
Author:Stuart B Goodman, Stanford University Orthopedics, USA
Translator:Duan Ruimeng Reviewed by:Chen Xiantao
Inflammation: General Principles
Osteonecrosis encompasses a range of diseases that lead to the death of bone cells and bone marrow. Osteonecrosis can be localized or widespread (multifocal). Numerous different inciting factors are associated with osteonecrosis. Generally, ONFH is caused by traumatic events (such as femoral neck displacement fractures, hip dislocations, or closed reductions of hip dislocations), but it can also be non-traumatic, meaning not caused by mechanical injury. Traumatic etiologies are believed to directly damage the blood supply to the local area. Non-traumatic causes include high-dose corticosteroid use, excessive alcohol consumption, autoimmune diseases such as systemic lupus erythematosus (SLE), radiation therapy, chemotherapy, hypercoagulable states, sickle cell disease, Gaucher’s disease, and other causes. Osteonecrosis typically occurs in the epiphyseal and metaphyseal regions and can lead to bone collapse and secondary degenerative arthritis. Osteonecrosis must be distinguished from incomplete fractures caused by overuse, abnormal pathologic fractures, and other conditions. Osteonecrosis typically occurs in weight-bearing joints such as the hip (femoral head), knee (femoral and tibial condyles), and humerus (head), but can occur in virtually any bone and location. Most cases are associated with corticosteroid use or alcohol abuse, typically occurring in young patients of working age. Collapse of the affected joint leads to pain and end-stage arthritis. Therefore, early diagnosis of osteonecrosis is essential to assess and mitigate potential inciting factors to limit its progression to late stages. Furthermore, early diagnosis and treatment may prevent or reverse disease progression, thus preserving the patient’s own anatomy and avoiding joint replacement surgery. Unfortunately, a recent study on osteonecrosis at our tertiary care center showed that 77% of cases were diagnosed at late stages of ONFH, impacting the process of hip preservation.
Relationship Between Chronic Inflammation and Osteonecrosis
Despite the many etiologies associated with osteonecrosis, ultimately, they all involve insufficient oxygen and nutrient supply to the affected area (Figure 1). These events are associated with enhanced differentiation of bone marrow mesenchymal stem cells along adipogenic pathways and insufficient osteogenesis and angiogenesis. However, to some extent, the affected anatomical regions exhibit chronic inflammation, cell death, and histological evidence of impaired repair. Real-time imaging probe analyses show that activated macrophages and neutrophils persist locally six weeks after vascular cautery-induced osteonecrosis in mice. In other studies, hormone-related osteonecrosis in rats led to upregulation of the PRR toll-like receptor 4 (TLR4), with downstream adaptor proteins MyD88 and the major transcription factors of inflammatory proteins, nuclear factor-κB (NF-κB) and monocyte chemotactic protein-1 (MCP-1) also being upregulated.
