
In recent years, the concept of acute gastrointestinal injury (AGI) has been proposed in the field of adult medicine abroad, emphasizing the graded definition and treatment of gastrointestinal function to protect the gastrointestinal function of critically ill patients and to prevent and treat gastrointestinal failure early.
Gastrointestinal dysfunction or failure is closely related to critical illness, which can be secondary to various critical diseases or be a component of multiple organ dysfunction syndrome (MODS), and can also be caused by diseases of the gastrointestinal mucosa or the digestive system itself. Gastrointestinal failure increases the mortality rate of critically ill patients and is an important factor affecting patient prognosis.
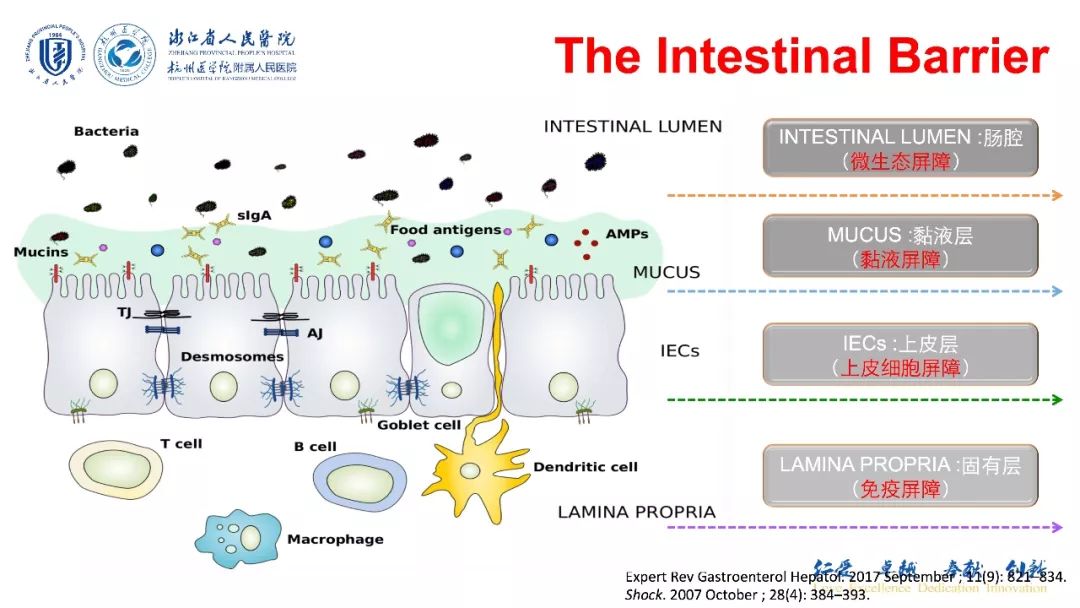
The intestine is one of the organs most affected early and severely in cases of severe infection, tissue hypoxia, and ischemia. In critical conditions, systemic inflammatory responses, capillary leakage, and large amounts of fluid exudation, as well as vascular dysfunction, can all affect the gastrointestinal organs.Research shows that gastrointestinal failure is not only a component of MODS but also a triggering factor for MODS.After gastrointestinal function is impaired, it affects the digestive and absorption functions of nutrients and water, the absorption and regulation of intestinal flora and its products, and subsequently impacts the endocrine and immune functions of the gastrointestinal system. Intestinal injury leads to a large number of bacterial translocations, causing enteric infections and enterogenic sepsis.
The common causes of gastrointestinal dysfunction in critical illness can be summarized as follows:
(1) Severe infectious diseases, such as severe sepsis, septic shock, severe pneumonia, severe intra-abdominal infections, pancreatitis, etc., caused by various pathogens like bacteria and viruses.
(2) Tissue hypoxia and ischemia caused by various reasons, such as asphyxia, acute respiratory distress syndrome, various shocks, poisoning, and post-cardiopulmonary resuscitation.
