Expert systems are computer intelligent program systems that can solve various complex problems by simulating the analysis process of specific experts in a particular field through reasoning technology. They mainly consist of four parts: knowledge acquisition module, knowledge base, inference engine module, and result interpreter. Since 2008, our laboratory has gradually developed and applied expert systems to manage data at 12 process nodes in the clinical microbiology laboratory. We found that the logical reasoning ability of the expert system is completely unaffected by work experience and work status. By inputting expert knowledge into the knowledge base and applying this knowledge to manage data at information nodes, the expert system is a very effective method for improving work efficiency and quality.
1. Design of Expert System Architecture
The architecture design of the clinical microbiology laboratory data management expert system is shown in Figure 1. The staff collects and organizes various published literature, including reference books, CLSI standards, guidelines, work experience, expert system rules from commercial identification systems, and laboratory operational procedures, and inputs expert knowledge into the expert knowledge base through the knowledge acquisition module. In daily work, the inference engine module of the expert system cross-verifies the data at various nodes in the clinical microbiology laboratory with the expert knowledge in the knowledge base. The reasoning results are displayed through the interpretation interface, including various warning messages and guidance for the next steps.
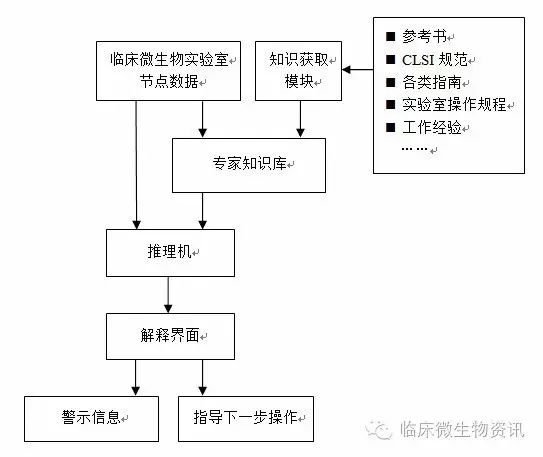 Figure 1 Architecture Design of Clinical Microbiology Laboratory Data Management Expert System
Figure 1 Architecture Design of Clinical Microbiology Laboratory Data Management Expert System
2. Application of Expert System
The expert system is applied to the workflow of the clinical microbiology laboratory, managing data at 12 process nodes from sample reception to test result reporting. The inference engine modules for managing data at the 12 different nodes vary, and the expert knowledge used and the final result interpretation methods are also different. The specifics are introduced as follows:
2.1 Application at Sample Reception Node:
① By comparing the current time with the specimen collection time, the expert system manages the sample submission duration. For example, it identifies the submission duration for cerebrospinal fluid bacterial culture specimens. If it exceeds the specified time, the expert system gives a warning message: “Sample submission time is too long.”
② By assessing the correlation between specimen type and test items, the expert system judges the rationality of the submission purpose. For example, for mid-stream urine specimens submitted for anaerobic bacteria culture, the system will determine it as unreasonable and provide guidance: “Suspected anaerobic infection of the urinary tract, suggest using bladder puncture for specimen collection.”
2.2 Application at Sample Information Collection and Input Node:
The expert system verifies and manages data collected through barcode scanning from the local area network, data obtained via QR code images, and manually entered data. For example, for a male patient with a specimen type of “vaginal secretion” and a female patient with a specimen type of “semen,” the expert system will issue a warning for “contradictory data.”
2.3 Application at Culture Medium Selection Node:
The expert system deduces the types of culture media required for bacterial culture based on the specimen type and test items, adding patient age and gender information. It automatically prints adhesive labels to be affixed to the corresponding culture media. The label information includes: unique specimen ID and barcode, specimen type name, patient name, gender, age, ward, bed number, etc., with the label size being 3 cm long and 2 cm wide.