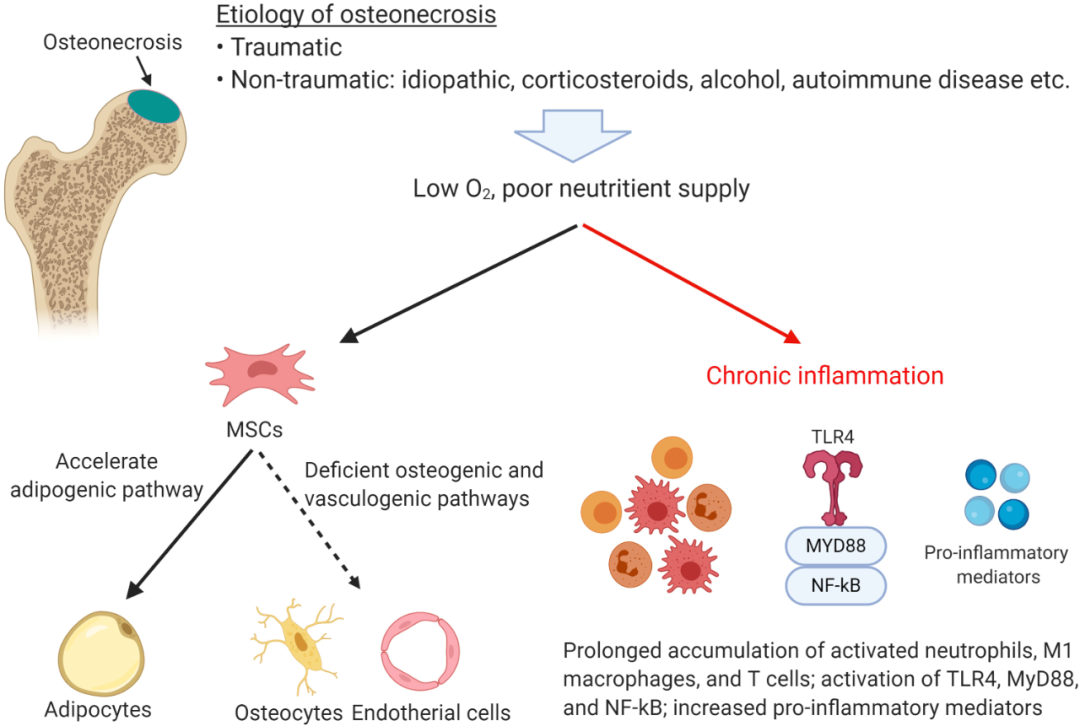
Notably, many molecules associated with acute and chronic inflammation, osteonecrosis, and bone healing overlap and play important roles in the activation of the innate immune system and tissue repair. NF-κB is the main pro-inflammatory transcription factor induced by injurious stimuli, activating pro-inflammatory factors or licensing MSCs. TLR4 is a PRR on the cell surface that can be activated by PAMPs, DAMPs, and other substances. TLR4 has two signaling pathways: MyD88-dependent (TLR4/MyD88/NF-κB) and MyD88-independent (TLR4/TRIF/IRF3). The MyD88-dependent pathway activates NF-κB and promotes the expression of the chemokine MCP-1. MCP-1 is a chemotactic agent for monocyte-macrophage lineage and MSC osteoblast lineage cells. MCP-1 induces proliferation of monocytes/macrophages and promotes differentiation and activation of osteoclasts. In pig models, byproducts of necrotic bone have been shown to upregulate a large number of pro-inflammatory cytokines, a mechanism dependent on macrophage activation of TLR4. This observation has been confirmed in hormone-related ONFH rat models, which exhibit excessive activation of TLR4/NF-κB and inhibition of the typical Wnt/β-catenin pathway (which regulates cell cycle, cell migration, and organogenesis). In one study, serum was collected from 20 patients at different stages of ONFH and compared with serum from a normal control group, identifying eight genes including TLR4 as potential serum biomarkers for disease severity. Other biomarkers include BIRC3, CBL, CCR5, LYN, PAK1, PTEN, and RAF1, which are related to inflammation, bone and cartilage metabolism, and angiogenesis.This suggests that potential biological strategies to alleviate complications of osteonecrosis may need to reduce chronic inflammation and promote osteogenesis and angiogenesis.
Strategies to Alleviate Chronic Inflammation and Promote Osteogenesis and Angiogenesis in ONFH
Healing of chronic critical-sized bone defects caused by trauma (delayed healing, nonunion), prior infections, periprosthetic bone resorption, and other causes is similar in many ways to the defects encountered in osteonecrosis. To some extent, these etiologies are associated with chronic inflammation, including local osteonecrosis, fibrosis, insufficient osteogenesis and angiogenesis, and tissue adipose infiltration. Therefore, studies of critical-sized bone defect healing models are relevant to the treatment of osteonecrotic lesions. Our laboratory and others have reviewed strategies and approaches to address these challenging clinical scenarios.
