Introduction Multimodal monitoring of patients with severe traumatic brain injury (TBI) is primarily conducted in neurocritical care units to prevent secondary harmful brain injuries and facilitate patient recovery. Both invasive and non-invasive techniques are typically employed to monitor various parameters. The latest guidelines from the Brain Trauma Foundation in 2016 provide recommendations and thresholds for some of these parameters. Nevertheless, there remains a lack of high-level evidence for several parameters and thresholds. Methods In terms of invasive brain monitoring, intracranial pressure (ICP) is foundational, and pressures above 22 mmHg should be avoided. From ICP, cerebral perfusion pressure (CPP) (mean arterial pressure (MAP) – ICP) and pressure reactivity index (PRx) (the correlation between slow-wave MAP and ICP as an alternative indicator of cerebrovascular reactivity) can be derived. In local monitoring, brain tissue oxygen pressure (PbtO2) is commonly used, with ongoing Phase 3 studies to determine its additional impact on outcomes in conjunction with ICP monitoring. Cerebral microdialysis (CMD) is another regional invasive method for measuring substances in the brain extracellular fluid. The international consensus has proposed thresholds and management strategies, despite the lack of high-level evidence. While invasive monitoring is generally safe, approximately 10% of cases report iatrogenic hemorrhage, although such hemorrhages may not significantly affect long-term outcomes. Non-invasive monitoring is relatively new in the field of TBI treatment, with studies typically derived from single-center retrospective experiences. Near-infrared spectroscopy (NIRS) for measuring regional tissue saturation has been shown to correlate with outcomes. Transcranial Doppler (TCD) has several tentative practical applications in TBI, such as measuring ICP and detecting vasospasm. Additionally, continuous sampling of brain injury biomarkers in blood can be used to detect the development of secondary brain injury. Conclusion In multimodal monitoring, the most crucial aspect is data interpretation, which requires an understanding of the advantages and limitations of each parameter. A combination of several modalities may enable the identification of specific pathological states suitable for treatment. However, cost-effectiveness should consider the incremental benefits of adding several parameters, which currently have lower levels of evidence, thus warranting further research.
Introduction
Traumatic brain injury (TBI) is one of the most common causes of death and acquired disability worldwide, with the greatest burden borne by low- and middle-income countries. TBI is considered one of the most complex and heterogeneous diseases among the most complex organs, which is also one of the main reasons why all drug trials targeting the potential pathophysiology of TBI have not demonstrated efficacy to date. It is presumed that improving monitoring may be one of the best ways to discern specific pathological states that may be suitable for treatment, thus increasing the likelihood of success in future trials. In severe TBI, patients lose consciousness at the scene of injury or upon admission (typically assessed using the Glasgow Coma Scale (GCS), score <9), and standardized management protocols are recommended for admission to specialized neurocritical care units (NCCU). The primary goals are to mitigate the burden of secondary brain injury to optimize recovery. To facilitate this, organizations such as the Brain Trauma Foundation (BTF, the fourth iteration of guidelines released in 2017) and the Seattle International Consensus Conference on Severe Traumatic Brain Injury (SIBICC, starting in 2020) have provided frameworks for different monitoring modalities, levels of clinical evidence, and specified relevant thresholds and ranges. Despite the lack of higher-level evidence for efficacy, several monitoring modalities, including both invasive and non-invasive techniques, are commonly used in specific centers today, often in combination. This brief review will cover the most commonly used modalities, the current status of ongoing trials, and recommendations on how to optimize multimodal monitoring in severe TBI.