This node’s expert knowledge mainly comes from the latest version of the “National Clinical Testing Operating Procedures.” For example, for bacterial culture of sputum specimens, it will automatically print labels for blood agar, MacConkey agar, chocolate agar, and original smear; for fecal specimens, it will print labels for MacConkey agar and SS agar. If it is a fecal specimen from a child with diarrhea, it will additionally print a label for a Sabouraud agar plate.
 Figure 2 Adhesive Labels
Figure 2 Adhesive Labels
2.4 Application at Bacterial Identification and Drug Sensitivity Operation Node:
The expert system infers based on the relevant data input in the electronic work record single node, guiding bacterial identification and drug sensitivity operations. Simultaneously, it verifies the manually entered or instrument-transmitted bacterial identification and drug sensitivity results against the data in the electronic work record single, issuing warnings for contradictory data.
① In guiding bacterial identification operations, for example, for Gram stain data indicating “fungal spores,” the inference engine module suggests: “Select [Candida tropicalis identification plate] for identification, and choose [ATB Candida drug sensitivity plate] for drug sensitivity.” For a specimen of “cerebrospinal fluid” with colony morphology of “umbonate” and alpha-hemolysis, and Gram stain indicating “positive cocci (in chains),” the module suggests: “Select [Siemens Streptococcus drug sensitivity plate].” If the user selects this suggestion, the inference engine module will automatically read specimen type, patient ID, name, age, etc., and generate a string compatible with the Siemens bacterial identification instrument’s two-way communication protocol, sending it to the Siemens instrument interface program.
② In verifying bacterial identification results, for example, if the identification result is “Escherichia coli” but the oxidase test is “positive,” the expert system will issue a warning: “Identification result is inconsistent with oxidase test.” For Gram stain indicating “negative bacilli” but having “fluconazole” in the drug sensitivity test, it will issue a warning: “Drug sensitivity test type error.”
2.5 Application at Drug Sensitivity Result Interpretation Node:
Based on expert knowledge from the CLSI “Standards for Performing Antimicrobial Susceptibility Testing,” the expert system identifies the antibiotic MIC values or inhibition zone diameters, bacterial names, and specimen sources entering this node against the breakpoint for drug sensitivity judgment in the expert knowledge base, ultimately providing interpretations of resistant, sensitive, or intermediate results, along with corresponding prompts.
For example, interpreting that the penicillin MIC for Streptococcus pneumoniae in a “cerebrospinal fluid” specimen is 0.5μg/ml as “resistant,” while interpreting the same MIC in a “sputum” specimen as “sensitive.” For the MIC of 1ug/ml for methicillin in Staphylococcus aureus, it is interpreted as “sensitive,” while for coagulase-negative Staphylococcus, it is interpreted as “resistant.” For Enterobacteriaceae against imipenem with an MIC of 1ug/ml, it is interpreted as “sensitive” and also provides a prompt: “Interpretation standard is based on a dosing regimen of 500mg every 6 hours or 1g every 8 hours.”
2.6 Application at Comprehensive Evaluation Node for Bacterial Identification and Drug Sensitivity Results:
The expert knowledge in this node’s knowledge base mainly comes from the CLSI “Standards for Performing Antimicrobial Susceptibility Testing” and references expert knowledge from commercial systems such as bioMérieux. In practical applications, the expert system performs logical judgments based on bacterial identification data and drug sensitivity data, along with patient-related data, focusing on four aspects:
① Verifying natural resistance in bacteria to determine if the experimental results are erroneous. For instance, in Enterobacteriaceae, Enterobacter cloacae is naturally resistant to cefoxitin, and Morganella morganii is naturally resistant to minocycline. If the expert system detects a “sensitive” result, it will issue a warning: “Natural resistance, please check if the test is correct?” requiring staff to input their account and password for confirmation.
② Identifying and prompting the need for re-examination of improbable or rare drug sensitivity results. For instance, resistance of Staphylococcus aureus to vancomycin and resistance of Escherichia coli to imipenem will prompt warnings such as “Rare result, suggest re-examination!”