Inhibiting Chronic Inflammation
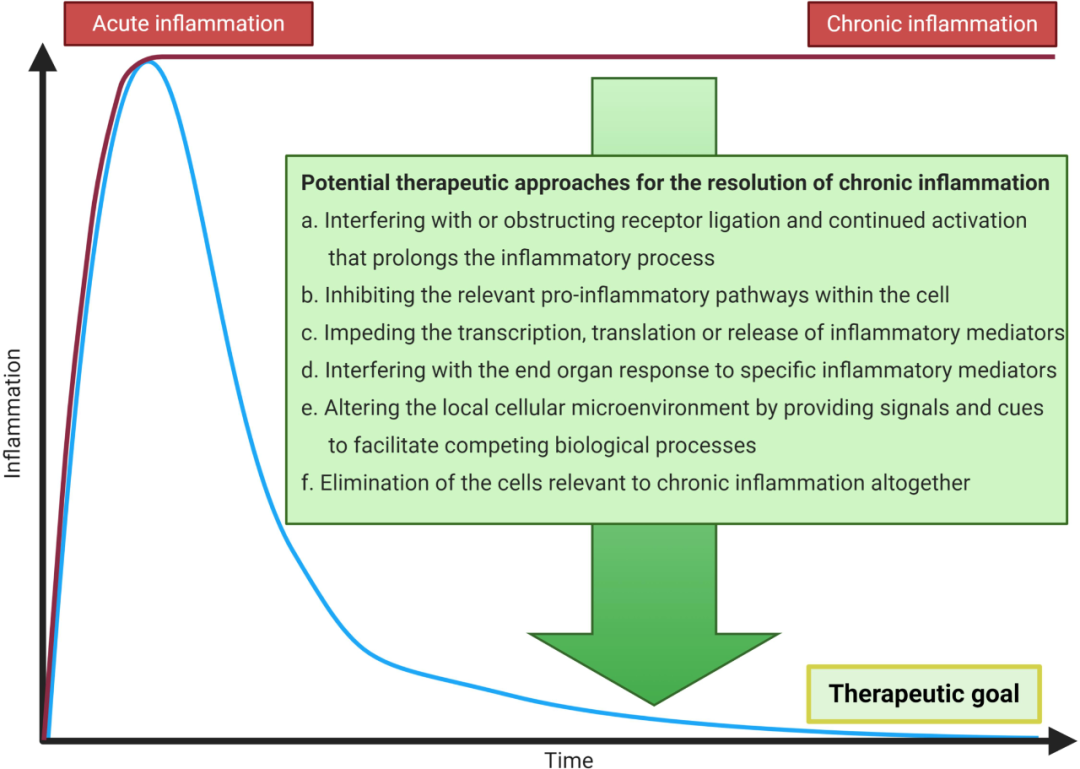
Given the association of osteonecrosis with chronic inflammation, it seems prudent to consider intervening in these processes. Potential therapeutic approaches must be time- and space-sensitive, as healing of soft and hard tissues after acute injury relies on acute inflammation for a short period (usually days), followed by the licensing of mesenchymal stem cells and other cells to initiate repair.
In light of these facts, the following are potential methods to alleviate chronic inflammation (Figure 2):
(a) Interfering with or obstructing receptor engagement and sustained activation that prolong the inflammatory process;
(b) Inhibiting intracellular pro-inflammatory pathways;
(c) Obstructing transcription, translation, or release of inflammatory mediators;
(d) Interfering with the response of end organs to specific inflammatory mediators;
(e) Promoting competing biological processes by providing signals and cues to alter the local cellular microenvironment;
(f) Completely eliminating cells associated with chronic inflammation.
Many of these strategies have been employed in the treatment of systemic chronic inflammatory diseases such as rheumatoid arthritis (RA). Pharmacological agents for RA include antimetabolites and other chemotherapeutic agents, disease-modifying drugs, and biologics that directly or indirectly interfere with specific cytokines, chemokines, and other pro-inflammatory molecules like tumor necrosis factor α (TNFα), interleukins (IL) such as IL-1β and IL-6. While these drugs are very effective for treating rheumatoid arthritis, it is impractical to administer these potentially serious side-effect-inducing drugs systemically for chronic inflammation due to osteonecrosis and significant bone defects. Therefore, local administration may be the preferred route. Regarding alleviating chronic inflammation associated with osteonecrosis and critical-sized bone defects, the following local methods show promise: inhibiting specific TLRs, especially TLR4; interfering with the following proteins: adaptor protein MyD88, transcription factor NF-кB, or chemokine MCP-1 and macrophage inhibitory factor (MIF); and polarizing macrophage states from M1 pro-inflammatory to M2 anti-inflammatory phenotypes through local delivery of IL-4 or IL-13. Our laboratory and others have used these strategies in models simulating chronic inflammation associated with wear particle disease.Infusion of IL-4 (an anti-inflammatory cytokine) is an important proposed strategy to suppress chronic inflammation in various clinical conditions. IL-4 protein can be delivered directly, via scaffolds or other devices, or through genetically modified mesenchymal stem cells overexpressing IL-4, which can also be upregulated via NF-кB. This approach is a significant direction in our laboratory for treating chronic bone defects and osteonecrosis. Other potential immunotherapeutic approaches include delivery of IL-13, IL-10, IL-1Ra, TNF receptor sR, etc.