(3) Severe trauma or burns, cranial trauma or lesions, etc.
(4) Various syndromes related to systemic inflammatory responses, such as hemophagocytic syndrome, macrophage activation syndrome, MODS.
(5) Increased intra-abdominal pressure and abdominal compartment syndrome (ACS) due to various causes.
In 2012, the European Society of Intensive Care Medicine’s abdominal problems working group established and published recommendations for graded diagnosis and treatment of gastrointestinal function in critically ill patients based on evidence from clinical medicine, current understanding and research results regarding the pathophysiology of gastrointestinal failure, and expert opinions. Since the failure of any organ is a dynamic process, the occurrence of gastrointestinal failure is also the result of a gradual progression of the condition after injury, introducing the new concept of AGI and related terminology definitions, and recommending graded diagnosis and treatment of AGI.
1 Definition and Terminology
1.1 AGI
Refers to gastrointestinal dysfunction caused by the acute disease itself in critically ill patients. It is classified into four grades based on the severity of the condition, with objective indicators mainly based on the patient’s symptoms, such as visible bleeding in feces or gastric contents, lower gastrointestinal paralysis, feeding intolerance, nausea, vomiting, diarrhea, frequent bowel movements, bowel sounds, gastric retention, and incorporating intra-abdominal hypertension into the grading criteria. It is further divided into primary AGI and secondary AGI based on the etiology.
1.2 Primary AGI
Refers to AGI resulting from diseases or direct injuries originating in the gastrointestinal system, commonly seen in the early stages of gastrointestinal system injuries, such as peritonitis, pathological changes in the pancreas or liver, abdominal surgery, abdominal trauma, etc.
1.3 Secondary AGI
Refers to the body’s response to severe diseases without primary gastrointestinal diseases, such as occurring in pneumonia, cardiac diseases, non-abdominal surgeries or injuries, and post-cardiopulmonary resuscitation.
1.4 Feeding Intolerance Syndrome (FI)
Refers to enteral nutrition intolerance caused by any clinical reason (such as vomiting, diarrhea, gastrointestinal bleeding, enteric fistula, etc.). Its diagnosis is often based on complex clinical assessments, with no single clear symptoms or indicators to define it. When after 72 hours, the energy supply target of 20 kcal/(kg·d) cannot be achieved via enteral nutrition, or enteral nutrition is stopped for any clinical reason, FI should be considered, excluding reasons for clinical operation, etc.
1.5 Gastric Retention
Defined as a large amount of gastric retention if the single gastric fluid aspiration exceeds 200 ml.
1.6 Lower Gastrointestinal Paralysis (Paralytic Ileus)
Refers to impaired intestinal motility function, leading to an inability to expel feces. Clinical symptoms include cessation of bowel movements for at least 3 days, with bowel sounds present or absent, while excluding mechanical intestinal obstruction.
1.7 Intestinal Dilation
Diagnosed when abdominal X-ray or CT shows a colon diameter exceeding 6 cm (cecum exceeding 9 cm) or a small intestine diameter exceeding 3 cm.
1.8 Intra-abdominal Hypertension (IAH)
Refers to intra-abdominal pressure (IAP) ≥12 mmHg measured at least twice within 6 hours, with an average of at least 4 IAP measurements in one day not lower than 12 mmHg, IAH should also be considered.
1.9 ACS
Refers to sustained elevation of intra-abdominal pressure, with at least two IAP measurements exceeding 20 mmHg within 6 hours, and new organ dysfunction occurring.
The quantitative indicators in the above definitions or terminologies are based on adult standards; there are no pediatric standards for large gastric retention and intestinal dilation; regarding IAH, the diagnostic standards for children differ from adults: the diagnostic standard for IAH is persistent or recurrent IAP >10 mmHg; the IAH grading involved in the following AGI grading is IAH level I standard for children is IAP 10–15 mmHg, level II is the same as adults. The diagnostic standard for ACS is persistent IAP >10 mmHg, accompanied by new organ dysfunction or exacerbation of existing organ dysfunction due to increased IAP.