Invasive Monitoring
Intracranial Pressure
One of the cornerstones of neurosurgical intervention involves the Monro-Kellie doctrine, which posits that for the expansion of intracranial mass, compensation will occur (initially through the reduction of intracranial cerebrospinal fluid (CSF) and intracranial venous blood). Initially, the brain has considerable elasticity to accommodate volume increases, but as the intracranial mass increases, this compliance decreases, leading to incremental increases in ICP. If not treated promptly, these increases will result in brain herniation, including subfalcine and uncal herniation, which can lead to circulatory failure. The gold standard technique for measuring intracranial pressure is through external ventricular drainage (EVD); however, today, parenchymal monitoring devices (commonly abbreviated as ICPM, “ICP monitors”) are often used. Both techniques have their pros and cons; EVD is cheaper and has the potential to drain cerebrospinal fluid to treat elevated ICP (although ICP cannot be accurately measured at that time), although its risk profile is slightly higher. However, ICPM is easier to insert than EVD, which is sometimes done at the bedside in certain centers. While the initial EVD cannot simultaneously drain CSF and measure ICP, new pressure sensors in EVD or CSF pumps make this possible.
The BTF guidelines provide B-level evidence suggesting that the use of ICP monitoring information for the treatment of severe TBI patients is recommended to reduce mortality during hospitalization and in the two weeks post-injury, with ICP levels below 22 mmHg associated with good outcomes. Although a meta-analysis from 2010 showed improvements in both mortality and functional outcomes, elevated ICP is primarily associated with an increased risk of mortality following TBI.In 2012, the ICP monitoring paradigm was challenged when Randall Chesnut and his colleagues published a randomized trial of ICP monitoring in traumatic brain injury, which showed that the ICP monitoring group did not perform better in short- and long-term outcomes compared to the group managed by clinicians based on clinical and radiological results (benchmark evidence from the South American trial on the treatment of intracranial pressure (BEST:TRIP trial)).However, the real takeaway from BEST:TRIP, as proposed by Chesnut, is not that ICP monitoring is ineffective, but rather that if you know what you are doing, active ICP management is better than guessing, as monitoring reduces the number of ICP-lowering treatments given to each patient by half. Moreover, BEST:TRIP failed to show efficacy solely by comparing monitoring regimens, suggesting that additional monitoring modalities may be needed to improve outcomes. The results of BEST:TRIP have also been challenged by several experts in the field due to its efficacy issues and highlight the complexities of inferring results from healthcare systems in low- and middle-income countries to high-income countries.
Cerebral Perfusion Pressure (CPP) and Pressure Reactivity Index (PRx)
From ICP, other parameters can be derived, such as CPP (mean arterial pressure (MAP) – ICP) and PRx (the correlation between slow-wave MAP and ICP). CPP is the net pressure gradient leading to cerebral perfusion and is a common alternative indicator of cerebral blood flow, and it is typically managed by increasing MAP (in addition to lowering ICP). While there are differing schools of thought on how to manage CPP, the Lund concept advocates a more cautious approach (range of 50-70 mmHg), which is now recommended in the 2017 BTF and SIBICC guidelines to use a range of 60-70 mmHg, where levels above 70 mmHg are considered counterproductive, graded as Level II evidence (but it should be emphasized