③ Comprehensive analysis of specimen sources and drug sensitivity data can mask some drug sensitivity test reports. For example, chloramphenicol sensitivity in urinary isolates of Enterobacteriaceae is not routinely reported, so it must be masked on the report. For fosfomycin, reporting is only done for Escherichia coli isolated from the urinary tract; other strains must also be masked.
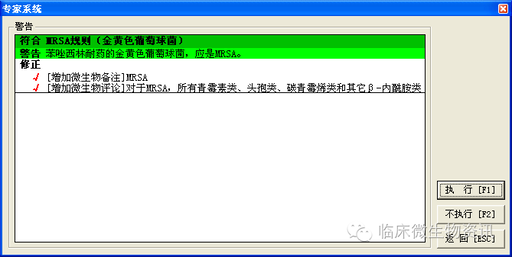
④ Comprehensive data analysis provides clinical treatment recommendations. For instance, for methicillin-resistant coagulase-negative Staphylococcus (MRS), the expert system will provide a report comment: “For MRS, β-lactam antibiotics such as penicillins, β-lactam/β-lactamase inhibitor combinations, cephalosporins, and carbapenems are clinically ineffective.”
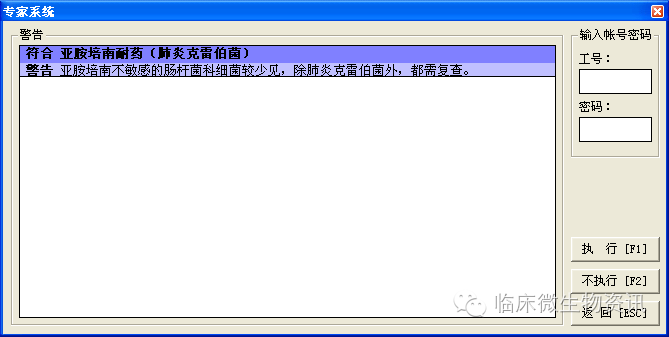 Figure 3 The expert system’s warning message requires staff to input their account and password for confirmation
Figure 3 The expert system’s warning message requires staff to input their account and password for confirmation
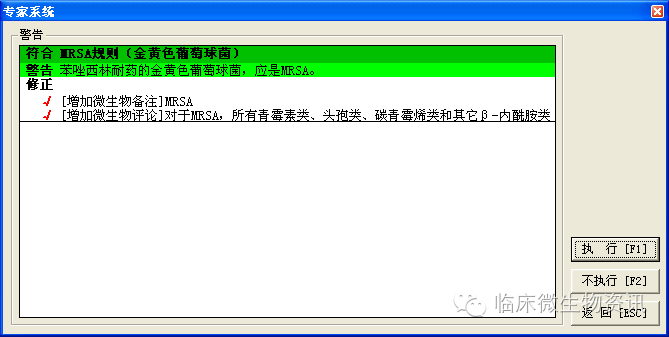 Figure 4 The expert system can add comments to the report
Figure 4 The expert system can add comments to the report
2.7 Application at Negative Result Reporting Node:
The expert system automatically provides the text for negative test results based on patient and specimen information. For example, for negative results from routine bacterial culture of feces, it will state: “No Salmonella or Shigella detected in culture.” For fecal cultures of Vibrio cholerae, it will state: “No Vibrio cholerae detected in culture,” as seen in Figure 5.
 Figure 5 The expert system can batch add text for negative test results
Figure 5 The expert system can batch add text for negative test results
2.8 Application at Positive Result Reporting Node:
The expert system compares positive test results (including detected pathogens and corresponding drug sensitivity data) with data from the laboratory over the past five years. If the positive result is not within the common probability range, it will provide a prompt.
For example, when managing the pathogen “Salmonella” detected in a patient’s respiratory specimen, the expert system will analyze and statistically evaluate the common pathogens in respiratory specimens over the past five years, finding that the “Salmonella” is not within the “common” range, thus issuing a warning, as seen in Figure 6.
For resistance results of Enterobacter cloacae against imipenem, the expert system will compare it with the resistance rates of Enterobacter cloacae against imipenem over the past five years. If the resistance rate is below 10%, the expert system will issue a warning: “Uncommon result.”