Grading and management of AGI
1 AGI Grade I (Presence of Risk Factors for Gastrointestinal Dysfunction and Failure)
Defined as having a clear etiology, with partial impairment of gastrointestinal function. It is characterized by temporary and self-limiting features. Clinically, it is often seen in nausea and vomiting after abdominal surgery and disappearance of bowel sounds; decreased intestinal motility in the early stages of shock.
Treatment Principles:
(1) Generally, the patient’s overall condition will gradually improve; except for intravenous administration of adequate fluids, no specific interventions for gastrointestinal symptoms are required.
(2) It is recommended to provide enteral nutrition as early as possible within 24–48 hours post-injury (Evidence Level 1B).
(3) Minimize the use of drugs that impair gastrointestinal motility, such as catecholamines and opioids (Evidence Level 1C).
2 AGI Grade II (Gastrointestinal Dysfunction)
Defined as impaired gastrointestinal digestion and absorption functions, unable to meet the body’s demands for nutrients and water, but not yet affecting the patient’s overall condition. It is characterized by acute gastrointestinal symptoms, requiring certain interventions to meet the body’s needs for nutrients and water. Clinically, it may present as gastroparesis with large gastric retention or reflux, lower gastrointestinal paralysis, diarrhea, IAH level I (IAP 12–15 mmHg), visible bleeding in gastric contents or feces, and food intolerance.
Treatment Principles:
Implement certain treatment measures to prevent progression to gastrointestinal failure. Treatment measures include:
(1) Treat IAH (Evidence Level 1D);
(2) Restore gastrointestinal motility, such as using prokinetic agents (Evidence Level 1C);
(3) Provide enteral nutrition; when there is large gastric retention or reflux, attempt to provide small amounts of enteral nutrition (Evidence Level 2D);
(4) In patients with gastroparesis where prokinetic agents are ineffective, consider providing post-pyloric nutrition (Evidence Level 2D).
3 AGI Grade III (Gastrointestinal Failure)
Defined as the loss of gastrointestinal function, with no recovery of gastrointestinal function after intervention, and no improvement in overall condition, such as persistent food intolerance despite aggressive treatment (e.g., erythromycin, placement of post-pyloric tube), and persistent or progressive multi-organ dysfunction. Clinically, it may present as large gastric retention, persistent gastrointestinal paralysis, intestinal dilation, intra-abdominal hypertension progressing to level II (IAP 16–20 mmHg), and decreased abdominal perfusion pressure (<60 mmHg).
Treatment Principles:
(1) Monitor and manage IAH (Evidence Level 1D).
(2) Exclude other intra-abdominal diseases, such as cholecystitis, peritonitis, intestinal ischemia. Discontinue any medications that may cause gastrointestinal paralysis as soon as possible (Evidence Level 1C).
(3) Avoid early parenteral nutrition (within 7 days prior to ICU admission) to reduce the incidence of hospital-acquired infections (Evidence Level 2B).
(4) Routine attempts to provide small amounts of enteral nutrition should be made (Evidence Level 2D).
4 AGI Grade IV (Gastrointestinal Failure with Distant Organ Dysfunction)
Defined as AGI progressing to a life-threatening state, with the patient experiencing worsening MODS and shock, posing an imminent life threat. The patient’s overall condition deteriorates sharply, accompanied by distant organ dysfunction, such as intestinal ischemia and necrosis, gastrointestinal bleeding leading to hemorrhagic shock, Ogilvie’s syndrome (acute colonic pseudo-obstruction), and ACS requiring urgent decompression.
Treatment Principles:Emergency laparotomy or other emergency interventions (e.g., colonoscopic decompression) (Evidence Level 1D).

Long press to recognize the QR code to follow us

We are dedicated to providing you with critical care information, a platform with warmth.