates calculated by risk stratification based on the TRIO score were similar to those in the internal validation set (Figure 5).
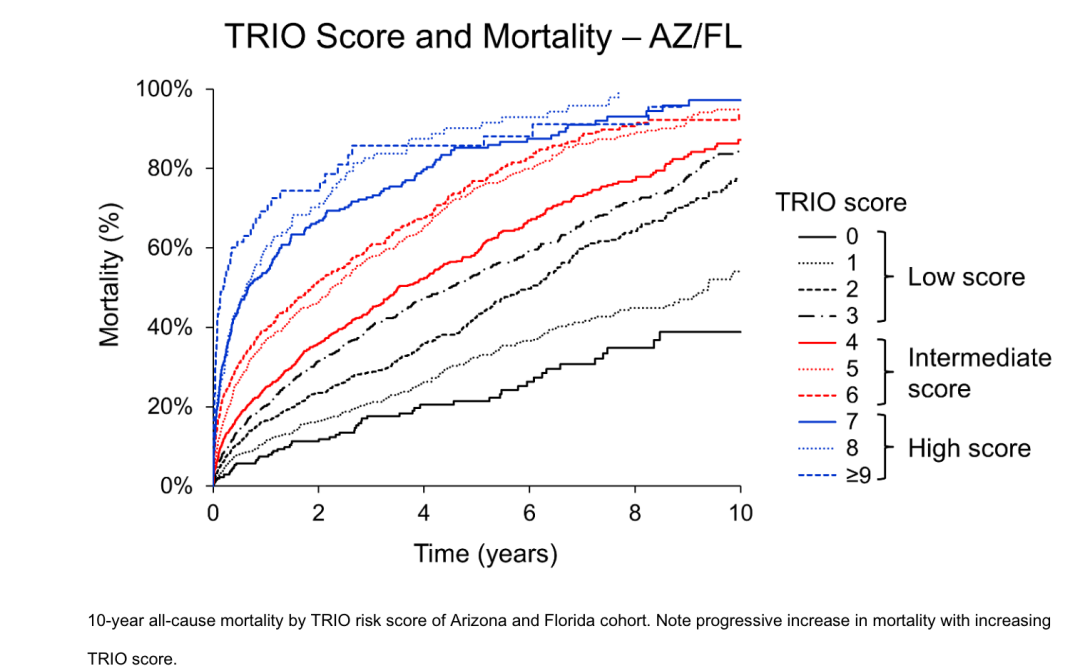
Figure 5 Survival Curves Classified by TRIO Score in External Validation Set
Step 7 Expanding Research
Recently, the research team selected 13,482 patients with recorded right ventricular systolic pressure (RVSP) from this population and grouped them based on the presence of pulmonary hypertension (PH, defined as echocardiographic RVSP >50 mmHg) to further study the application of the TRIO score in the PH population. The main findings of the study were: 1) The TRIO score can be used for risk stratification in TR and PH patients (Figure 6); 2) At all TRIO score levels, the mortality rate in PH patients was significantly higher than in non-PH patients, and the impact of PH was more pronounced in patients with lower TRIO scores; 3) In PH patients, other risk factors affecting mortality include elevated RVSP and NT-proBNP, pulmonary artery pulsatility index (PAPi; estimated by echocardiography) <4, and right ventricular dysfunction; 4) The incremental value of a multivariable model including RVSP, NT-pro-BNP, PAPi, and right ventricular dysfunction compared to the TRIO score alone was modest (C-statistic for TRIO was 0.62, and for the model was 0.65).
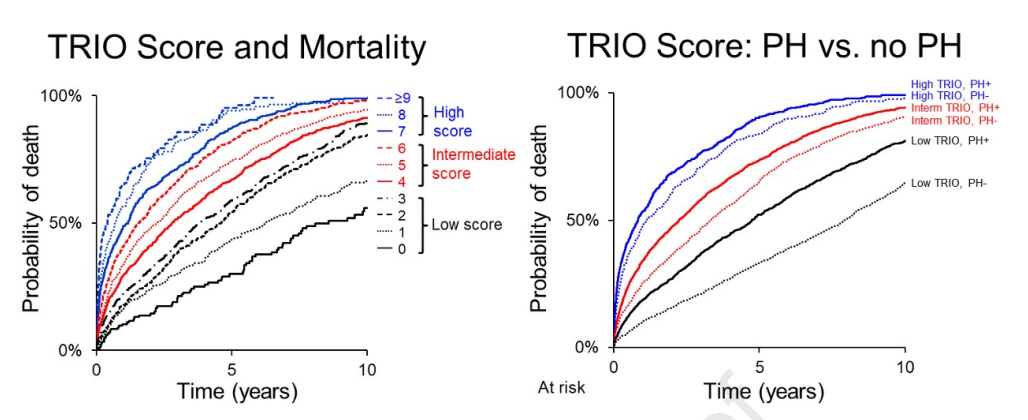
Figure 5 Impact of TRIO Score on Prognosis in Patients with Moderate TR and PH (Left) and Grouped by Pulmonary Hypertension (Right)
Research Summary
The TRIO score is a simple tool for risk assessment of moderate to severe TR patients based on eight common variables, easily calculated even in basic medical conditions. Although the C-statistic of this scoring system is relatively low, its clinical usability is relatively high since it does not include some clinically complex indicators such as echocardiography. Both studies indicate that the greatest impact on mortality from TR is in patients with lower TRIO scores, suggesting that this population may benefit the most from early tricuspid interventions. Further prospective studies are still needed to validate the clinical utility of this score. Additionally, the construction, validation, and subsequent related research processes of this score have certain reference significance.
Swipe up to read more
References:
[1] Lara-Breitinger KM, Scott CG, Nkomo VT, et al. Tricuspid Regurgitation Impact on Outcomes (TRIO): A Simple Clinical Risk Score. Mayo Clin Proc. 2022;97(8):1449-1461.
[2] Alabdaljabar MS, Naser JA, Kane CJ, et al. Tricuspid Regurgitation Impact on Outcomes (TRIO) score for risk stratification in patients with pulmonary hypertension [published online ahead of print, 2023 Jul 23]. J Am Soc Echocardiogr. 2023;S0894-7317(23)00364-4.
[3] Heitzinger G, Pavo N, Koschatko S, et al. Contemporary insights into the epidemiology, impact and treatment of secondary tricuspid regurgitation across the heart failure spectrum. Eur J Heart Fail. 2023;25(6):857-867.
· END ·
Copyright and Disclaimer:
The Yan Dao Medical Voice Network aims to build a media platform for academic dissemination by medical experts and to voice for healthcare professionals. All articles published through the Yan Dao Medical Voice Network WeChat public account, APP, and website hold copyright to the information within, and we only provide information transmission.
1. The Yan Dao Medical Voice Network reserves the right to technically process/delete content;
2. For reprinted or shared content, the Yan Dao Medical Voice Network will indicate the author and source;
3. The published articles do not represent the stance/views of the Yan Dao Medical Voice Network; if there are errors in the content, please feel free to point them out; 4. For content whose source cannot be confirmed, if it involves copyright or dispute issues, and if we unintentionally infringe on your rights, please contact us promptly, providing the URL of the content and relevant proof materials, and we will immediately correct or delete the relevant content after verification. This public account does not bear any responsibility and has the final interpretation rights for this statement.

For more information, click “Read the Original” to download “Yan Dao Medical Voice APP”