that the zero-level positions of MAP and ICP are critical). They also note that the patient’s autoregulatory capacity should be considered when determining the optimal CPP for the patient. PRx is an alternative indicator of cerebrovascular autoregulation, measured on a scale from 0 indicating complete autoregulation to 1 indicating complete inability to autoregulate blood flow. The BTF states that PRx >0.25 has been shown to be associated with mortality, and >0.05 is associated with adverse outcomes (Level II evidence). Similarly, recent studies emphasize that more than 50% of patients spend days in the ICU with impaired cerebral autoregulation, and during periods of controlled ICP and CPP, impaired autoregulation seems to dominate the manifestations of cerebral dysfunction in moderate/severe TBI. Additionally, data support the relative therapeutic independence of cerebral autoregulation from the guideline-based treatment approaches currently in TBI management, focusing our attention on strategies aimed at finding the “worst” state of cerebral autoregulation for specific patients. Joint work from Sweden and the UK suggests that patients with negative correlation PRx should adopt a CPP strategy, while those with positive correlation PRx should focus on lowering ICP to improve prognosis; thus, more modalities may assist management strategies. Furthermore, the lowest CPP of PRx is referred to as the “optimal CPP,” and in a recently published study, CPPOpt guiding treatment: Target Efficacy Assessment (COGITATE), a prospective study with n=30 was randomly assigned to CPP 60-70 mmHg and n=30 to personalized CPPopt targets; the authors demonstrated that CPPopt management is safe. Larger trials are needed to show clinical efficacy.Brain Tissue Local Oxygen Pressure (PbtO2) Local brain oxygen saturation can be measured through invasive catheters using different techniques to assess PbtO2 (sometimes referred to as PbrO2). The BTF indicates that Level II evidence suggests that PbtO2 < 29 mmHg increases the risk of mortality; Level III evidence suggests that levels below 15-20 mmHg are associated with adverse outcomes. Some PbtO2 monitors on the market also monitor brain temperature, which is important in itself as it differs from core temperature monitoring but has also been shown to affect intracranial dynamic changes. PbtO2 is becoming the second major monitoring parameter besides ICP, but there is little evidence regarding what it adds beyond ICP monitoring. However, in 2017, the Brain Tissue Oxygen Monitoring and Management in Severe Traumatic Brain Injury (BOOST-2) trial was published, showing that PbtO2 monitoring has adequate safety, and there was a trend towards improved outcomes in the PbtO2 + ICP cohort compared to the cohort using only ICP monitoring. These results led to refinements in treatment protocols and power calculations for the North American Phase III trial BOOST-3, which is currently underway to provide Level I evidence for PbtO2 + ICP monitoring efficacy. Other similar trials include the French OXY-TC trial and the Australian and New Zealand Brain Oxygen Neuro-monitoring Assessment (BONANZA) trial (ACTRN12619001328167), both of which use specified stratification algorithms to see whether these are better than isolated ICP monitoring based on the information from ICP and PbtO2. Similarly, the SIBICC guidelines have proposed appropriate treatment recommendations when combining ICP and PbtO2, defining specific TBI phenotypes based on multimodal monitoring according to existing evidence (Figure 1).
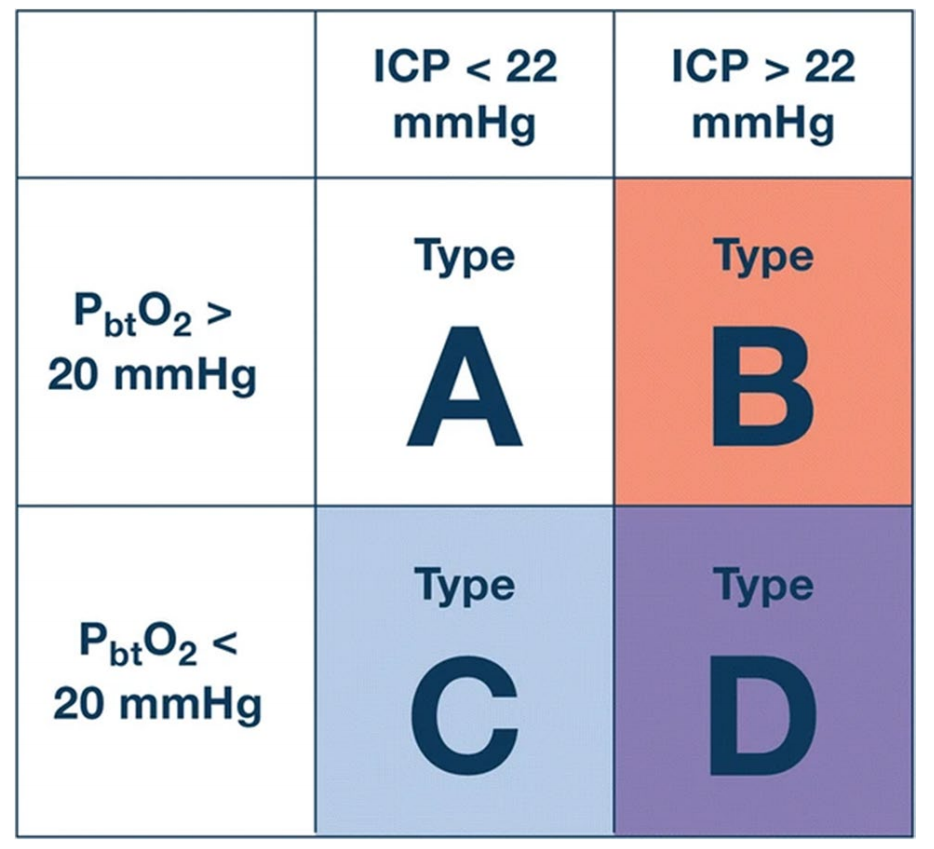
Figure 1 Examples of different definitions of TBI phenotypes based on multimodal monitoring using ICP and PbtO2. ICP intracranial pressure, PbtO2 brain tissue oxygen pressure.