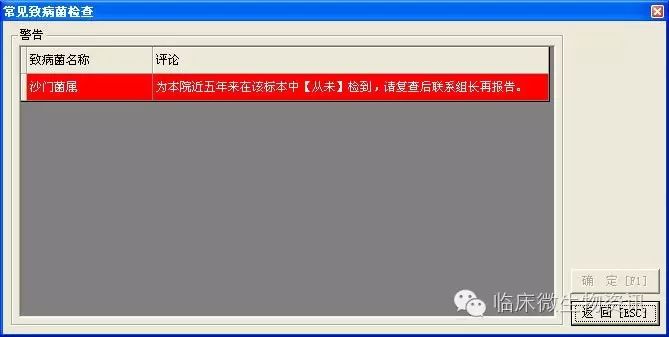 Figure 6 Warning given by the expert system when “Salmonella” is detected in respiratory specimens.
Figure 6 Warning given by the expert system when “Salmonella” is detected in respiratory specimens.
2.9 Application at Blood Culture Management Node:
The expert system manages the raw data collected from the blood culture instrument’s online interface program entering this node, focusing on four aspects:
① Management of negative results. The expert system dynamically detects the blood culture instrument’s judgment of blood bottle results. If a “negative” result is detected, it can directly initiate the negative result reporting procedure in the laboratory information management system.
② Management of instrument positive alarms. If a positive alarm information is detected during the night, the expert system can directly send a notification to the night shift personnel for positive blood bottle handling.
③ Management of graded blood culture reports. After staff performs Gram staining and microscopy on positive blood cultures, the expert system can automatically push preliminary report information to the clinical based on the specimen’s sending ward and doctor information.
④ Management of dual blood culture bottles. The expert system monitors the submission of dual blood culture bottles in real-time, issuing warnings if the submission ratio of dual bottles in any ward is too low.
2.10 Application at Mycoplasma Culture Node:
The data entering this node mainly comes from the image acquisition system for Ureaplasma and Mycoplasma identification and drug sensitivity testing plates. The expert system’s knowledge base sets specific position coordinates and color domain values for positive and negative judgments. The inference engine module of the expert system identifies the images of the detected testing plates, ultimately providing results for Ureaplasma and Mycoplasma culture and drug sensitivity, and issuing warnings for contradictory data. The interface of this functional module is shown in Figure 7.
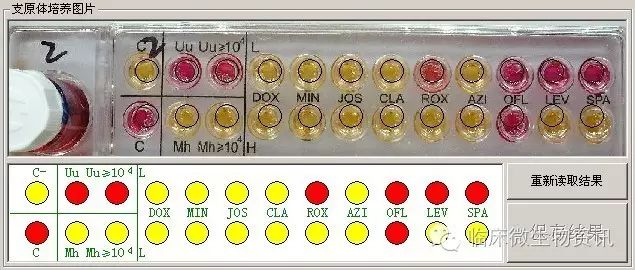 Figure 7 Automatic interpretation system interface for Ureaplasma and Mycoplasma culture and drug sensitivity results
Figure 7 Automatic interpretation system interface for Ureaplasma and Mycoplasma culture and drug sensitivity results
2.11 Application at Sample Testing Time Limit Management Node:
The expert system sets the expected reporting times for different specimens and testing items in the knowledge base through the knowledge acquisition module. During the expert system’s operation, it monitors the unapproved reports in the laboratory information management system in real-time and determines whether the expected reporting time has been exceeded.
If it has exceeded, the expert system checks whether there are operation records for that specimen in the “electronic work record single node” for that day. If not, it prompts the user to check that specimen to prevent missed reporting.
For example, if the expert system presets the reporting time for sputum bacterial culture as 2 days, and if no report is made after 2 days, and there are no records of “pure separation,” “machine operation,” or “re-examination” in the “electronic work record single node” for that day, it indicates that the specimen may have been forgotten. The expert system will prompt to check that specimen, as seen in Figure 8.