Biomolecules and Drugs
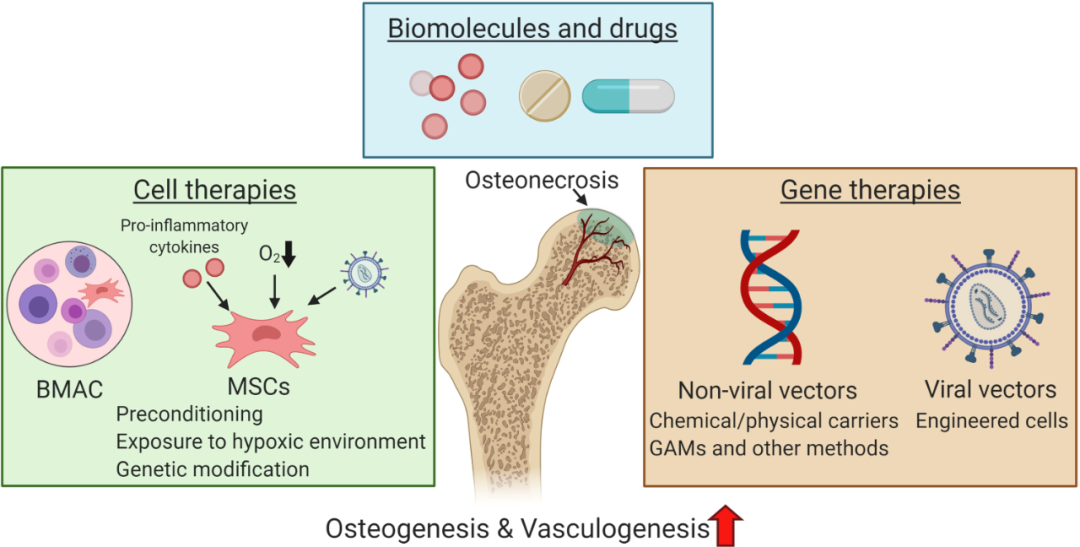
Local injection of growth factors and other molecules to enhance osteogenesis and angiogenesis, or to inhibit osteoclasts for the treatment of bone defects and osteonecrosis is not a new concept. These factors include members of the transforming growth factor (TGF) superfamily, including TGFβ and bone morphogenetic proteins (BMPs), fibroblast growth factor (FGF), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), hepatocyte growth factor, parathyroid hormone (PTH), etc. These reagents are delivered in the form of proteins embedded in various polymers, scaffolds, or matrices. These biomolecules serve as drug delivery systems that are absorbed, embedded, immobilized, or coated, and then released through diffusion, matrix degradation, or crosslinking. Other drugs for local delivery include corticosteroids and other steroids, statins, and bisphosphonates. These biomolecules are often multifunctional, regulating multiple pathways including inflammatory cascades, osteogenesis, and angiogenesis, and have other biological targets. While some of these interventions have been used in extensive preclinical and limited clinical studies for the treatment of bone defects, they are rarely used for the clinical treatment of osteonecrosis. In fact, clinical trials have not widely accepted and implemented systemic treatment with bisphosphonates or statins as effective for ONFH, but local treatments may be effective.The challenges of the harsh biological environment of necrotic, avascular bone lesions may be too high for successful drug therapies.
Cell Therapy
Gene Therapy

Summary


Discussion

This article represents the author’s personal views and does not reflect the official position of Bone Today. We hope everyone can make rational judgments and apply accordingly.
Submission Email: [email protected]