Cerebral Microdialysis (CMD) CMD involves a catheter with a semipermeable membrane that is inserted into brain tissue and connected to a pump, allowing substances to flow into the tubing from the brain extracellular fluid (ECF) via osmosis. In severe traumatic shock, CMD is primarily used for bedside monitoring of metabolites using point-of-care devices. In the BTF, measuring glutamate with CMD (increased levels are associated with mortality compared to lower levels) is classified as Level III evidence, while there are several similar retrospective studies regarding thresholds for glucose, lactate, pyruvate, and lactate:pyruvate ratio (LPR). Research from the University of Cambridge in the UK has shown that LPR >25 is associated with metabolic disturbances in the brain, and when the brain suffers from high LPR, it also has low ECF glucose, low PbtO2, and impaired PRx. Similarly, research from Sweden combined LPR with glucose and pyruvate levels to create a “ischemic” state (high lactate and LPR, low pyruvate) and “mitochondrial dysfunction” (high lactate and LPR, although pyruvate levels are normal), and saw these were common across different traumatic diseases.Combination of Several Monitoring Modalities
In addition to the studies mentioned above, there are also regional centers that have combined ICP, PbtO2, and CMD monitoring over time and gained experience from it. One such center is Addenbrooke’s Hospital in Cambridge, UK, which published threshold recommendations for these parameters in 2017 (Table 1). Although not based on evidence beyond Level III, and without specific indications of what each added modality provides for additional monitoring or predictive capacity, they do provide guidance for centers using these monitoring modalities. Recently, this group published a paper that used an LPR-driven algorithm (if LPR >25) and adopted a tiered treatment approach, first correcting ICP (if above 20mmHg) (intracranial hypertension), then adjusting CPP (if PbtO2 <20mmHg) (oxygen delivery failure), and then increasing serum glucose to 10mmol/l when brain glucose <1.0mmol/l (neuroglycopenia). If no measures were taken to correct LPR, the patient was considered to have mitochondrial dysfunction. They then accurately mapped out which neuro-metabolic state (NMS) the patient was in during the first two weeks post-injury. Aside from normal LPR, the two most common NMS were mitochondrial dysfunction and neuroglycopenia, while intracranial hypertension and PbtO2 issues were rare. By categorizing patients into different NMS, targeted groups for mitochondrial dysfunction could also be specifically addressed. Such approaches could potentially lead to better monitoring in larger trials, targeting specific patient groups in the heterogeneous landscape of TBI, allowing for tailored treatment for each patient.