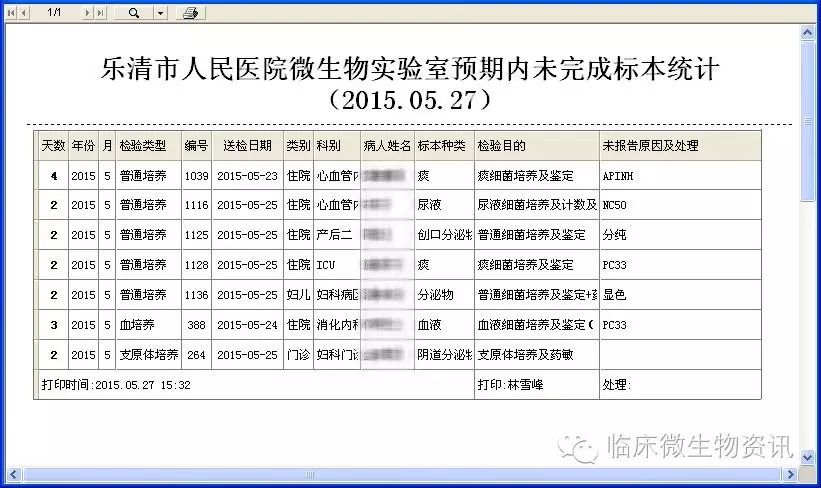 Figure 8 The expert system lists all specimens that have not been completed within the expected time to prevent omissions.
Figure 8 The expert system lists all specimens that have not been completed within the expected time to prevent omissions.
2.12 Application at Hospital Infection Indicator Management Node:
The expert system manages all data from issued reports. When it detects data related to methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, carbapenem-resistant Enterobacteriaceae, and multidrug-resistant Acinetobacter, it will prompt the user and guide them to send warning information to relevant departments via SMS or the hospital information management system.
3. Conclusion
The expert system is the most practical and widely used branch of artificial intelligence. It can infer and judge based on a considerable amount of authoritative knowledge and experience in a specific field, according to human experts’ logical thinking, and ultimately make intelligent decisions. It has broad applications in the medical field.
Research shows that in the complex business processes centered around “specimens” in clinical microbiology laboratories, data generation and transmission span multiple departments and positions within hospitals, taking three to seven days (or even longer, as in the case of Mycobacterium tuberculosis culture, which takes 84 days) from the application of analysis items to the use of analysis results. If data at any node in the process encounters issues, it directly leads to failures in the subsequent node operations using that data, affecting the overall operational efficiency of the clinical microbiology laboratory and, ultimately, clinical medical activities.
Establishing an expert system in the microbiology laboratory can utilize pre-recorded expert knowledge to reason about the data generated at each node of the clinical microbiology laboratory workflow, determining data validity or providing prompts for the next steps. This professional and efficient digital tool replaces manual management of massive and complex experimental data, marking an inevitable trend in laboratory digitalization. In this study, the expert system not only applies to common bacterial identification and drug sensitivity result interpretation nodes but also manages data at other workflow nodes in the clinical microbiology laboratory, such as verifying data at the sample reception node and sample information collection node, providing warnings for unreasonable data, reducing human errors, and improving work efficiency; pushing positive alarm information from the blood culture management node to allow timely processing of positive blood culture bottles, enabling early notification to clinical doctors for patient treatment; and real-time monitoring of various hospital infection indicators at the hospital infection indicator management node, promptly discovering and sending early warning information to relevant departments, allowing them to take timely measures to prevent hospital-acquired infections in other patients.
In summary, the establishment and application of the clinical microbiology laboratory data management expert system can reduce laboratory errors, improve work efficiency, and provide strong technical support for the overall improvement of laboratory management levels, better serving clinical and patients, effectively reducing patient hospitalization days and additional hospitalization costs, and creating safe medical activities.
Author: Lin Xuefeng (Yueqing Hospital Affiliated to Wenzhou Medical University)
Published in: Chinese Journal of Clinical Infectious Diseases, 2016, 9(2).
Please indicate the author and source when reprinting. Thank you.