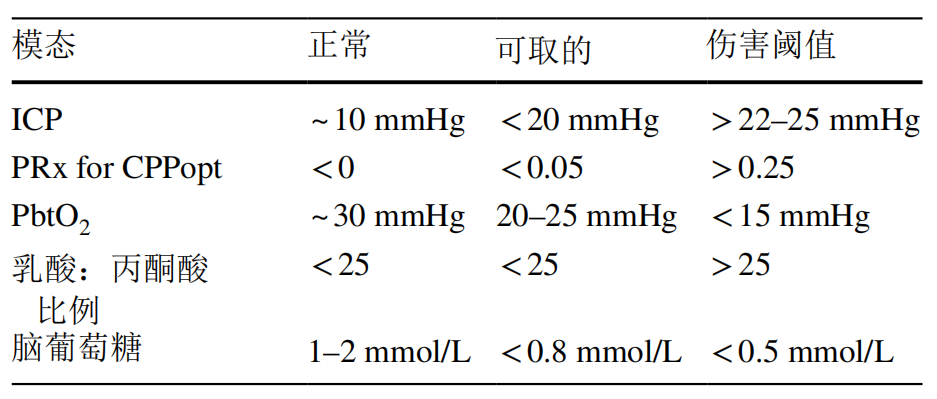
Table 1 Recommendations for multimodal monitoring using ICP, PbtO2, and CMD. Derived and modified from [28]. ICP intracranial pressure, PbtO2 brain tissue oxygen pressure, CMD cerebral microdialysis, PRx pressure reactivity index, CPPopt optimal cerebral perfusion pressure.
Risks and Difficulties of Invasive Brain Monitoring Invasive monitoring is not without risks. Tavakoli and colleagues reported in a review in 2017 an infection rate associated with EVD of about 10%, and ICPM of about 1%, with some studies showing bleeding after EVD insertion (although often subclinical) at about 30% (ICPM about 1%). In a recent study by Pease et al., they found that among 599 patients with severe traumatic brain injury, there was a 12% rate of bleeding and a 7% rate of CSF verification of infections caused by invasive monitoring. However, while patients with complications had longer hospital stays, there were no differences in outcomes at 6 months. Many catheter insertions also exceeded the manufacturer’s recommendations, typically 20 mm in the right frontal white matter, but the final range was between 9 and 42 mm. For this reason, bolting and other intracranial access devices are often used to prevent this by better securing the intracranial monitor. An example of this setup is shown (Figure 2).
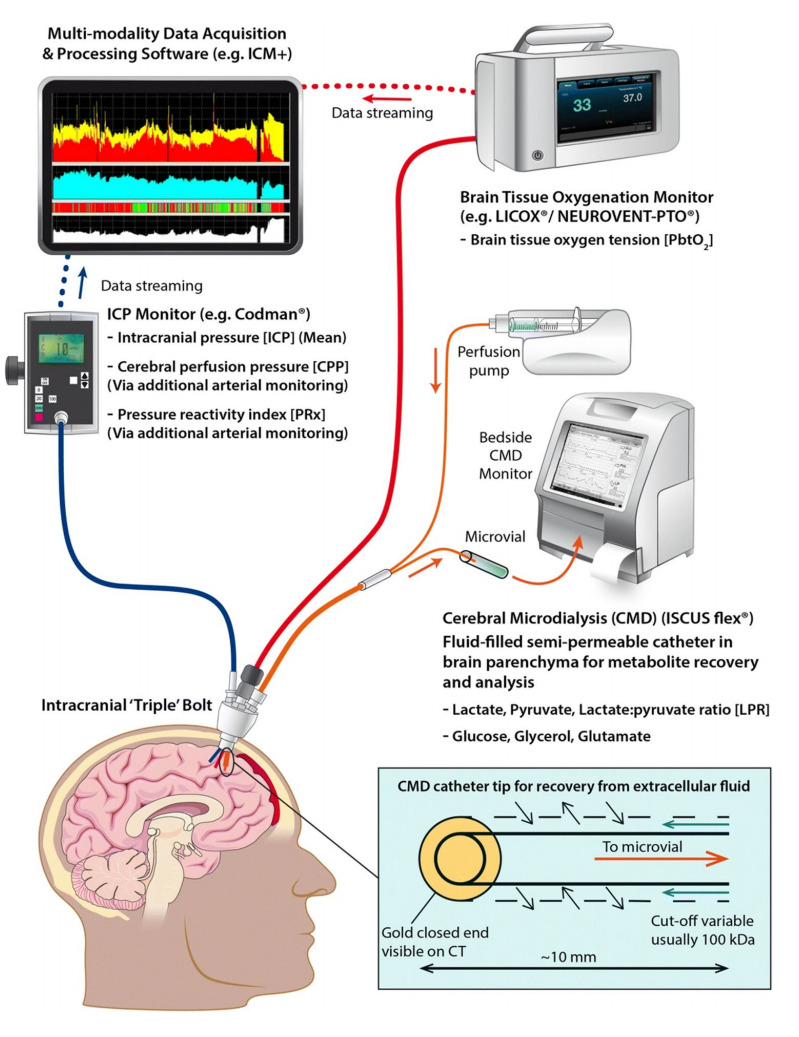
Figure 2 Invasive multimodal monitoring setup combining ICP, PbtO2, and CMD. ICP intracranial pressure, PbtO2 brain tissue oxygen pressure, CMD cerebral microdialysis, PRx pressure reactivity index, CPP cerebral perfusion pressure.
Another aspect of invasive monitoring involves the limitations of monitoring too small an area. It has been shown that when monitoring patients using three different CMD catheters, there are significant differences in lactate:pyruvate and glucose levels depending on the position of the catheter and the distance from the intracranial lesion. Similar issues exist with PbtO2, which shows lower levels when placed in abnormal tissue. While this is desirable as it allows monitoring of more vulnerable boundary areas and indicates deterioration more quickly, it also increases the complexity of multimodal monitoring in many cases, potentially further hindering more mainstream use. Therefore, while some centers target specific areas for regional monitoring, the goal of many centers is to assess healthier tissue to evaluate more “whole brain” measurements (the latest consensus on CMD monitoring also recommends this).
Non-invasive Monitoring
While invasive monitoring techniques are the gold standard in the field of TBI, non-invasive monitoring techniques exist. Compared to invasive techniques, they are generally cheaper, carry lower risks, and provide simpler methods, and as research progresses, they may replace some of the invasive techniques currently in use.
Near-Infrared Spectroscopy
Although the BTF guidelines do not support it, NIRS technology has been used since the 1970s to measure oxygenated hemoglobin. Regional hypoxia measured using continuous cranial NIRS has been shown to correlate with adverse outcomes, increased ICP, and low PbtO2, as shown in a systematic review from 2020. However, NIRS regional saturation has been shown to be affected by extracranial noise, which somewhat hinders its broader clinical application.
Transcranial Doppler
Currently, the latest BTF guidelines indicate that there is not enough evidence to recommend TCD monitoring. However, TCD monitoring has many different utilities after TBI, such as estimating flow velocity in vessels, like vasospasm and ICP. This method is relatively harmless through the use of ultrasound technology. Additionally, in many centers where invasive intracranial pressure monitoring cannot be performed, the assessment of the optic nerve sheath diameter (ONSD) can also serve as a substitute for ICP. One downside of TCD is that it is inherently intermittent and highly user-dependent; however, new robotic TCDs are being introduced and may facilitate this type of monitoring as a key advantage becomes the opportunity for user-independent longitudinal assessments for each patient.
Continuous Sampling of Brain Injury Protein Biomarkers
Protein biomarkers of tissue fate are currently used in several aspects of medicine and have also been introduced into TBI management. While most commonly used to screen mild TBI patients for lesions to rule out the need for computed tomography (CT), protein biomarkers can be continuously sampled to monitor the progression of lesions or the development of new injuries. The most studied blood biomarker is the astrocytic protein S100B. Other proteins studied in this context include neuron-specific enolase (NSE), glial fibrillary acidic protein (GFAP), tau, neurofilament light (NfL), and ubiquitin C-terminal hydrolase L1 (UCH-L1). Even a relatively modest increase in S100B (>0.05 μg/L) sampled every 12 hours has shown strong sensitivity and specificity for detecting imaging-visible lesions. Currently, blood biomarkers are not part of the BTF guidelines.
Other Issues Related to Neuro-monitoring
Cost
Costs associated with neuro-monitoring vary to some extent by center. However, considering only consumables, the cost of ICPM is about $500 per week (EVD about $200-300), while the cost of PbtO2 is about $1000, and CMD is about $700. Non-invasive monitoring is very cheap, with negligible consumable costs for techniques like TCD, while the cost of NIRS sensors is about $150 (for two bilateral sensors). Continuous sampling of S100B tests twice daily for a week costs about $300. It should be acknowledged that due to the heterogeneity of severe TBI and the lack of larger-scale trials, it is challenging to conduct sufficient cost-effectiveness analyses in this field. However, to justify the costs of using several monitoring modalities, particularly in cost-sensitive environments such as low- and middle-income countries, studies that clearly show additional benefits are warranted.
Interpretation of Monitoring Data
Although guidelines provided by the BTF and international consensus conferences on CMD monitoring offer thresholds for different parameters and metabolites, the dynamics of multimodal monitoring are often more complex. Trends and trajectories are often more relevant than absolute numbers, which are challenging to adequately describe in guidelines. Additionally, it is crucial to be able to trust the sensors, and many sensor placements, such as within a contusion or near the dura mater, may render CMD and PbtO2 measurements unreliable, thus complicating treatment guidance. Therefore, multimodal monitoring largely relies on quality control and different indirect tests, such as increasing the flow of oxygen (FiO2) to 100% to observe the response on PbtO2 to trust your monitor. In the future, artificial intelligence (AI) and various machine learning methods may assist in interpreting multimodal monitoring signals. Currently, this has been shown to improve dynamic predictions in patients using ICP monitoring, but it is still in its infancy when it comes to real-time integration of several modalities. However, the most important point is that merely inserting fancy and expensive monitoring devices does not improve the prognosis and management of TBI patients. Instead, it will be the staff and physicians in the NCCU who interpret and act on these changes to rapidly guide potential changes in diagnosis and management, and educational and training efforts are necessary to maintain adequate competency levels. So, what is the best combination of modalities? Should it combine invasive (such as ICP) and non-invasive (such as NIRS)? Should there be a regional (like CMD or PbtO2) and a global (like ICP or continuous S100B sampling)? One that is continuous (like ICP or PbtO2) and one that is intermittent (like TCD)? Given the lack of strong evidence supporting anything other than ICP monitoring, it could even be argued that the addition of several monitors should be determined by regional/center preference, conditions, and infrastructure. Typically, if a center is accustomed to using a set of modalities that may be less widely used globally, such as more outdated jugular bulb oxygen monitoring instead of PbtO2 monitoring, if that organization has experience in how to act and manage this information, it may be better for that specific center than other combinations.
Conclusion
While invasive ICP monitoring has long been the established gold standard for TBI monitoring, it cannot detect smaller lesions early, such as ischemic injuries. This is also one reason why centers around the world are increasingly adopting multimodal monitoring approaches using PbtO2 and/or CMD monitoring. Generally, the BEST-TRIP trial clearly indicates that more monitoring will inform us, so we do not have to guess who should be treated and when. Non-invasive technologies such as NIRS and TCD monitoring can partially replace some invasive monitoring, but more research is still needed. Currently, there is little evidence of additional benefits from using several monitoring modalities. However, several studies are underway to determine the role of PbtO2 + ICP. These types of studies will be able to discern specific pathological states in TBI that are susceptible to different types of treatment. Although there are currently no approved therapies targeting the fundamental pathophysiology of traumatic brain injury, multimodal monitoring will be a solution that provides better granularity regarding the processes of secondary injury, which can be addressed with more complex therapies in the future.Source:
Current state of high-fidelity multimodal monitoring in traumatic brain injury,
Acta Neurochirurgica
https://doi.org/10.1007/s00701-022-05383-8